- Global Issues
- Community Projects
- Creative Writing
- Storytelling
- Problem-Solving Method
- Real World Issues
- Future Scenarios
- Authentic Assessments
- 5Cs of Learning
- Youth Protection
- DEIB Commitment
- International Conference
- Find FPS Near Me
- Partner With Us

Food Security
How might food security issues of availability, access, and affordability essential for living a healthy life impact society in the future?

Rising Sea Levels
How might we address the impact of rising sea levels on coastlines, industries, and people in the future?

Agricultural Industry
How might the agricultural industry adapt to the needs of feeding a growing world population in the future?

Nanotechnology
How might the use of nanotechnology in medicine, healthcare, and other industries affect humanity in the future?

The full list of 50+ years of solving real world challenges
See a comprehensive list of all the Future Problem Solving competition topics from 1974 to today.

Air Quality
How will the quality of air, a globally shared resource essential for human health and prosperity, impact us in the future?

Changing with the times: environmental sustainability issues
See how Future Problem Solving environment topic-related challenges evolved through the decades.

Artificial Intelligence (AI)
How will the emerging uses of artificial intelligence (AI) impact how we work, live, play, and learn in the future?
Have a topic idea?
Featured articles.

Future Problem Solving Students – A Five Year Study
A comparison of reading and mathematics performance between students participating in a future problem solving program and nonparticipants.
Data from the The Minnesota Comprehensive Assessment (MCA) was collected by Grandview Middle School and provided to Scholastic Testing Service, Inc. for statistical analysis.
Findings reported by Scholastic Testing Service, Inc. Performance data on the MCA was collected from 2010-2014 for students in grade 6 at Grandview Middle School in Mound, MN (Westonka Public School District). Students were identified as either FPS: students participating in a Future Problem Solving program, or Non-FPS: students not participating in the program. Summary statistics using Reading and Mathematics Scaled Scores were developed for each group of students by year and across years. To determine if the mean scores across the years were significantly different, t-tests were used. A Cohen’s d test was then performed to measure the effect of the size of the found differences.
In all cases, students participating in the Future Problem Solving Program performed significantly higher on the MCA in both areas of Mathematics and Reading.
Effects of Group Training in Problem-Solving Style on Future Problem-Solving Performance
The journal of creative behavior (jcb) of the creative education foundation.
Seventy-five participants from one suburban high school formed 21 teams with 3–4 members each for Future Problem Solving (FPS). Students were selected to participate in either the regular FPS or an enhanced FPS, where multiple group training activities grounded in problem-solving style were incorporated into a 9-week treatment period.
An ANCOVA procedure was used to examine the difference in team responses to a creative problem-solving scenario for members of each group, after accounting for initial differences in creative problem-solving performance, years of experience in FPS, and creative thinking related to fluency, flexibility, and originality. The ANCOVA resulted in a significant difference in problem-solving performance in favor of students in the treatment group (F(1, 57) = 8.21, p = .006, partial eta squared = .126, medium), while there were no significant differences in years of experience or creativity scores. This result led researchers to conclude that students in both groups had equivalent creative ability and that participation in the group activities emphasizing problem-solving style significantly contributed to creative performance.
In the comparison group, a total of 47% had scores that qualified for entry to the state competition. In contrast, 89% of the students in the treatment group had scores that qualified them for the state bowl. None of the teams from the comparison group qualified for the international competition, while two teams from the treatment group were selected, with one earning sixth place.
The results of this study suggest that problem-solving performance by team members can be improved through direct instruction in problem-solving style, particularly when there is a focus on group dynamics.
The Journal of Creative Behavior, Vol. 0, Iss. 0, pp. 1–12 © 2017 by the Creative Education Foundation, Inc. DOI: 10.1002/jocb.176
Future Problem Solving Program International—Second Generation Study
“how important was future problem solving in the development of your following skill sets”.
In 2011, a team of researchers from the University of Virginia submitted a report titled “Future Problem Solving Program International—Second Generation Study.” (Callahan, Alimin, & Uguz, 2012). The study, based on a survey, collected data from over 150 Future Problem Solving alumni to understand the impact of their participation in Future Problem Solving as students or volunteers.
Percentage of Alumni Rating Important and Extremely Important in Developing Skill Sets
- 96% Look at the “Big Picture”
- 93% Critical Thinking
- 93% Teamwork and Collaboration
- 93% Identify and Solve Problems
- 93% Time Management
- 90% Researching
- 90% Evaluation and Decision Making
- 86% Creativity and Innovation
- 86% Written Communication
The report captured alumni’s positive experiences as students in Future Problem Solving and documented that the alumni continued to utilize the FPS-structured approach to solving problems in their adult lives.
Executive Director
A seasoned educator, April Michele has served as the Executive Director since 2018 and been with Future Problem Solving more than a decade. Her background in advanced curriculum strategies and highly engaging learning techniques translates well in the development of materials, publications, training, and marketing for the organization and its global network. April’s expertise includes pedagogy and strategies for critical and creative thinking and providing quality educational services for students and adults worldwide.
Prior to joining Future Problem Solving, April taught elementary and middle grades, spending most of her classroom career in gifted education. She earned the National Board certification (NBPTS) as a Middle Childhood/Generalist and later served as a National Board assessor for the certification of others. In addition, April facilitated the Theory and Development of Creativity course for the state of Florida’s certification of teachers. She has also collaborated on a variety of special projects through the Department of Education. Beyond her U.S. education credentials, she has been trained for the International Baccalaureate Middle Years Programme (MYP) in Humanities.
A graduate of the University of Central Florida with a bachelor’s in Elementary Education and the University of South Florida with a master’s in Gifted Education, April’s passion is providing a challenging curriculum for 21st century students so they are equipped with the problem-solving and ethical leadership skills they need to thrive in the future. As a board member in her local Rotary Club, she facilitates problem solving in leadership at the Rotary Youth Leadership Awards (RYLA). She is also a certified Project Management Professional (PMP) from the Project Management Institute and earned her certificate in Nonprofit Management from the Edyth Bush Institute at Rollins College.

How it works
Transform your enterprise with the scalable mindsets, skills, & behavior change that drive performance.
Explore how BetterUp connects to your core business systems.
We pair AI with the latest in human-centered coaching to drive powerful, lasting learning and behavior change.
Build leaders that accelerate team performance and engagement.
Unlock performance potential at scale with AI-powered curated growth journeys.
Build resilience, well-being and agility to drive performance across your entire enterprise.
Transform your business, starting with your sales leaders.
Unlock business impact from the top with executive coaching.
Foster a culture of inclusion and belonging.
Accelerate the performance and potential of your agencies and employees.
See how innovative organizations use BetterUp to build a thriving workforce.
Discover how BetterUp measurably impacts key business outcomes for organizations like yours.
A demo is the first step to transforming your business. Meet with us to develop a plan for attaining your goals.

- What is coaching?
Learn how 1:1 coaching works, who its for, and if it's right for you.
Accelerate your personal and professional growth with the expert guidance of a BetterUp Coach.
Types of Coaching
Navigate career transitions, accelerate your professional growth, and achieve your career goals with expert coaching.
Enhance your communication skills for better personal and professional relationships, with tailored coaching that focuses on your needs.
Find balance, resilience, and well-being in all areas of your life with holistic coaching designed to empower you.
Discover your perfect match : Take our 5-minute assessment and let us pair you with one of our top Coaches tailored just for you.

Research, expert insights, and resources to develop courageous leaders within your organization.
Best practices, research, and tools to fuel individual and business growth.
View on-demand BetterUp events and learn about upcoming live discussions.
The latest insights and ideas for building a high-performing workplace.
- BetterUp Briefing
The online magazine that helps you understand tomorrow's workforce trends, today.
Innovative research featured in peer-reviewed journals, press, and more.
Founded in 2022 to deepen the understanding of the intersection of well-being, purpose, and performance
We're on a mission to help everyone live with clarity, purpose, and passion.
Join us and create impactful change.
Read the buzz about BetterUp.
Meet the leadership that's passionate about empowering your workforce.
For Business
For Individuals
10 Problem-solving strategies to turn challenges on their head

Jump to section
What is an example of problem-solving?
What are the 5 steps to problem-solving, 10 effective problem-solving strategies, what skills do efficient problem solvers have, how to improve your problem-solving skills.
Problems come in all shapes and sizes — from workplace conflict to budget cuts.
Creative problem-solving is one of the most in-demand skills in all roles and industries. It can boost an organization’s human capital and give it a competitive edge.
Problem-solving strategies are ways of approaching problems that can help you look beyond the obvious answers and find the best solution to your problem .
Let’s take a look at a five-step problem-solving process and how to combine it with proven problem-solving strategies. This will give you the tools and skills to solve even your most complex problems.
Good problem-solving is an essential part of the decision-making process . To see what a problem-solving process might look like in real life, let’s take a common problem for SaaS brands — decreasing customer churn rates.
To solve this problem, the company must first identify it. In this case, the problem is that the churn rate is too high.
Next, they need to identify the root causes of the problem. This could be anything from their customer service experience to their email marketing campaigns. If there are several problems, they will need a separate problem-solving process for each one.
Let’s say the problem is with email marketing — they’re not nurturing existing customers. Now that they’ve identified the problem, they can start using problem-solving strategies to look for solutions.
This might look like coming up with special offers, discounts, or bonuses for existing customers. They need to find ways to remind them to use their products and services while providing added value. This will encourage customers to keep paying their monthly subscriptions.
They might also want to add incentives, such as access to a premium service at no extra cost after 12 months of membership. They could publish blog posts that help their customers solve common problems and share them as an email newsletter.
The company should set targets and a time frame in which to achieve them. This will allow leaders to measure progress and identify which actions yield the best results.

Perhaps you’ve got a problem you need to tackle. Or maybe you want to be prepared the next time one arises. Either way, it’s a good idea to get familiar with the five steps of problem-solving.
Use this step-by-step problem-solving method with the strategies in the following section to find possible solutions to your problem.
1. Identify the problem
The first step is to know which problem you need to solve. Then, you need to find the root cause of the problem.
The best course of action is to gather as much data as possible, speak to the people involved, and separate facts from opinions.
Once this is done, formulate a statement that describes the problem. Use rational persuasion to make sure your team agrees .
2. Break the problem down
Identifying the problem allows you to see which steps need to be taken to solve it.
First, break the problem down into achievable blocks. Then, use strategic planning to set a time frame in which to solve the problem and establish a timeline for the completion of each stage.
3. Generate potential solutions
At this stage, the aim isn’t to evaluate possible solutions but to generate as many ideas as possible.
Encourage your team to use creative thinking and be patient — the best solution may not be the first or most obvious one.
Use one or more of the different strategies in the following section to help come up with solutions — the more creative, the better.
4. Evaluate the possible solutions
Once you’ve generated potential solutions, narrow them down to a shortlist. Then, evaluate the options on your shortlist.
There are usually many factors to consider. So when evaluating a solution, ask yourself the following questions:
- Will my team be on board with the proposition?
- Does the solution align with organizational goals ?
- Is the solution likely to achieve the desired outcomes?
- Is the solution realistic and possible with current resources and constraints?
- Will the solution solve the problem without causing additional unintended problems?

5. Implement and monitor the solutions
Once you’ve identified your solution and got buy-in from your team, it’s time to implement it.
But the work doesn’t stop there. You need to monitor your solution to see whether it actually solves your problem.
Request regular feedback from the team members involved and have a monitoring and evaluation plan in place to measure progress.
If the solution doesn’t achieve your desired results, start this step-by-step process again.
There are many different ways to approach problem-solving. Each is suitable for different types of problems.
The most appropriate problem-solving techniques will depend on your specific problem. You may need to experiment with several strategies before you find a workable solution.
Here are 10 effective problem-solving strategies for you to try:
- Use a solution that worked before
- Brainstorming
- Work backward
- Use the Kipling method
- Draw the problem
- Use trial and error
- Sleep on it
- Get advice from your peers
- Use the Pareto principle
- Add successful solutions to your toolkit
Let’s break each of these down.
1. Use a solution that worked before
It might seem obvious, but if you’ve faced similar problems in the past, look back to what worked then. See if any of the solutions could apply to your current situation and, if so, replicate them.
2. Brainstorming
The more people you enlist to help solve the problem, the more potential solutions you can come up with.
Use different brainstorming techniques to workshop potential solutions with your team. They’ll likely bring something you haven’t thought of to the table.
3. Work backward
Working backward is a way to reverse engineer your problem. Imagine your problem has been solved, and make that the starting point.
Then, retrace your steps back to where you are now. This can help you see which course of action may be most effective.
4. Use the Kipling method
This is a method that poses six questions based on Rudyard Kipling’s poem, “ I Keep Six Honest Serving Men .”
- What is the problem?
- Why is the problem important?
- When did the problem arise, and when does it need to be solved?
- How did the problem happen?
- Where is the problem occurring?
- Who does the problem affect?
Answering these questions can help you identify possible solutions.
5. Draw the problem
Sometimes it can be difficult to visualize all the components and moving parts of a problem and its solution. Drawing a diagram can help.
This technique is particularly helpful for solving process-related problems. For example, a product development team might want to decrease the time they take to fix bugs and create new iterations. Drawing the processes involved can help you see where improvements can be made.

6. Use trial-and-error
A trial-and-error approach can be useful when you have several possible solutions and want to test them to see which one works best.
7. Sleep on it
Finding the best solution to a problem is a process. Remember to take breaks and get enough rest . Sometimes, a walk around the block can bring inspiration, but you should sleep on it if possible.
A good night’s sleep helps us find creative solutions to problems. This is because when you sleep, your brain sorts through the day’s events and stores them as memories. This enables you to process your ideas at a subconscious level.
If possible, give yourself a few days to develop and analyze possible solutions. You may find you have greater clarity after sleeping on it. Your mind will also be fresh, so you’ll be able to make better decisions.
8. Get advice from your peers
Getting input from a group of people can help you find solutions you may not have thought of on your own.
For solo entrepreneurs or freelancers, this might look like hiring a coach or mentor or joining a mastermind group.
For leaders , it might be consulting other members of the leadership team or working with a business coach .
It’s important to recognize you might not have all the skills, experience, or knowledge necessary to find a solution alone.
9. Use the Pareto principle
The Pareto principle — also known as the 80/20 rule — can help you identify possible root causes and potential solutions for your problems.
Although it’s not a mathematical law, it’s a principle found throughout many aspects of business and life. For example, 20% of the sales reps in a company might close 80% of the sales.
You may be able to narrow down the causes of your problem by applying the Pareto principle. This can also help you identify the most appropriate solutions.
10. Add successful solutions to your toolkit
Every situation is different, and the same solutions might not always work. But by keeping a record of successful problem-solving strategies, you can build up a solutions toolkit.
These solutions may be applicable to future problems. Even if not, they may save you some of the time and work needed to come up with a new solution.

Improving problem-solving skills is essential for professional development — both yours and your team’s. Here are some of the key skills of effective problem solvers:
- Critical thinking and analytical skills
- Communication skills , including active listening
- Decision-making
- Planning and prioritization
- Emotional intelligence , including empathy and emotional regulation
- Time management
- Data analysis
- Research skills
- Project management
And they see problems as opportunities. Everyone is born with problem-solving skills. But accessing these abilities depends on how we view problems. Effective problem-solvers see problems as opportunities to learn and improve.
Ready to work on your problem-solving abilities? Get started with these seven tips.
1. Build your problem-solving skills
One of the best ways to improve your problem-solving skills is to learn from experts. Consider enrolling in organizational training , shadowing a mentor , or working with a coach .
2. Practice
Practice using your new problem-solving skills by applying them to smaller problems you might encounter in your daily life.
Alternatively, imagine problematic scenarios that might arise at work and use problem-solving strategies to find hypothetical solutions.
3. Don’t try to find a solution right away
Often, the first solution you think of to solve a problem isn’t the most appropriate or effective.
Instead of thinking on the spot, give yourself time and use one or more of the problem-solving strategies above to activate your creative thinking.

4. Ask for feedback
Receiving feedback is always important for learning and growth. Your perception of your problem-solving skills may be different from that of your colleagues. They can provide insights that help you improve.
5. Learn new approaches and methodologies
There are entire books written about problem-solving methodologies if you want to take a deep dive into the subject.
We recommend starting with “ Fixed — How to Perfect the Fine Art of Problem Solving ” by Amy E. Herman.
6. Experiment
Tried-and-tested problem-solving techniques can be useful. However, they don’t teach you how to innovate and develop your own problem-solving approaches.
Sometimes, an unconventional approach can lead to the development of a brilliant new idea or strategy. So don’t be afraid to suggest your most “out there” ideas.
7. Analyze the success of your competitors
Do you have competitors who have already solved the problem you’re facing? Look at what they did, and work backward to solve your own problem.
For example, Netflix started in the 1990s as a DVD mail-rental company. Its main competitor at the time was Blockbuster.
But when streaming became the norm in the early 2000s, both companies faced a crisis. Netflix innovated, unveiling its streaming service in 2007.
If Blockbuster had followed Netflix’s example, it might have survived. Instead, it declared bankruptcy in 2010.
Use problem-solving strategies to uplevel your business
When facing a problem, it’s worth taking the time to find the right solution.
Otherwise, we risk either running away from our problems or headlong into solutions. When we do this, we might miss out on other, better options.
Use the problem-solving strategies outlined above to find innovative solutions to your business’ most perplexing problems.
If you’re ready to take problem-solving to the next level, request a demo with BetterUp . Our expert coaches specialize in helping teams develop and implement strategies that work.
Boost your productivity
Maximize your time and productivity with strategies from our expert coaches.
Elizabeth Perry, ACC
Elizabeth Perry is a Coach Community Manager at BetterUp. She uses strategic engagement strategies to cultivate a learning community across a global network of Coaches through in-person and virtual experiences, technology-enabled platforms, and strategic coaching industry partnerships. With over 3 years of coaching experience and a certification in transformative leadership and life coaching from Sofia University, Elizabeth leverages transpersonal psychology expertise to help coaches and clients gain awareness of their behavioral and thought patterns, discover their purpose and passions, and elevate their potential. She is a lifelong student of psychology, personal growth, and human potential as well as an ICF-certified ACC transpersonal life and leadership Coach.
8 creative solutions to your most challenging problems
5 problem-solving questions to prepare you for your next interview, what are metacognitive skills examples in everyday life, what is lateral thinking 7 techniques to encourage creative ideas, 31 examples of problem solving performance review phrases, leadership activities that encourage employee engagement, learn what process mapping is and how to create one (+ examples), how much do distractions cost 8 effects of lack of focus, can dreams help you solve problems 6 ways to try, similar articles, the pareto principle: how the 80/20 rule can help you do more with less, thinking outside the box: 8 ways to become a creative problem solver, 3 problem statement examples and steps to write your own, what is tacit knowledge, and how does it benefit the workplace, contingency planning: 4 steps to prepare for the unexpected, stay connected with betterup, get our newsletter, event invites, plus product insights and research..
3100 E 5th Street, Suite 350 Austin, TX 78702
- Platform Overview
- Integrations
- Powered by AI
- BetterUp Lead™
- BetterUp Manage™
- BetterUp Care®
- Sales Performance
- Diversity & Inclusion
- Case Studies
- Why BetterUp?
- About Coaching
- Find your Coach
- Career Coaching
- Communication Coaching
- Life Coaching
- News and Press
- Leadership Team
- Become a BetterUp Coach
- BetterUp Labs
- Center for Purpose & Performance
- Leadership Training
- Business Coaching
- Contact Support
- Contact Sales
- Privacy Policy
- Acceptable Use Policy
- Trust & Security
- Cookie Preferences
- Bipolar Disorder
- Therapy Center
- When To See a Therapist
- Types of Therapy
- Best Online Therapy
- Best Couples Therapy
- Best Family Therapy
- Managing Stress
- Sleep and Dreaming
- Understanding Emotions
- Self-Improvement
- Healthy Relationships
- Student Resources
- Personality Types
- Guided Meditations
- Verywell Mind Insights
- 2024 Verywell Mind 25
- Mental Health in the Classroom
- Editorial Process
- Meet Our Review Board
- Crisis Support
Overview of the Problem-Solving Mental Process
Kendra Cherry, MS, is a psychosocial rehabilitation specialist, psychology educator, and author of the "Everything Psychology Book."
:max_bytes(150000):strip_icc():format(webp)/IMG_9791-89504ab694d54b66bbd72cb84ffb860e.jpg "problem solving 2022")
Rachel Goldman, PhD FTOS, is a licensed psychologist, clinical assistant professor, speaker, wellness expert specializing in eating behaviors, stress management, and health behavior change.
:max_bytes(150000):strip_icc():format(webp)/Rachel-Goldman-1000-a42451caacb6423abecbe6b74e628042.jpg "problem solving 2022")
- Identify the Problem
- Define the Problem
- Form a Strategy
- Organize Information
- Allocate Resources
- Monitor Progress
- Evaluate the Results
Frequently Asked Questions
Problem-solving is a mental process that involves discovering, analyzing, and solving problems. The ultimate goal of problem-solving is to overcome obstacles and find a solution that best resolves the issue.
The best strategy for solving a problem depends largely on the unique situation. In some cases, people are better off learning everything they can about the issue and then using factual knowledge to come up with a solution. In other instances, creativity and insight are the best options.
It is not necessary to follow problem-solving steps sequentially, It is common to skip steps or even go back through steps multiple times until the desired solution is reached.
In order to correctly solve a problem, it is often important to follow a series of steps. Researchers sometimes refer to this as the problem-solving cycle. While this cycle is portrayed sequentially, people rarely follow a rigid series of steps to find a solution.
The following steps include developing strategies and organizing knowledge.
1. Identifying the Problem
While it may seem like an obvious step, identifying the problem is not always as simple as it sounds. In some cases, people might mistakenly identify the wrong source of a problem, which will make attempts to solve it inefficient or even useless.
Some strategies that you might use to figure out the source of a problem include :
- Asking questions about the problem
- Breaking the problem down into smaller pieces
- Looking at the problem from different perspectives
- Conducting research to figure out what relationships exist between different variables
2. Defining the Problem
After the problem has been identified, it is important to fully define the problem so that it can be solved. You can define a problem by operationally defining each aspect of the problem and setting goals for what aspects of the problem you will address
At this point, you should focus on figuring out which aspects of the problems are facts and which are opinions. State the problem clearly and identify the scope of the solution.
3. Forming a Strategy
After the problem has been identified, it is time to start brainstorming potential solutions. This step usually involves generating as many ideas as possible without judging their quality. Once several possibilities have been generated, they can be evaluated and narrowed down.
The next step is to develop a strategy to solve the problem. The approach used will vary depending upon the situation and the individual's unique preferences. Common problem-solving strategies include heuristics and algorithms.
- Heuristics are mental shortcuts that are often based on solutions that have worked in the past. They can work well if the problem is similar to something you have encountered before and are often the best choice if you need a fast solution.
- Algorithms are step-by-step strategies that are guaranteed to produce a correct result. While this approach is great for accuracy, it can also consume time and resources.
Heuristics are often best used when time is of the essence, while algorithms are a better choice when a decision needs to be as accurate as possible.
4. Organizing Information
Before coming up with a solution, you need to first organize the available information. What do you know about the problem? What do you not know? The more information that is available the better prepared you will be to come up with an accurate solution.
When approaching a problem, it is important to make sure that you have all the data you need. Making a decision without adequate information can lead to biased or inaccurate results.
5. Allocating Resources
Of course, we don't always have unlimited money, time, and other resources to solve a problem. Before you begin to solve a problem, you need to determine how high priority it is.
If it is an important problem, it is probably worth allocating more resources to solving it. If, however, it is a fairly unimportant problem, then you do not want to spend too much of your available resources on coming up with a solution.
At this stage, it is important to consider all of the factors that might affect the problem at hand. This includes looking at the available resources, deadlines that need to be met, and any possible risks involved in each solution. After careful evaluation, a decision can be made about which solution to pursue.
6. Monitoring Progress
After selecting a problem-solving strategy, it is time to put the plan into action and see if it works. This step might involve trying out different solutions to see which one is the most effective.
It is also important to monitor the situation after implementing a solution to ensure that the problem has been solved and that no new problems have arisen as a result of the proposed solution.
Effective problem-solvers tend to monitor their progress as they work towards a solution. If they are not making good progress toward reaching their goal, they will reevaluate their approach or look for new strategies .
7. Evaluating the Results
After a solution has been reached, it is important to evaluate the results to determine if it is the best possible solution to the problem. This evaluation might be immediate, such as checking the results of a math problem to ensure the answer is correct, or it can be delayed, such as evaluating the success of a therapy program after several months of treatment.
Once a problem has been solved, it is important to take some time to reflect on the process that was used and evaluate the results. This will help you to improve your problem-solving skills and become more efficient at solving future problems.
A Word From Verywell
It is important to remember that there are many different problem-solving processes with different steps, and this is just one example. Problem-solving in real-world situations requires a great deal of resourcefulness, flexibility, resilience, and continuous interaction with the environment.
Get Advice From The Verywell Mind Podcast
Hosted by therapist Amy Morin, LCSW, this episode of The Verywell Mind Podcast shares how you can stop dwelling in a negative mindset.
Follow Now : Apple Podcasts / Spotify / Google Podcasts
You can become a better problem solving by:
- Practicing brainstorming and coming up with multiple potential solutions to problems
- Being open-minded and considering all possible options before making a decision
- Breaking down problems into smaller, more manageable pieces
- Asking for help when needed
- Researching different problem-solving techniques and trying out new ones
- Learning from mistakes and using them as opportunities to grow
It's important to communicate openly and honestly with your partner about what's going on. Try to see things from their perspective as well as your own. Work together to find a resolution that works for both of you. Be willing to compromise and accept that there may not be a perfect solution.
Take breaks if things are getting too heated, and come back to the problem when you feel calm and collected. Don't try to fix every problem on your own—consider asking a therapist or counselor for help and insight.
If you've tried everything and there doesn't seem to be a way to fix the problem, you may have to learn to accept it. This can be difficult, but try to focus on the positive aspects of your life and remember that every situation is temporary. Don't dwell on what's going wrong—instead, think about what's going right. Find support by talking to friends or family. Seek professional help if you're having trouble coping.
Davidson JE, Sternberg RJ, editors. The Psychology of Problem Solving . Cambridge University Press; 2003. doi:10.1017/CBO9780511615771
Sarathy V. Real world problem-solving . Front Hum Neurosci . 2018;12:261. Published 2018 Jun 26. doi:10.3389/fnhum.2018.00261
By Kendra Cherry, MSEd Kendra Cherry, MS, is a psychosocial rehabilitation specialist, psychology educator, and author of the "Everything Psychology Book."
What Are Problem-Solving Skills? Definition and Examples
- Share on Twitter Share on Twitter
- Share on Facebook Share on Facebook
- Share on LinkedIn Share on LinkedIn

Forage puts students first. Our blog articles are written independently by our editorial team. They have not been paid for or sponsored by our partners. See our full editorial guidelines .
Why do employers hire employees? To help them solve problems. Whether you’re a financial analyst deciding where to invest your firm’s money, or a marketer trying to figure out which channel to direct your efforts, companies hire people to help them find solutions. Problem-solving is an essential and marketable soft skill in the workplace.
So, how can you improve your problem-solving and show employers you have this valuable skill? In this guide, we’ll cover:
Problem-Solving Skills Definition
Why are problem-solving skills important, problem-solving skills examples, how to include problem-solving skills in a job application, how to improve problem-solving skills, problem-solving: the bottom line.
Problem-solving skills are the ability to identify problems, brainstorm and analyze answers, and implement the best solutions. An employee with good problem-solving skills is both a self-starter and a collaborative teammate; they are proactive in understanding the root of a problem and work with others to consider a wide range of solutions before deciding how to move forward.
Examples of using problem-solving skills in the workplace include:
- Researching patterns to understand why revenue decreased last quarter
- Experimenting with a new marketing channel to increase website sign-ups
- Brainstorming content types to share with potential customers
- Testing calls to action to see which ones drive the most product sales
- Implementing a new workflow to automate a team process and increase productivity
Problem-solving skills are the most sought-after soft skill of 2022. In fact, 86% of employers look for problem-solving skills on student resumes, according to the National Association of Colleges and Employers Job Outlook 2022 survey .
It’s unsurprising why employers are looking for this skill: companies will always need people to help them find solutions to their problems. Someone proactive and successful at problem-solving is valuable to any team.
“Employers are looking for employees who can make decisions independently, especially with the prevalence of remote/hybrid work and the need to communicate asynchronously,” Eric Mochnacz, senior HR consultant at Red Clover, says. “Employers want to see individuals who can make well-informed decisions that mitigate risk, and they can do so without suffering from analysis paralysis.”
Showcase new skills
Build the confidence and practical skills that employers are looking for with Forage’s free job simulations.
Problem-solving includes three main parts: identifying the problem, analyzing possible solutions, and deciding on the best course of action.
>>MORE: Discover the right career for you based on your skills with a career aptitude test .
Research is the first step of problem-solving because it helps you understand the context of a problem. Researching a problem enables you to learn why the problem is happening. For example, is revenue down because of a new sales tactic? Or because of seasonality? Is there a problem with who the sales team is reaching out to?
Research broadens your scope to all possible reasons why the problem could be happening. Then once you figure it out, it helps you narrow your scope to start solving it.
Analysis is the next step of problem-solving. Now that you’ve identified the problem, analytical skills help you look at what potential solutions there might be.
“The goal of analysis isn’t to solve a problem, actually — it’s to better understand it because that’s where the real solution will be found,” Gretchen Skalka, owner of Career Insights Consulting, says. “Looking at a problem through the lens of impartiality is the only way to get a true understanding of it from all angles.”
Decision-Making
Once you’ve figured out where the problem is coming from and what solutions are, it’s time to decide on the best way to go forth. Decision-making skills help you determine what resources are available, what a feasible action plan entails, and what solution is likely to lead to success.
On a Resume
Employers looking for problem-solving skills might include the word “problem-solving” or other synonyms like “ critical thinking ” or “analytical skills” in the job description.
“I would add ‘buzzwords’ you can find from the job descriptions or LinkedIn endorsements section to filter into your resume to comply with the ATS,” Matthew Warzel, CPRW resume writer, advises. Warzel recommends including these skills on your resume but warns to “leave the soft skills as adjectives in the summary section. That is the only place soft skills should be mentioned.”
On the other hand, you can list hard skills separately in a skills section on your resume .

Forage Resume Writing Masterclass
Learn how to showcase your skills and craft an award-winning resume with this free masterclass from Forage.
Avg. Time: 5 to 6 hours
Skills you’ll build: Resume writing, professional brand, professional summary, narrative, transferable skills, industry keywords, illustrating your impact, standing out
In a Cover Letter or an Interview
Explaining your problem-solving skills in an interview can seem daunting. You’re required to expand on your process — how you identified a problem, analyzed potential solutions, and made a choice. As long as you can explain your approach, it’s okay if that solution didn’t come from a professional work experience.
“Young professionals shortchange themselves by thinking only paid-for solutions matter to employers,” Skalka says. “People at the genesis of their careers don’t have a wealth of professional experience to pull from, but they do have relevant experience to share.”
Aaron Case, career counselor and CPRW at Resume Genius, agrees and encourages early professionals to share this skill. “If you don’t have any relevant work experience yet, you can still highlight your problem-solving skills in your cover letter,” he says. “Just showcase examples of problems you solved while completing your degree, working at internships, or volunteering. You can even pull examples from completely unrelated part-time jobs, as long as you make it clear how your problem-solving ability transfers to your new line of work.”
Learn How to Identify Problems
Problem-solving doesn’t just require finding solutions to problems that are already there. It’s also about being proactive when something isn’t working as you hoped it would. Practice questioning and getting curious about processes and activities in your everyday life. What could you improve? What would you do if you had more resources for this process? If you had fewer? Challenge yourself to challenge the world around you.
Think Digitally
“Employers in the modern workplace value digital problem-solving skills, like being able to find a technology solution to a traditional issue,” Case says. “For example, when I first started working as a marketing writer, my department didn’t have the budget to hire a professional voice actor for marketing video voiceovers. But I found a perfect solution to the problem with an AI voiceover service that cost a fraction of the price of an actor.”
Being comfortable with new technology — even ones you haven’t used before — is a valuable skill in an increasingly hybrid and remote world. Don’t be afraid to research new and innovative technologies to help automate processes or find a more efficient technological solution.
Collaborate
Problem-solving isn’t done in a silo, and it shouldn’t be. Use your collaboration skills to gather multiple perspectives, help eliminate bias, and listen to alternative solutions. Ask others where they think the problem is coming from and what solutions would help them with your workflow. From there, try to compromise on a solution that can benefit everyone.
If we’ve learned anything from the past few years, it’s that the world of work is constantly changing — which means it’s crucial to know how to adapt . Be comfortable narrowing down a solution, then changing your direction when a colleague provides a new piece of information. Challenge yourself to get out of your comfort zone, whether with your personal routine or trying a new system at work.
Put Yourself in the Middle of Tough Moments
Just like adapting requires you to challenge your routine and tradition, good problem-solving requires you to put yourself in challenging situations — especially ones where you don’t have relevant experience or expertise to find a solution. Because you won’t know how to tackle the problem, you’ll learn new problem-solving skills and how to navigate new challenges. Ask your manager or a peer if you can help them work on a complicated problem, and be proactive about asking them questions along the way.
Career Aptitude Test
What careers are right for you based on your skills? Take this quiz to find out. It’s completely free — you’ll just need to sign up to get your results!
Step 1 of 3
Companies always need people to help them find solutions — especially proactive employees who have practical analytical skills and can collaborate to decide the best way to move forward. Whether or not you have experience solving problems in a professional workplace, illustrate your problem-solving skills by describing your research, analysis, and decision-making process — and make it clear that you’re the solution to the employer’s current problems.
Looking to learn more workplace professional skills? Check out Two Sigma’s Professional Skills Development Virtual Experience Program .
Image Credit: Christina Morillo / Pexels

Related Posts
6 negotiation skills to level up your work life, how to build conflict resolution skills: case studies and examples, what is github uses and getting started, upskill with forage.

Build career skills recruiters are looking for.
How to improve your problem solving skills and build effective problem solving strategies

Design your next session with SessionLab
Join the 150,000+ facilitators using SessionLab.
Recommended Articles
A step-by-step guide to planning a workshop, how to create an unforgettable training session in 8 simple steps, 18 free facilitation resources we think you’ll love.
- 47 useful online tools for workshop planning and meeting facilitation
Effective problem solving is all about using the right process and following a plan tailored to the issue at hand. Recognizing your team or organization has an issue isn’t enough to come up with effective problem solving strategies.
To truly understand a problem and develop appropriate solutions, you will want to follow a solid process, follow the necessary problem solving steps, and bring all of your problem solving skills to the table.
We’ll first guide you through the seven step problem solving process you and your team can use to effectively solve complex business challenges. We’ll also look at what problem solving strategies you can employ with your team when looking for a way to approach the process. We’ll then discuss the problem solving skills you need to be more effective at solving problems, complete with an activity from the SessionLab library you can use to develop that skill in your team.
Let’s get to it!
What is a problem solving process?
- What are the problem solving steps I need to follow?
Problem solving strategies
What skills do i need to be an effective problem solver, how can i improve my problem solving skills.
Solving problems is like baking a cake. You can go straight into the kitchen without a recipe or the right ingredients and do your best, but the end result is unlikely to be very tasty!
Using a process to bake a cake allows you to use the best ingredients without waste, collect the right tools, account for allergies, decide whether it is a birthday or wedding cake, and then bake efficiently and on time. The result is a better cake that is fit for purpose, tastes better and has created less mess in the kitchen. Also, it should have chocolate sprinkles. Having a step by step process to solve organizational problems allows you to go through each stage methodically and ensure you are trying to solve the right problems and select the most appropriate, effective solutions.
What are the problem solving steps I need to follow?
All problem solving processes go through a number of steps in order to move from identifying a problem to resolving it.
Depending on your problem solving model and who you ask, there can be anything between four and nine problem solving steps you should follow in order to find the right solution. Whatever framework you and your group use, there are some key items that should be addressed in order to have an effective process.
We’ve looked at problem solving processes from sources such as the American Society for Quality and their four step approach , and Mediate ‘s six step process. By reflecting on those and our own problem solving processes, we’ve come up with a sequence of seven problem solving steps we feel best covers everything you need in order to effectively solve problems.

1. Problem identification
The first stage of any problem solving process is to identify the problem or problems you might want to solve. Effective problem solving strategies always begin by allowing a group scope to articulate what they believe the problem to be and then coming to some consensus over which problem they approach first. Problem solving activities used at this stage often have a focus on creating frank, open discussion so that potential problems can be brought to the surface.
2. Problem analysis
Though this step is not a million miles from problem identification, problem analysis deserves to be considered separately. It can often be an overlooked part of the process and is instrumental when it comes to developing effective solutions.
The process of problem analysis means ensuring that the problem you are seeking to solve is the right problem . As part of this stage, you may look deeper and try to find the root cause of a specific problem at a team or organizational level.
Remember that problem solving strategies should not only be focused on putting out fires in the short term but developing long term solutions that deal with the root cause of organizational challenges.
Whatever your approach, analyzing a problem is crucial in being able to select an appropriate solution and the problem solving skills deployed in this stage are beneficial for the rest of the process and ensuring the solutions you create are fit for purpose.
3. Solution generation
Once your group has nailed down the particulars of the problem you wish to solve, you want to encourage a free flow of ideas connecting to solving that problem. This can take the form of problem solving games that encourage creative thinking or problem solving activities designed to produce working prototypes of possible solutions.
The key to ensuring the success of this stage of the problem solving process is to encourage quick, creative thinking and create an open space where all ideas are considered. The best solutions can come from unlikely places and by using problem solving techniques that celebrate invention, you might come up with solution gold.
4. Solution development
No solution is likely to be perfect right out of the gate. It’s important to discuss and develop the solutions your group has come up with over the course of following the previous problem solving steps in order to arrive at the best possible solution. Problem solving games used in this stage involve lots of critical thinking, measuring potential effort and impact, and looking at possible solutions analytically.
During this stage, you will often ask your team to iterate and improve upon your frontrunning solutions and develop them further. Remember that problem solving strategies always benefit from a multitude of voices and opinions, and not to let ego get involved when it comes to choosing which solutions to develop and take further.
Finding the best solution is the goal of all problem solving workshops and here is the place to ensure that your solution is well thought out, sufficiently robust and fit for purpose.
5. Decision making
Nearly there! Once your group has reached consensus and selected a solution that applies to the problem at hand you have some decisions to make. You will want to work on allocating ownership of the project, figure out who will do what, how the success of the solution will be measured and decide the next course of action.
The decision making stage is a part of the problem solving process that can get missed or taken as for granted. Fail to properly allocate roles and plan out how a solution will actually be implemented and it less likely to be successful in solving the problem.
Have clear accountabilities, actions, timeframes, and follow-ups. Make these decisions and set clear next-steps in the problem solving workshop so that everyone is aligned and you can move forward effectively as a group.
Ensuring that you plan for the roll-out of a solution is one of the most important problem solving steps. Without adequate planning or oversight, it can prove impossible to measure success or iterate further if the problem was not solved.
6. Solution implementation
This is what we were waiting for! All problem solving strategies have the end goal of implementing a solution and solving a problem in mind.
Remember that in order for any solution to be successful, you need to help your group through all of the previous problem solving steps thoughtfully. Only then can you ensure that you are solving the right problem but also that you have developed the correct solution and can then successfully implement and measure the impact of that solution.
Project management and communication skills are key here – your solution may need to adjust when out in the wild or you might discover new challenges along the way.
7. Solution evaluation
So you and your team developed a great solution to a problem and have a gut feeling its been solved. Work done, right? Wrong. All problem solving strategies benefit from evaluation, consideration, and feedback. You might find that the solution does not work for everyone, might create new problems, or is potentially so successful that you will want to roll it out to larger teams or as part of other initiatives.
None of that is possible without taking the time to evaluate the success of the solution you developed in your problem solving model and adjust if necessary.
Remember that the problem solving process is often iterative and it can be common to not solve complex issues on the first try. Even when this is the case, you and your team will have generated learning that will be important for future problem solving workshops or in other parts of the organization.
It’s worth underlining how important record keeping is throughout the problem solving process. If a solution didn’t work, you need to have the data and records to see why that was the case. If you go back to the drawing board, notes from the previous workshop can help save time. Data and insight is invaluable at every stage of the problem solving process and this one is no different.
Problem solving workshops made easy
Problem solving strategies are methods of approaching and facilitating the process of problem-solving with a set of techniques , actions, and processes. Different strategies are more effective if you are trying to solve broad problems such as achieving higher growth versus more focused problems like, how do we improve our customer onboarding process?
Broadly, the problem solving steps outlined above should be included in any problem solving strategy though choosing where to focus your time and what approaches should be taken is where they begin to differ. You might find that some strategies ask for the problem identification to be done prior to the session or that everything happens in the course of a one day workshop.
The key similarity is that all good problem solving strategies are structured and designed. Four hours of open discussion is never going to be as productive as a four-hour workshop designed to lead a group through a problem solving process.
Good problem solving strategies are tailored to the team, organization and problem you will be attempting to solve. Here are some example problem solving strategies you can learn from or use to get started.
Use a workshop to lead a team through a group process
Often, the first step to solving problems or organizational challenges is bringing a group together effectively. Most teams have the tools, knowledge, and expertise necessary to solve their challenges – they just need some guidance in how to use leverage those skills and a structure and format that allows people to focus their energies.
Facilitated workshops are one of the most effective ways of solving problems of any scale. By designing and planning your workshop carefully, you can tailor the approach and scope to best fit the needs of your team and organization.
Problem solving workshop
- Creating a bespoke, tailored process
- Tackling problems of any size
- Building in-house workshop ability and encouraging their use
Workshops are an effective strategy for solving problems. By using tried and test facilitation techniques and methods, you can design and deliver a workshop that is perfectly suited to the unique variables of your organization. You may only have the capacity for a half-day workshop and so need a problem solving process to match.
By using our session planner tool and importing methods from our library of 700+ facilitation techniques, you can create the right problem solving workshop for your team. It might be that you want to encourage creative thinking or look at things from a new angle to unblock your groups approach to problem solving. By tailoring your workshop design to the purpose, you can help ensure great results.
One of the main benefits of a workshop is the structured approach to problem solving. Not only does this mean that the workshop itself will be successful, but many of the methods and techniques will help your team improve their working processes outside of the workshop.
We believe that workshops are one of the best tools you can use to improve the way your team works together. Start with a problem solving workshop and then see what team building, culture or design workshops can do for your organization!
Run a design sprint
Great for:
- aligning large, multi-discipline teams
- quickly designing and testing solutions
- tackling large, complex organizational challenges and breaking them down into smaller tasks
By using design thinking principles and methods, a design sprint is a great way of identifying, prioritizing and prototyping solutions to long term challenges that can help solve major organizational problems with quick action and measurable results.
Some familiarity with design thinking is useful, though not integral, and this strategy can really help a team align if there is some discussion around which problems should be approached first.
The stage-based structure of the design sprint is also very useful for teams new to design thinking. The inspiration phase, where you look to competitors that have solved your problem, and the rapid prototyping and testing phases are great for introducing new concepts that will benefit a team in all their future work.
It can be common for teams to look inward for solutions and so looking to the market for solutions you can iterate on can be very productive. Instilling an agile prototyping and testing mindset can also be great when helping teams move forwards – generating and testing solutions quickly can help save time in the long run and is also pretty exciting!
Break problems down into smaller issues
Organizational challenges and problems are often complicated and large scale in nature. Sometimes, trying to resolve such an issue in one swoop is simply unachievable or overwhelming. Try breaking down such problems into smaller issues that you can work on step by step. You may not be able to solve the problem of churning customers off the bat, but you can work with your team to identify smaller effort but high impact elements and work on those first.
This problem solving strategy can help a team generate momentum, prioritize and get some easy wins. It’s also a great strategy to employ with teams who are just beginning to learn how to approach the problem solving process. If you want some insight into a way to employ this strategy, we recommend looking at our design sprint template below!
Use guiding frameworks or try new methodologies
Some problems are best solved by introducing a major shift in perspective or by using new methodologies that encourage your team to think differently.
Props and tools such as Methodkit , which uses a card-based toolkit for facilitation, or Lego Serious Play can be great ways to engage your team and find an inclusive, democratic problem solving strategy. Remember that play and creativity are great tools for achieving change and whatever the challenge, engaging your participants can be very effective where other strategies may have failed.
LEGO Serious Play
- Improving core problem solving skills
- Thinking outside of the box
- Encouraging creative solutions
LEGO Serious Play is a problem solving methodology designed to get participants thinking differently by using 3D models and kinesthetic learning styles. By physically building LEGO models based on questions and exercises, participants are encouraged to think outside of the box and create their own responses.
Collaborate LEGO Serious Play exercises are also used to encourage communication and build problem solving skills in a group. By using this problem solving process, you can often help different kinds of learners and personality types contribute and unblock organizational problems with creative thinking.
Problem solving strategies like LEGO Serious Play are super effective at helping a team solve more skills-based problems such as communication between teams or a lack of creative thinking. Some problems are not suited to LEGO Serious Play and require a different problem solving strategy.
Card Decks and Method Kits
- New facilitators or non-facilitators
- Approaching difficult subjects with a simple, creative framework
- Engaging those with varied learning styles
Card decks and method kids are great tools for those new to facilitation or for whom facilitation is not the primary role. Card decks such as the emotional culture deck can be used for complete workshops and in many cases, can be used right out of the box. Methodkit has a variety of kits designed for scenarios ranging from personal development through to personas and global challenges so you can find the right deck for your particular needs.
Having an easy to use framework that encourages creativity or a new approach can take some of the friction or planning difficulties out of the workshop process and energize a team in any setting. Simplicity is the key with these methods. By ensuring everyone on your team can get involved and engage with the process as quickly as possible can really contribute to the success of your problem solving strategy.
Source external advice
Looking to peers, experts and external facilitators can be a great way of approaching the problem solving process. Your team may not have the necessary expertise, insights of experience to tackle some issues, or you might simply benefit from a fresh perspective. Some problems may require bringing together an entire team, and coaching managers or team members individually might be the right approach. Remember that not all problems are best resolved in the same manner.
If you’re a solo entrepreneur, peer groups, coaches and mentors can also be invaluable at not only solving specific business problems, but in providing a support network for resolving future challenges. One great approach is to join a Mastermind Group and link up with like-minded individuals and all grow together. Remember that however you approach the sourcing of external advice, do so thoughtfully, respectfully and honestly. Reciprocate where you can and prepare to be surprised by just how kind and helpful your peers can be!
Mastermind Group
- Solo entrepreneurs or small teams with low capacity
- Peer learning and gaining outside expertise
- Getting multiple external points of view quickly
Problem solving in large organizations with lots of skilled team members is one thing, but how about if you work for yourself or in a very small team without the capacity to get the most from a design sprint or LEGO Serious Play session?
A mastermind group – sometimes known as a peer advisory board – is where a group of people come together to support one another in their own goals, challenges, and businesses. Each participant comes to the group with their own purpose and the other members of the group will help them create solutions, brainstorm ideas, and support one another.
Mastermind groups are very effective in creating an energized, supportive atmosphere that can deliver meaningful results. Learning from peers from outside of your organization or industry can really help unlock new ways of thinking and drive growth. Access to the experience and skills of your peers can be invaluable in helping fill the gaps in your own ability, particularly in young companies.
A mastermind group is a great solution for solo entrepreneurs, small teams, or for organizations that feel that external expertise or fresh perspectives will be beneficial for them. It is worth noting that Mastermind groups are often only as good as the participants and what they can bring to the group. Participants need to be committed, engaged and understand how to work in this context.
Coaching and mentoring
- Focused learning and development
- Filling skills gaps
- Working on a range of challenges over time
Receiving advice from a business coach or building a mentor/mentee relationship can be an effective way of resolving certain challenges. The one-to-one format of most coaching and mentor relationships can really help solve the challenges those individuals are having and benefit the organization as a result.
A great mentor can be invaluable when it comes to spotting potential problems before they arise and coming to understand a mentee very well has a host of other business benefits. You might run an internal mentorship program to help develop your team’s problem solving skills and strategies or as part of a large learning and development program. External coaches can also be an important part of your problem solving strategy, filling skills gaps for your management team or helping with specific business issues.
Now we’ve explored the problem solving process and the steps you will want to go through in order to have an effective session, let’s look at the skills you and your team need to be more effective problem solvers.
Problem solving skills are highly sought after, whatever industry or team you work in. Organizations are keen to employ people who are able to approach problems thoughtfully and find strong, realistic solutions. Whether you are a facilitator , a team leader or a developer, being an effective problem solver is a skill you’ll want to develop.
Problem solving skills form a whole suite of techniques and approaches that an individual uses to not only identify problems but to discuss them productively before then developing appropriate solutions.
Here are some of the most important problem solving skills everyone from executives to junior staff members should learn. We’ve also included an activity or exercise from the SessionLab library that can help you and your team develop that skill.
If you’re running a workshop or training session to try and improve problem solving skills in your team, try using these methods to supercharge your process!

Active listening
Active listening is one of the most important skills anyone who works with people can possess. In short, active listening is a technique used to not only better understand what is being said by an individual, but also to be more aware of the underlying message the speaker is trying to convey. When it comes to problem solving, active listening is integral for understanding the position of every participant and to clarify the challenges, ideas and solutions they bring to the table.
Some active listening skills include:
- Paying complete attention to the speaker.
- Removing distractions.
- Avoid interruption.
- Taking the time to fully understand before preparing a rebuttal.
- Responding respectfully and appropriately.
- Demonstrate attentiveness and positivity with an open posture, making eye contact with the speaker, smiling and nodding if appropriate. Show that you are listening and encourage them to continue.
- Be aware of and respectful of feelings. Judge the situation and respond appropriately. You can disagree without being disrespectful.
- Observe body language.
- Paraphrase what was said in your own words, either mentally or verbally.
- Remain neutral.
- Reflect and take a moment before responding.
- Ask deeper questions based on what is said and clarify points where necessary.
Active Listening #hyperisland #skills #active listening #remote-friendly This activity supports participants to reflect on a question and generate their own solutions using simple principles of active listening and peer coaching. It’s an excellent introduction to active listening but can also be used with groups that are already familiar with it. Participants work in groups of three and take turns being: “the subject”, the listener, and the observer.
Analytical skills
All problem solving models require strong analytical skills, particularly during the beginning of the process and when it comes to analyzing how solutions have performed.
Analytical skills are primarily focused on performing an effective analysis by collecting, studying and parsing data related to a problem or opportunity.
It often involves spotting patterns, being able to see things from different perspectives and using observable facts and data to make suggestions or produce insight.
Analytical skills are also important at every stage of the problem solving process and by having these skills, you can ensure that any ideas or solutions you create or backed up analytically and have been sufficiently thought out.
Nine Whys #innovation #issue analysis #liberating structures With breathtaking simplicity, you can rapidly clarify for individuals and a group what is essentially important in their work. You can quickly reveal when a compelling purpose is missing in a gathering and avoid moving forward without clarity. When a group discovers an unambiguous shared purpose, more freedom and more responsibility are unleashed. You have laid the foundation for spreading and scaling innovations with fidelity.
Collaboration
Trying to solve problems on your own is difficult. Being able to collaborate effectively, with a free exchange of ideas, to delegate and be a productive member of a team is hugely important to all problem solving strategies.
Remember that whatever your role, collaboration is integral, and in a problem solving process, you are all working together to find the best solution for everyone.
Marshmallow challenge with debriefing #teamwork #team #leadership #collaboration In eighteen minutes, teams must build the tallest free-standing structure out of 20 sticks of spaghetti, one yard of tape, one yard of string, and one marshmallow. The marshmallow needs to be on top. The Marshmallow Challenge was developed by Tom Wujec, who has done the activity with hundreds of groups around the world. Visit the Marshmallow Challenge website for more information. This version has an extra debriefing question added with sample questions focusing on roles within the team.
Communication
Being an effective communicator means being empathetic, clear and succinct, asking the right questions, and demonstrating active listening skills throughout any discussion or meeting.
In a problem solving setting, you need to communicate well in order to progress through each stage of the process effectively. As a team leader, it may also fall to you to facilitate communication between parties who may not see eye to eye. Effective communication also means helping others to express themselves and be heard in a group.
Bus Trip #feedback #communication #appreciation #closing #thiagi #team This is one of my favourite feedback games. I use Bus Trip at the end of a training session or a meeting, and I use it all the time. The game creates a massive amount of energy with lots of smiles, laughs, and sometimes even a teardrop or two.
Creative problem solving skills can be some of the best tools in your arsenal. Thinking creatively, being able to generate lots of ideas and come up with out of the box solutions is useful at every step of the process.
The kinds of problems you will likely discuss in a problem solving workshop are often difficult to solve, and by approaching things in a fresh, creative manner, you can often create more innovative solutions.
Having practical creative skills is also a boon when it comes to problem solving. If you can help create quality design sketches and prototypes in record time, it can help bring a team to alignment more quickly or provide a base for further iteration.
The paper clip method #sharing #creativity #warm up #idea generation #brainstorming The power of brainstorming. A training for project leaders, creativity training, and to catalyse getting new solutions.
Critical thinking
Critical thinking is one of the fundamental problem solving skills you’ll want to develop when working on developing solutions. Critical thinking is the ability to analyze, rationalize and evaluate while being aware of personal bias, outlying factors and remaining open-minded.
Defining and analyzing problems without deploying critical thinking skills can mean you and your team go down the wrong path. Developing solutions to complex issues requires critical thinking too – ensuring your team considers all possibilities and rationally evaluating them.
Agreement-Certainty Matrix #issue analysis #liberating structures #problem solving You can help individuals or groups avoid the frequent mistake of trying to solve a problem with methods that are not adapted to the nature of their challenge. The combination of two questions makes it possible to easily sort challenges into four categories: simple, complicated, complex , and chaotic . A problem is simple when it can be solved reliably with practices that are easy to duplicate. It is complicated when experts are required to devise a sophisticated solution that will yield the desired results predictably. A problem is complex when there are several valid ways to proceed but outcomes are not predictable in detail. Chaotic is when the context is too turbulent to identify a path forward. A loose analogy may be used to describe these differences: simple is like following a recipe, complicated like sending a rocket to the moon, complex like raising a child, and chaotic is like the game “Pin the Tail on the Donkey.” The Liberating Structures Matching Matrix in Chapter 5 can be used as the first step to clarify the nature of a challenge and avoid the mismatches between problems and solutions that are frequently at the root of chronic, recurring problems.
Data analysis
Though it shares lots of space with general analytical skills, data analysis skills are something you want to cultivate in their own right in order to be an effective problem solver.
Being good at data analysis doesn’t just mean being able to find insights from data, but also selecting the appropriate data for a given issue, interpreting it effectively and knowing how to model and present that data. Depending on the problem at hand, it might also include a working knowledge of specific data analysis tools and procedures.
Having a solid grasp of data analysis techniques is useful if you’re leading a problem solving workshop but if you’re not an expert, don’t worry. Bring people into the group who has this skill set and help your team be more effective as a result.
Decision making
All problems need a solution and all solutions require that someone make the decision to implement them. Without strong decision making skills, teams can become bogged down in discussion and less effective as a result.
Making decisions is a key part of the problem solving process. It’s important to remember that decision making is not restricted to the leadership team. Every staff member makes decisions every day and developing these skills ensures that your team is able to solve problems at any scale. Remember that making decisions does not mean leaping to the first solution but weighing up the options and coming to an informed, well thought out solution to any given problem that works for the whole team.
Lightning Decision Jam (LDJ) #action #decision making #problem solving #issue analysis #innovation #design #remote-friendly The problem with anything that requires creative thinking is that it’s easy to get lost—lose focus and fall into the trap of having useless, open-ended, unstructured discussions. Here’s the most effective solution I’ve found: Replace all open, unstructured discussion with a clear process. What to use this exercise for: Anything which requires a group of people to make decisions, solve problems or discuss challenges. It’s always good to frame an LDJ session with a broad topic, here are some examples: The conversion flow of our checkout Our internal design process How we organise events Keeping up with our competition Improving sales flow
Dependability
Most complex organizational problems require multiple people to be involved in delivering the solution. Ensuring that the team and organization can depend on you to take the necessary actions and communicate where necessary is key to ensuring problems are solved effectively.
Being dependable also means working to deadlines and to brief. It is often a matter of creating trust in a team so that everyone can depend on one another to complete the agreed actions in the agreed time frame so that the team can move forward together. Being undependable can create problems of friction and can limit the effectiveness of your solutions so be sure to bear this in mind throughout a project.
Team Purpose & Culture #team #hyperisland #culture #remote-friendly This is an essential process designed to help teams define their purpose (why they exist) and their culture (how they work together to achieve that purpose). Defining these two things will help any team to be more focused and aligned. With support of tangible examples from other companies, the team members work as individuals and a group to codify the way they work together. The goal is a visual manifestation of both the purpose and culture that can be put up in the team’s work space.
Emotional intelligence
Emotional intelligence is an important skill for any successful team member, whether communicating internally or with clients or users. In the problem solving process, emotional intelligence means being attuned to how people are feeling and thinking, communicating effectively and being self-aware of what you bring to a room.
There are often differences of opinion when working through problem solving processes, and it can be easy to let things become impassioned or combative. Developing your emotional intelligence means being empathetic to your colleagues and managing your own emotions throughout the problem and solution process. Be kind, be thoughtful and put your points across care and attention.
Being emotionally intelligent is a skill for life and by deploying it at work, you can not only work efficiently but empathetically. Check out the emotional culture workshop template for more!
Facilitation
As we’ve clarified in our facilitation skills post, facilitation is the art of leading people through processes towards agreed-upon objectives in a manner that encourages participation, ownership, and creativity by all those involved. While facilitation is a set of interrelated skills in itself, the broad definition of facilitation can be invaluable when it comes to problem solving. Leading a team through a problem solving process is made more effective if you improve and utilize facilitation skills – whether you’re a manager, team leader or external stakeholder.
The Six Thinking Hats #creative thinking #meeting facilitation #problem solving #issue resolution #idea generation #conflict resolution The Six Thinking Hats are used by individuals and groups to separate out conflicting styles of thinking. They enable and encourage a group of people to think constructively together in exploring and implementing change, rather than using argument to fight over who is right and who is wrong.
Flexibility
Being flexible is a vital skill when it comes to problem solving. This does not mean immediately bowing to pressure or changing your opinion quickly: instead, being flexible is all about seeing things from new perspectives, receiving new information and factoring it into your thought process.
Flexibility is also important when it comes to rolling out solutions. It might be that other organizational projects have greater priority or require the same resources as your chosen solution. Being flexible means understanding needs and challenges across the team and being open to shifting or arranging your own schedule as necessary. Again, this does not mean immediately making way for other projects. It’s about articulating your own needs, understanding the needs of others and being able to come to a meaningful compromise.
The Creativity Dice #creativity #problem solving #thiagi #issue analysis Too much linear thinking is hazardous to creative problem solving. To be creative, you should approach the problem (or the opportunity) from different points of view. You should leave a thought hanging in mid-air and move to another. This skipping around prevents premature closure and lets your brain incubate one line of thought while you consciously pursue another.
Working in any group can lead to unconscious elements of groupthink or situations in which you may not wish to be entirely honest. Disagreeing with the opinions of the executive team or wishing to save the feelings of a coworker can be tricky to navigate, but being honest is absolutely vital when to comes to developing effective solutions and ensuring your voice is heard.
Remember that being honest does not mean being brutally candid. You can deliver your honest feedback and opinions thoughtfully and without creating friction by using other skills such as emotional intelligence.
Explore your Values #hyperisland #skills #values #remote-friendly Your Values is an exercise for participants to explore what their most important values are. It’s done in an intuitive and rapid way to encourage participants to follow their intuitive feeling rather than over-thinking and finding the “correct” values. It is a good exercise to use to initiate reflection and dialogue around personal values.
Initiative
The problem solving process is multi-faceted and requires different approaches at certain points of the process. Taking initiative to bring problems to the attention of the team, collect data or lead the solution creating process is always valuable. You might even roadtest your own small scale solutions or brainstorm before a session. Taking initiative is particularly effective if you have good deal of knowledge in that area or have ownership of a particular project and want to get things kickstarted.
That said, be sure to remember to honor the process and work in service of the team. If you are asked to own one part of the problem solving process and you don’t complete that task because your initiative leads you to work on something else, that’s not an effective method of solving business challenges.
15% Solutions #action #liberating structures #remote-friendly You can reveal the actions, however small, that everyone can do immediately. At a minimum, these will create momentum, and that may make a BIG difference. 15% Solutions show that there is no reason to wait around, feel powerless, or fearful. They help people pick it up a level. They get individuals and the group to focus on what is within their discretion instead of what they cannot change. With a very simple question, you can flip the conversation to what can be done and find solutions to big problems that are often distributed widely in places not known in advance. Shifting a few grains of sand may trigger a landslide and change the whole landscape.
Impartiality
A particularly useful problem solving skill for product owners or managers is the ability to remain impartial throughout much of the process. In practice, this means treating all points of view and ideas brought forward in a meeting equally and ensuring that your own areas of interest or ownership are not favored over others.
There may be a stage in the process where a decision maker has to weigh the cost and ROI of possible solutions against the company roadmap though even then, ensuring that the decision made is based on merit and not personal opinion.
Empathy map #frame insights #create #design #issue analysis An empathy map is a tool to help a design team to empathize with the people they are designing for. You can make an empathy map for a group of people or for a persona. To be used after doing personas when more insights are needed.
Being a good leader means getting a team aligned, energized and focused around a common goal. In the problem solving process, strong leadership helps ensure that the process is efficient, that any conflicts are resolved and that a team is managed in the direction of success.
It’s common for managers or executives to assume this role in a problem solving workshop, though it’s important that the leader maintains impartiality and does not bulldoze the group in a particular direction. Remember that good leadership means working in service of the purpose and team and ensuring the workshop is a safe space for employees of any level to contribute. Take a look at our leadership games and activities post for more exercises and methods to help improve leadership in your organization.
Leadership Pizza #leadership #team #remote-friendly This leadership development activity offers a self-assessment framework for people to first identify what skills, attributes and attitudes they find important for effective leadership, and then assess their own development and initiate goal setting.
In the context of problem solving, mediation is important in keeping a team engaged, happy and free of conflict. When leading or facilitating a problem solving workshop, you are likely to run into differences of opinion. Depending on the nature of the problem, certain issues may be brought up that are emotive in nature.
Being an effective mediator means helping those people on either side of such a divide are heard, listen to one another and encouraged to find common ground and a resolution. Mediating skills are useful for leaders and managers in many situations and the problem solving process is no different.
Conflict Responses #hyperisland #team #issue resolution A workshop for a team to reflect on past conflicts, and use them to generate guidelines for effective conflict handling. The workshop uses the Thomas-Killman model of conflict responses to frame a reflective discussion. Use it to open up a discussion around conflict with a team.
Planning
Solving organizational problems is much more effective when following a process or problem solving model. Planning skills are vital in order to structure, deliver and follow-through on a problem solving workshop and ensure your solutions are intelligently deployed.
Planning skills include the ability to organize tasks and a team, plan and design the process and take into account any potential challenges. Taking the time to plan carefully can save time and frustration later in the process and is valuable for ensuring a team is positioned for success.
3 Action Steps #hyperisland #action #remote-friendly This is a small-scale strategic planning session that helps groups and individuals to take action toward a desired change. It is often used at the end of a workshop or programme. The group discusses and agrees on a vision, then creates some action steps that will lead them towards that vision. The scope of the challenge is also defined, through discussion of the helpful and harmful factors influencing the group.
Prioritization
As organisations grow, the scale and variation of problems they face multiplies. Your team or is likely to face numerous challenges in different areas and so having the skills to analyze and prioritize becomes very important, particularly for those in leadership roles.
A thorough problem solving process is likely to deliver multiple solutions and you may have several different problems you wish to solve simultaneously. Prioritization is the ability to measure the importance, value, and effectiveness of those possible solutions and choose which to enact and in what order. The process of prioritization is integral in ensuring the biggest challenges are addressed with the most impactful solutions.
Impact and Effort Matrix #gamestorming #decision making #action #remote-friendly In this decision-making exercise, possible actions are mapped based on two factors: effort required to implement and potential impact. Categorizing ideas along these lines is a useful technique in decision making, as it obliges contributors to balance and evaluate suggested actions before committing to them.
Project management
Some problem solving skills are utilized in a workshop or ideation phases, while others come in useful when it comes to decision making. Overseeing an entire problem solving process and ensuring its success requires strong project management skills.
While project management incorporates many of the other skills listed here, it is important to note the distinction of considering all of the factors of a project and managing them successfully. Being able to negotiate with stakeholders, manage tasks, time and people, consider costs and ROI, and tie everything together is massively helpful when going through the problem solving process.
Record keeping
Working out meaningful solutions to organizational challenges is only one part of the process. Thoughtfully documenting and keeping records of each problem solving step for future consultation is important in ensuring efficiency and meaningful change.
For example, some problems may be lower priority than others but can be revisited in the future. If the team has ideated on solutions and found some are not up to the task, record those so you can rule them out and avoiding repeating work. Keeping records of the process also helps you improve and refine your problem solving model next time around!
Personal Kanban #gamestorming #action #agile #project planning Personal Kanban is a tool for organizing your work to be more efficient and productive. It is based on agile methods and principles.
Research skills
Conducting research to support both the identification of problems and the development of appropriate solutions is important for an effective process. Knowing where to go to collect research, how to conduct research efficiently, and identifying pieces of research are relevant are all things a good researcher can do well.
In larger groups, not everyone has to demonstrate this ability in order for a problem solving workshop to be effective. That said, having people with research skills involved in the process, particularly if they have existing area knowledge, can help ensure the solutions that are developed with data that supports their intention. Remember that being able to deliver the results of research efficiently and in a way the team can easily understand is also important. The best data in the world is only as effective as how it is delivered and interpreted.
Customer experience map #ideation #concepts #research #design #issue analysis #remote-friendly Customer experience mapping is a method of documenting and visualizing the experience a customer has as they use the product or service. It also maps out their responses to their experiences. To be used when there is a solution (even in a conceptual stage) that can be analyzed.
Risk management
Managing risk is an often overlooked part of the problem solving process. Solutions are often developed with the intention of reducing exposure to risk or solving issues that create risk but sometimes, great solutions are more experimental in nature and as such, deploying them needs to be carefully considered.
Managing risk means acknowledging that there may be risks associated with more out of the box solutions or trying new things, but that this must be measured against the possible benefits and other organizational factors.
Be informed, get the right data and stakeholders in the room and you can appropriately factor risk into your decision making process.
Decisions, Decisions… #communication #decision making #thiagi #action #issue analysis When it comes to decision-making, why are some of us more prone to take risks while others are risk-averse? One explanation might be the way the decision and options were presented. This exercise, based on Kahneman and Tversky’s classic study , illustrates how the framing effect influences our judgement and our ability to make decisions . The participants are divided into two groups. Both groups are presented with the same problem and two alternative programs for solving them. The two programs both have the same consequences but are presented differently. The debriefing discussion examines how the framing of the program impacted the participant’s decision.
Team-building
No single person is as good at problem solving as a team. Building an effective team and helping them come together around a common purpose is one of the most important problem solving skills, doubly so for leaders. By bringing a team together and helping them work efficiently, you pave the way for team ownership of a problem and the development of effective solutions.
In a problem solving workshop, it can be tempting to jump right into the deep end, though taking the time to break the ice, energize the team and align them with a game or exercise will pay off over the course of the day.
Remember that you will likely go through the problem solving process multiple times over an organization’s lifespan and building a strong team culture will make future problem solving more effective. It’s also great to work with people you know, trust and have fun with. Working on team building in and out of the problem solving process is a hallmark of successful teams that can work together to solve business problems.
9 Dimensions Team Building Activity #ice breaker #teambuilding #team #remote-friendly 9 Dimensions is a powerful activity designed to build relationships and trust among team members. There are 2 variations of this icebreaker. The first version is for teams who want to get to know each other better. The second version is for teams who want to explore how they are working together as a team.
Time management
The problem solving process is designed to lead a team from identifying a problem through to delivering a solution and evaluating its effectiveness. Without effective time management skills or timeboxing of tasks, it can be easy for a team to get bogged down or be inefficient.
By using a problem solving model and carefully designing your workshop, you can allocate time efficiently and trust that the process will deliver the results you need in a good timeframe.
Time management also comes into play when it comes to rolling out solutions, particularly those that are experimental in nature. Having a clear timeframe for implementing and evaluating solutions is vital for ensuring their success and being able to pivot if necessary.
Improving your skills at problem solving is often a career-long pursuit though there are methods you can use to make the learning process more efficient and to supercharge your problem solving skillset.
Remember that the skills you need to be a great problem solver have a large overlap with those skills you need to be effective in any role. Investing time and effort to develop your active listening or critical thinking skills is valuable in any context. Here are 7 ways to improve your problem solving skills.
Share best practices
Remember that your team is an excellent source of skills, wisdom, and techniques and that you should all take advantage of one another where possible. Best practices that one team has for solving problems, conducting research or making decisions should be shared across the organization. If you have in-house staff that have done active listening training or are data analysis pros, have them lead a training session.
Your team is one of your best resources. Create space and internal processes for the sharing of skills so that you can all grow together.
Ask for help and attend training
Once you’ve figured out you have a skills gap, the next step is to take action to fill that skills gap. That might be by asking your superior for training or coaching, or liaising with team members with that skill set. You might even attend specialized training for certain skills – active listening or critical thinking, for example, are business-critical skills that are regularly offered as part of a training scheme.
Whatever method you choose, remember that taking action of some description is necessary for growth. Whether that means practicing, getting help, attending training or doing some background reading, taking active steps to improve your skills is the way to go.
Learn a process
Problem solving can be complicated, particularly when attempting to solve large problems for the first time. Using a problem solving process helps give structure to your problem solving efforts and focus on creating outcomes, rather than worrying about the format.
Tools such as the seven-step problem solving process above are effective because not only do they feature steps that will help a team solve problems, they also develop skills along the way. Each step asks for people to engage with the process using different skills and in doing so, helps the team learn and grow together. Group processes of varying complexity and purpose can also be found in the SessionLab library of facilitation techniques . Using a tried and tested process and really help ease the learning curve for both those leading such a process, as well as those undergoing the purpose.
Effective teams make decisions about where they should and shouldn’t expend additional effort. By using a problem solving process, you can focus on the things that matter, rather than stumbling towards a solution haphazardly.
Create a feedback loop
Some skills gaps are more obvious than others. It’s possible that your perception of your active listening skills differs from those of your colleagues.
It’s valuable to create a system where team members can provide feedback in an ordered and friendly manner so they can all learn from one another. Only by identifying areas of improvement can you then work to improve them.
Remember that feedback systems require oversight and consideration so that they don’t turn into a place to complain about colleagues. Design the system intelligently so that you encourage the creation of learning opportunities, rather than encouraging people to list their pet peeves.
While practice might not make perfect, it does make the problem solving process easier. If you are having trouble with critical thinking, don’t shy away from doing it. Get involved where you can and stretch those muscles as regularly as possible.
Problem solving skills come more naturally to some than to others and that’s okay. Take opportunities to get involved and see where you can practice your skills in situations outside of a workshop context. Try collaborating in other circumstances at work or conduct data analysis on your own projects. You can often develop those skills you need for problem solving simply by doing them. Get involved!
Use expert exercises and methods
Learn from the best. Our library of 700+ facilitation techniques is full of activities and methods that help develop the skills you need to be an effective problem solver. Check out our templates to see how to approach problem solving and other organizational challenges in a structured and intelligent manner.
There is no single approach to improving problem solving skills, but by using the techniques employed by others you can learn from their example and develop processes that have seen proven results.
Try new ways of thinking and change your mindset
Using tried and tested exercises that you know well can help deliver results, but you do run the risk of missing out on the learning opportunities offered by new approaches. As with the problem solving process, changing your mindset can remove blockages and be used to develop your problem solving skills.
Most teams have members with mixed skill sets and specialties. Mix people from different teams and share skills and different points of view. Teach your customer support team how to use design thinking methods or help your developers with conflict resolution techniques. Try switching perspectives with facilitation techniques like Flip It! or by using new problem solving methodologies or models. Give design thinking, liberating structures or lego serious play a try if you want to try a new approach. You will find that framing problems in new ways and using existing skills in new contexts can be hugely useful for personal development and improving your skillset. It’s also a lot of fun to try new things. Give it a go!
Encountering business challenges and needing to find appropriate solutions is not unique to your organization. Lots of very smart people have developed methods, theories and approaches to help develop problem solving skills and create effective solutions. Learn from them!
Books like The Art of Thinking Clearly , Think Smarter, or Thinking Fast, Thinking Slow are great places to start, though it’s also worth looking at blogs related to organizations facing similar problems to yours, or browsing for success stories. Seeing how Dropbox massively increased growth and working backward can help you see the skills or approach you might be lacking to solve that same problem. Learning from others by reading their stories or approaches can be time-consuming but ultimately rewarding.
A tired, distracted mind is not in the best position to learn new skills. It can be tempted to burn the candle at both ends and develop problem solving skills outside of work. Absolutely use your time effectively and take opportunities for self-improvement, though remember that rest is hugely important and that without letting your brain rest, you cannot be at your most effective.
Creating distance between yourself and the problem you might be facing can also be useful. By letting an idea sit, you can find that a better one presents itself or you can develop it further. Take regular breaks when working and create a space for downtime. Remember that working smarter is preferable to working harder and that self-care is important for any effective learning or improvement process.
Want to design better group processes?
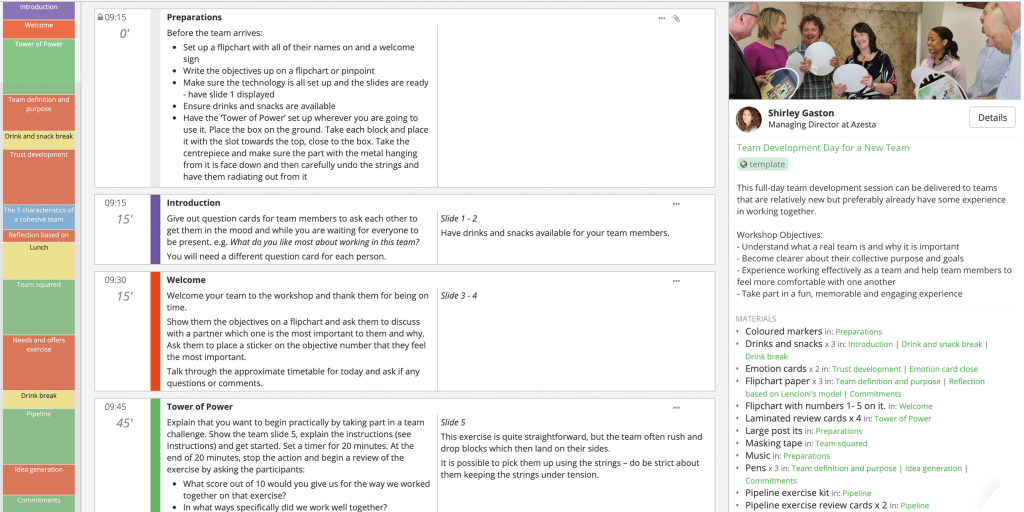
Over to you
Now we’ve explored some of the key problem solving skills and the problem solving steps necessary for an effective process, you’re ready to begin developing more effective solutions and leading problem solving workshops.
Need more inspiration? Check out our post on problem solving activities you can use when guiding a group towards a great solution in your next workshop or meeting. Have questions? Did you have a great problem solving technique you use with your team? Get in touch in the comments below. We’d love to chat!
Leave a Comment Cancel reply
Your email address will not be published. Required fields are marked *

Going from a mere idea to a workshop that delivers results for your clients can feel like a daunting task. In this piece, we will shine a light on all the work behind the scenes and help you learn how to plan a workshop from start to finish. On a good day, facilitation can feel like effortless magic, but that is mostly the result of backstage work, foresight, and a lot of careful planning. Read on to learn a step-by-step approach to breaking the process of planning a workshop into small, manageable chunks. The flow starts with the first meeting with a client to define the purposes of a workshop.…

How does learning work? A clever 9-year-old once told me: “I know I am learning something new when I am surprised.” The science of adult learning tells us that, in order to learn new skills (which, unsurprisingly, is harder for adults to do than kids) grown-ups need to first get into a specific headspace. In a business, this approach is often employed in a training session where employees learn new skills or work on professional development. But how do you ensure your training is effective? In this guide, we'll explore how to create an effective training session plan and run engaging training sessions. As team leader, project manager, or consultant,…
Facilitation is more and more recognized as a key component of work, as employers and society are faced with bigger and more complex problems and ideas. From facilitating meetings to big, multi-stakeholder strategy development workshops, the facilitator's skillset is more and more in demand. In this article, we will go through a list of the best online facilitation resources, including newsletters, podcasts, communities, and 10 free toolkits you can bookmark and read to upskill and improve your facilitation practice. When designing activities and workshops, you'll probably start by using templates and methods you are familiar with. Soon enough, you'll need to expand your range and look for facilitation methods and…
Design your next workshop with SessionLab
Join the 150,000 facilitators using SessionLab
Sign up for free
Using Psychology
Over fifty problem-solving strategies explained — 2022.
by ahoskin4 | Oct 15, 2018 | Problem solving , Social Support | 26 comments

By John Malouff, Ph.D., J.D.
The comprehensive nature of the list of problem solving strategies allows individuals to use a checklist approach to problem solving. It also could facilitate training others in problem solving. The classification of the strategies into types may facilitate the development of new strategies that fit into a specific category. The explanations and examples given could serve as a valuable supplement to other explanations and examples available in books and on the web.
The strategies on this list are in themselves not original. The original aspects of this list are:
- putting all these specific strategies together
- organizing them into the types described below
- giving each type of strategy a fresh explanation with new examples.
Problem-solving strategies explained, with examples
Strategies to help you understand the problem.
It is easier to solve a specific problem than a vague one. So clarify the problem before you start looking for a solution. If your problem is that your spouse tells you that you are not supportive enough, find out what he or she means by supportive. If your problem is that your mother can't get the new software to work, determine what doesn't happen that she wants to happen. If your problem is a math homework question, read carefully the question (usually at the end):Is the answer supposed to be in metres or centimetres, rounded or not, square or not, etc.
Strategies to help you simplify the task
Strategies to help you determine the cause of the problem, strategies involving the use of external aids to help you identify possible solutions, strategies involving the use of logic to help you identify possible solutions, strategies using a possible solution as a starting point to help you solve a problem, strategies to help you determine which possible solution is best, strategies using geometry for problem solving, strategies to help you function optimally while problem solving, strategies to help you solve multiple problems, sources of the list.
The strategies in this document come from a variety of sources, many of which have long since faded from my memory. Some of the ideas were previously described in the following references, which provide a wealth of examples:
D’Zurilla, T.J., & Goldfried, M.R. (1971). Problem solving and behaviour modification. Journal of Abnormal Psychology, 78, 104–126.
Fabian, J. (1990). Creative thinking & problem solving. Chelsea, MI:Lewis.
More information about Problem Solving
Harris, R. (2002). Problem solving techniques.
McNamara, C. (1999). Basic guidelines to problem solving and decision making.
Wikipedia (2006). Problem solving.
About the author
John Malouff , Ph.D., J.D., earned a law degree from the University of Colorado in 1979 and a Ph.D. in clinical psychology from Arizona State University in 1984. He currently works as an associate professor of psychology at the University of New England, in Armidale, Australia. He has co-authored five books and several dozen articles in scientific journals.
26 Comments

I got a lot of in for information from this.

Great! Thanks for your comment, McKenzie. With help from a technician at the University of New England, Australia, I recently moved my public-service web sites to my blog. Now readers can comment and ask questions.

Thanks for sharing John. The examples are brief but nice and easy to read through. I had a laugh at the reference to “New VCR” in the first example. I actually still have one believe it or not.
Hi McKenzie. I too still have a VCR.

I learned a lot of information using this article!
Hi Emma. Thanks for the feedback!

Thank you John for sharing your efforts .You are very generous. Your work covers so many ways to look at problem solving. ps I was never any good at geometry !but there are plenty of other strategies .
Thanks for the positive comment, Dinah.

I am writing a book on critical thinking and evidence-based management for healthcare managers and administrators and would like your permission to include these strategies. I will provide proper attribution, including your name and link to the blog post. Thank you
Hi Frank. You may include the strategies. Best wishes for the book. John

Do you have a format or curriculum these could be used in a group structure?
Hi Erin. I do not. I assign the set of strategies in my Behavior Modification course as part of covering cognitive therapy methods. Maybe you will create something of the sort you mention.
Thank you so much. I am working on building a curriculum for a group with co-occurring disorders. And i found this information to be helpful with starting.

As always, such clear and concise instruction that can easily be applied to every day situations. Thank you

Thank you for putting this together. I found a lot of useful information here.
You’re welcome.

This resource was shared with us at our annual AISH (Academy for International School Heads) gathering. around 400 heads of schools were using this helpful resource! Thank you for posting and sharing this with us
Great! Thanks, Monique. The more people who use the methods, the better.

I learned a lot from reading this article. I realized so many things and I found many information here that is applicable in everyday situations.
Thank you so much for compiling all this information. 😀

Absolutely enjoyed reading these articles. I learned a lot of things that I never really thought about.

I have been reading how to solve problems, even before they start, once you have them and strategies to process, and this is the best I have found. Thank you for sharing to all of us!

I learned quite a bit but there was some things I struggled with
Great job! Efficient strategies and very informative.

Amazing breakdown to every example/strategies! Learned quite a bit of new ways to figure out solutions. Thank you!
Submit a Comment
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
Submit Comment

Subscribe by Email
You can unsubscribe at any time.
Please, insert a valid email.
Thank you, your email will be added to the mailing list once you click on the link in the confirmation email.
Spam protection has stopped this request. Please contact site owner for help.
This form is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
Blog categories
- Behaviour Modification
- Bereavement and Grief
- Child Psychology
- Cursing and Swearing
- Health-related behavior
- Human Thinking and Behavior
- Job hunting
- law and psychology
- Mental health problems
- Observational learning
- Organizational Psychology
- Parenting Support
- Personality
- Political psychology
- Positive psychology
- Problem solving
- Psychotherapy
- romantic relationships
- Sexual assault
- Social psychology
- Social Support
- Strategies for Teachers
- Uncategorized
- Weight control
- Weight Loss
Suggestions or feedback?
MIT News | Massachusetts Institute of Technology
- Machine learning
- Social justice
- Black holes
- Classes and programs
Departments
- Aeronautics and Astronautics
- Brain and Cognitive Sciences
- Architecture
- Political Science
- Mechanical Engineering
Centers, Labs, & Programs
- Abdul Latif Jameel Poverty Action Lab (J-PAL)
- Picower Institute for Learning and Memory
- Lincoln Laboratory
- School of Architecture + Planning
- School of Engineering
- School of Humanities, Arts, and Social Sciences
- Sloan School of Management
- School of Science
- MIT Schwarzman College of Computing
Solve at MIT 2022: Demystifying world issues one connection at a time
Press contact :.

Previous image Next image
The world entered 2022 with growing weariness after two years of a global pandemic that has claimed 5.61 million lives , and continuing humanitarian and climate crises, with energy-related emissions set to rise by 87 million metric tonnes (about 96 million tons), and 274 million people in need of lifesaving humanitarian assistance.
None of these issues has simple fixes. However, we retain our sense of optimism and purpose knowing that there are innovators working tirelessly around the world to solve these challenges one idea at a time.
Solve at MIT 2022 , the flagship event of MIT Solve , recently convened over 300 social impact leaders including 62 Solver teams as well as thousands of virtual supporters. The May 5-7 event featured plenaries where leaders from various sectors discussed the state of global issues and how technology can contribute to making us more resilient. Throughout the three days, Solver teams , members, and supporters joined over a dozen working sessions to discuss the progress and obstacles they were experiencing, and brainstorm how to scale their impact.
Below are a few of the many notable takeaways from Solve at MIT 2022.
There’s human capital at stake for every technological advancement
Technology has seemingly limitless capacity to solve some of the world's biggest challenges, but developing and deploying it comes with its own concerns. Some of the most dangerous consequences of technological development are human and land degradation.
Within the opening plenary, Ethical and Inclusive Innovation: Solving With, By and For the Most Underserved , Azra Akšamija, director of the Art, Culture and Technology program at MIT and the Future Heritage Lab, shared, “When we work with fragile communities we always have the best intentions, but best intentions don't always make the best solutions.” Power dynamics and especially colonial dynamics can impact the effectiveness of well-intended initiatives or innovation.
While discussing Vodafone's partnership with Waking Women Healing Institute , June Sugiyama, director of Vodafone Americas Foundation, asked Indigenous Fellow Kristen Welch, its executive director, how other companies can help support innovators and entrepreneurs. Welch boldly called on us all to first and foremost decolonize, which includes looking internally and at budget streams and policies. She said, “Decolonize yourself and make sure you have BIPOC and two-spirit people at every level of decision-making within your company and institution and corporation.”

Previous item Next item
Yuval Noah Harari, historian, bestselling author, and co-founder of Sapienship, reminded us that we also have the freedom to choose ethical innovation and to consider the consequences of our actions. He shared, “People who design technology have enormous power to shape and reshape the world. They have choices. You can design many different types of technologies, not just one, it’s never deterministic … you can, as an engineer, as an entrepreneur, create a technological tool for a government to survey and monitor citizens, or you can create the opposite tool for citizens to monitor the government.”
Impact investment does not equate to charity
During the Investing in Community-Led Solutions plenary, Hala Hanna, managing director of Solve stated, “Charity asks: what’s wrong, how can I help? Justice asks: why is it happening, how can I change it?”
In addition to mentorship and expert consulting, funding and creating monetary partnerships can play a critical role in the success of innovators looking to improve the world. Impact investing has grown tremendously in the last decade, but there is still a misrepresentation of what it should look like.
In the plenary, Angela Jackson, chief ecosystem investment officer at Kapor Enterprises, asserted, “We invest with an impact lens but we also want returns. We don't want the narrative to be that when you invest in Black, Latinx, or Indigenous communities that you’re expecting concessionary returns. In those communities, there is the same genius, right? They’re solving problems for their communities. Our ethos is, yes we’re going to get impact, but also we can expect returns … I’d like to see investors think beyond [investing] because it’s the moral thing to do or the charitable thing to do, but really doing it in service of equity and in service of efficiency.”
Jeffrey Cry, managing partner at Raven Indigenous Capital Partners, echoed Jackson’s sentiments, saying, “We don’t want charitable investing at all. The businesses we invest in we see as best-in-class business, not best-in-Indigenous investments — best in class.”
Even with impact investments made — performative or not — corporations must be held accountable past initial commitments. To exemplify a bona fide commitment to social justice, Vilas Dhar, president and trustee and the Patrick J. Mcgovern Foundation, awarded Kimberly Seals Allers, founder of the IRTH App , the 2022 AI for Humanity Prize at the conclusion of the program. Seals Allers and Irth are helping to address racism and bias in maternity and infant care.
Start alone but don’t stay alone
There may be a time in your life when you feel compelled to solve a problem, and there may be no one else available to take action with you. In those times, Sakena Yacoobi, founder and president of the Afghan Institute of Learning , implores us all to be bold. “Don't wait for something to come, you need to act on it yourself.”

Anne Wojcicki, founder and CEO of 23andMe, shared during the plenary Promoting Our Care Providers that she was also no stranger to initiating change, even if it meant taking an unconventional approach. Wojcicki left her life on Wall Street to empower health through human genome-centered solutions and break the one-size-fits-all approach that the health care industry has been practicing. “I’m going to set up a different kind of health care system that is based on what’s in your best interest. Everything that [23andMe] does now has been controversial because it is not part of the system at all. And that was intentional from the very beginning,” stated Wojcicki.
Although breakthroughs and initiatives to solve world challenges do sometimes call for the action of an individual, Thanasi Dilos, co-founder of Civics Unplugged and Solv[ED] judge, reminded us that community support leads to better outcomes. During the Closing Plenary: Young Leaders on the Horizon , Dilos shared, “Funding is great for young people, but what is really also important is community and agency.” Adding also, “No one is self-made — everyone is made in community.”
What’s next for Solve?
Linda Henry , CEO of Boston Globe Media and Solve advisor, summarized well, “Solve is a catalytic convener to bring people together.”
The three-day event was only a fraction of the dialogue and idea exchange that needs to happen in order to tackle global issues, but it’s necessary to start somewhere.

Leveling the playing field in the care economy , figuring out how to uplift proximate leaders , and addressing lofty goals like net-zero are no easy feat. However, finding the solution to many world problems might be as simple as catalyzing connections like putting together an innovator and a funder who live in different time zones. Or it might mean looking internally and holding ourselves accountable to spearhead a new solution.
Noubar Afeyan, co-founder and chairman at Moderna and Solve advisor, left attendees with a note of encouragement, “When you find yourself in survival mode, don’t assume that you’re failing, because you could be close to a breakthrough.”
Share this news article on:
Related links.
- Videos: Solve at MIT 2022
- Article: "Innovation doesn’t mean what you think it does"
Related Topics
- Art, Culture and Technology
- Special events and guest speakers
- Sustainability
- Innovation and Entrepreneurship (I&E)
Related Articles

An expanded commitment to Indigenous scholarship and community at MIT
MIT Solve announces 2022 global challenges and the Indigenous Communities Fellowship
![Golden-toned photo of a young woman holding an armload of folders and "MIT SOLV[ED]" superimposed](https://news.mit.edu/sites/default/files/styles/news_article__archive/public/images/202105/Solv%5BED%5D.png?itok=-oUgIaia "problem solving 2022")
Solv[ED] inspires young people to become global problem-solvers

Solve sparks powerful impact on global challenges
More mit news.

Study: Titan’s lakes may be shaped by waves
Read full story →

3 Questions: Catherine D’Ignazio on data science and a quest for justice

Microscope system sharpens scientists’ view of neural circuit connections

Arvind, longtime MIT professor and prolific computer scientist, dies at 77

MIT-Takeda Program wraps up with 16 publications, a patent, and nearly two dozen projects completed

David Autor named the inaugural Daniel (1972) and Gail Rubinfeld Professor in Economics
- More news on MIT News homepage →
Massachusetts Institute of Technology 77 Massachusetts Avenue, Cambridge, MA, USA
- Map (opens in new window)
- Events (opens in new window)
- People (opens in new window)
- Careers (opens in new window)
- Accessibility
- Social Media Hub
- MIT on Facebook
- MIT on YouTube
- MIT on Instagram
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Review Article
- Open access
- Published: 11 January 2023
The effectiveness of collaborative problem solving in promoting students’ critical thinking: A meta-analysis based on empirical literature
- Enwei Xu ORCID: orcid.org/0000-0001-6424-8169 1 ,
- Wei Wang 1 &
- Qingxia Wang 1
Humanities and Social Sciences Communications volume 10 , Article number: 16 ( 2023 ) Cite this article
16k Accesses
18 Citations
3 Altmetric
Metrics details
- Science, technology and society
Collaborative problem-solving has been widely embraced in the classroom instruction of critical thinking, which is regarded as the core of curriculum reform based on key competencies in the field of education as well as a key competence for learners in the 21st century. However, the effectiveness of collaborative problem-solving in promoting students’ critical thinking remains uncertain. This current research presents the major findings of a meta-analysis of 36 pieces of the literature revealed in worldwide educational periodicals during the 21st century to identify the effectiveness of collaborative problem-solving in promoting students’ critical thinking and to determine, based on evidence, whether and to what extent collaborative problem solving can result in a rise or decrease in critical thinking. The findings show that (1) collaborative problem solving is an effective teaching approach to foster students’ critical thinking, with a significant overall effect size (ES = 0.82, z = 12.78, P < 0.01, 95% CI [0.69, 0.95]); (2) in respect to the dimensions of critical thinking, collaborative problem solving can significantly and successfully enhance students’ attitudinal tendencies (ES = 1.17, z = 7.62, P < 0.01, 95% CI[0.87, 1.47]); nevertheless, it falls short in terms of improving students’ cognitive skills, having only an upper-middle impact (ES = 0.70, z = 11.55, P < 0.01, 95% CI[0.58, 0.82]); and (3) the teaching type (chi 2 = 7.20, P < 0.05), intervention duration (chi 2 = 12.18, P < 0.01), subject area (chi 2 = 13.36, P < 0.05), group size (chi 2 = 8.77, P < 0.05), and learning scaffold (chi 2 = 9.03, P < 0.01) all have an impact on critical thinking, and they can be viewed as important moderating factors that affect how critical thinking develops. On the basis of these results, recommendations are made for further study and instruction to better support students’ critical thinking in the context of collaborative problem-solving.
Similar content being viewed by others

Testing theory of mind in large language models and humans

Cognitive control training with domain-general response inhibition does not change children’s brains or behavior

Impact of artificial intelligence on human loss in decision making, laziness and safety in education
Introduction.
Although critical thinking has a long history in research, the concept of critical thinking, which is regarded as an essential competence for learners in the 21st century, has recently attracted more attention from researchers and teaching practitioners (National Research Council, 2012 ). Critical thinking should be the core of curriculum reform based on key competencies in the field of education (Peng and Deng, 2017 ) because students with critical thinking can not only understand the meaning of knowledge but also effectively solve practical problems in real life even after knowledge is forgotten (Kek and Huijser, 2011 ). The definition of critical thinking is not universal (Ennis, 1989 ; Castle, 2009 ; Niu et al., 2013 ). In general, the definition of critical thinking is a self-aware and self-regulated thought process (Facione, 1990 ; Niu et al., 2013 ). It refers to the cognitive skills needed to interpret, analyze, synthesize, reason, and evaluate information as well as the attitudinal tendency to apply these abilities (Halpern, 2001 ). The view that critical thinking can be taught and learned through curriculum teaching has been widely supported by many researchers (e.g., Kuncel, 2011 ; Leng and Lu, 2020 ), leading to educators’ efforts to foster it among students. In the field of teaching practice, there are three types of courses for teaching critical thinking (Ennis, 1989 ). The first is an independent curriculum in which critical thinking is taught and cultivated without involving the knowledge of specific disciplines; the second is an integrated curriculum in which critical thinking is integrated into the teaching of other disciplines as a clear teaching goal; and the third is a mixed curriculum in which critical thinking is taught in parallel to the teaching of other disciplines for mixed teaching training. Furthermore, numerous measuring tools have been developed by researchers and educators to measure critical thinking in the context of teaching practice. These include standardized measurement tools, such as WGCTA, CCTST, CCTT, and CCTDI, which have been verified by repeated experiments and are considered effective and reliable by international scholars (Facione and Facione, 1992 ). In short, descriptions of critical thinking, including its two dimensions of attitudinal tendency and cognitive skills, different types of teaching courses, and standardized measurement tools provide a complex normative framework for understanding, teaching, and evaluating critical thinking.
Cultivating critical thinking in curriculum teaching can start with a problem, and one of the most popular critical thinking instructional approaches is problem-based learning (Liu et al., 2020 ). Duch et al. ( 2001 ) noted that problem-based learning in group collaboration is progressive active learning, which can improve students’ critical thinking and problem-solving skills. Collaborative problem-solving is the organic integration of collaborative learning and problem-based learning, which takes learners as the center of the learning process and uses problems with poor structure in real-world situations as the starting point for the learning process (Liang et al., 2017 ). Students learn the knowledge needed to solve problems in a collaborative group, reach a consensus on problems in the field, and form solutions through social cooperation methods, such as dialogue, interpretation, questioning, debate, negotiation, and reflection, thus promoting the development of learners’ domain knowledge and critical thinking (Cindy, 2004 ; Liang et al., 2017 ).
Collaborative problem-solving has been widely used in the teaching practice of critical thinking, and several studies have attempted to conduct a systematic review and meta-analysis of the empirical literature on critical thinking from various perspectives. However, little attention has been paid to the impact of collaborative problem-solving on critical thinking. Therefore, the best approach for developing and enhancing critical thinking throughout collaborative problem-solving is to examine how to implement critical thinking instruction; however, this issue is still unexplored, which means that many teachers are incapable of better instructing critical thinking (Leng and Lu, 2020 ; Niu et al., 2013 ). For example, Huber ( 2016 ) provided the meta-analysis findings of 71 publications on gaining critical thinking over various time frames in college with the aim of determining whether critical thinking was truly teachable. These authors found that learners significantly improve their critical thinking while in college and that critical thinking differs with factors such as teaching strategies, intervention duration, subject area, and teaching type. The usefulness of collaborative problem-solving in fostering students’ critical thinking, however, was not determined by this study, nor did it reveal whether there existed significant variations among the different elements. A meta-analysis of 31 pieces of educational literature was conducted by Liu et al. ( 2020 ) to assess the impact of problem-solving on college students’ critical thinking. These authors found that problem-solving could promote the development of critical thinking among college students and proposed establishing a reasonable group structure for problem-solving in a follow-up study to improve students’ critical thinking. Additionally, previous empirical studies have reached inconclusive and even contradictory conclusions about whether and to what extent collaborative problem-solving increases or decreases critical thinking levels. As an illustration, Yang et al. ( 2008 ) carried out an experiment on the integrated curriculum teaching of college students based on a web bulletin board with the goal of fostering participants’ critical thinking in the context of collaborative problem-solving. These authors’ research revealed that through sharing, debating, examining, and reflecting on various experiences and ideas, collaborative problem-solving can considerably enhance students’ critical thinking in real-life problem situations. In contrast, collaborative problem-solving had a positive impact on learners’ interaction and could improve learning interest and motivation but could not significantly improve students’ critical thinking when compared to traditional classroom teaching, according to research by Naber and Wyatt ( 2014 ) and Sendag and Odabasi ( 2009 ) on undergraduate and high school students, respectively.
The above studies show that there is inconsistency regarding the effectiveness of collaborative problem-solving in promoting students’ critical thinking. Therefore, it is essential to conduct a thorough and trustworthy review to detect and decide whether and to what degree collaborative problem-solving can result in a rise or decrease in critical thinking. Meta-analysis is a quantitative analysis approach that is utilized to examine quantitative data from various separate studies that are all focused on the same research topic. This approach characterizes the effectiveness of its impact by averaging the effect sizes of numerous qualitative studies in an effort to reduce the uncertainty brought on by independent research and produce more conclusive findings (Lipsey and Wilson, 2001 ).
This paper used a meta-analytic approach and carried out a meta-analysis to examine the effectiveness of collaborative problem-solving in promoting students’ critical thinking in order to make a contribution to both research and practice. The following research questions were addressed by this meta-analysis:
What is the overall effect size of collaborative problem-solving in promoting students’ critical thinking and its impact on the two dimensions of critical thinking (i.e., attitudinal tendency and cognitive skills)?
How are the disparities between the study conclusions impacted by various moderating variables if the impacts of various experimental designs in the included studies are heterogeneous?
This research followed the strict procedures (e.g., database searching, identification, screening, eligibility, merging, duplicate removal, and analysis of included studies) of Cooper’s ( 2010 ) proposed meta-analysis approach for examining quantitative data from various separate studies that are all focused on the same research topic. The relevant empirical research that appeared in worldwide educational periodicals within the 21st century was subjected to this meta-analysis using Rev-Man 5.4. The consistency of the data extracted separately by two researchers was tested using Cohen’s kappa coefficient, and a publication bias test and a heterogeneity test were run on the sample data to ascertain the quality of this meta-analysis.
Data sources and search strategies
There were three stages to the data collection process for this meta-analysis, as shown in Fig. 1 , which shows the number of articles included and eliminated during the selection process based on the statement and study eligibility criteria.

This flowchart shows the number of records identified, included and excluded in the article.
First, the databases used to systematically search for relevant articles were the journal papers of the Web of Science Core Collection and the Chinese Core source journal, as well as the Chinese Social Science Citation Index (CSSCI) source journal papers included in CNKI. These databases were selected because they are credible platforms that are sources of scholarly and peer-reviewed information with advanced search tools and contain literature relevant to the subject of our topic from reliable researchers and experts. The search string with the Boolean operator used in the Web of Science was “TS = (((“critical thinking” or “ct” and “pretest” or “posttest”) or (“critical thinking” or “ct” and “control group” or “quasi experiment” or “experiment”)) and (“collaboration” or “collaborative learning” or “CSCL”) and (“problem solving” or “problem-based learning” or “PBL”))”. The research area was “Education Educational Research”, and the search period was “January 1, 2000, to December 30, 2021”. A total of 412 papers were obtained. The search string with the Boolean operator used in the CNKI was “SU = (‘critical thinking’*‘collaboration’ + ‘critical thinking’*‘collaborative learning’ + ‘critical thinking’*‘CSCL’ + ‘critical thinking’*‘problem solving’ + ‘critical thinking’*‘problem-based learning’ + ‘critical thinking’*‘PBL’ + ‘critical thinking’*‘problem oriented’) AND FT = (‘experiment’ + ‘quasi experiment’ + ‘pretest’ + ‘posttest’ + ‘empirical study’)” (translated into Chinese when searching). A total of 56 studies were found throughout the search period of “January 2000 to December 2021”. From the databases, all duplicates and retractions were eliminated before exporting the references into Endnote, a program for managing bibliographic references. In all, 466 studies were found.
Second, the studies that matched the inclusion and exclusion criteria for the meta-analysis were chosen by two researchers after they had reviewed the abstracts and titles of the gathered articles, yielding a total of 126 studies.
Third, two researchers thoroughly reviewed each included article’s whole text in accordance with the inclusion and exclusion criteria. Meanwhile, a snowball search was performed using the references and citations of the included articles to ensure complete coverage of the articles. Ultimately, 36 articles were kept.
Two researchers worked together to carry out this entire process, and a consensus rate of almost 94.7% was reached after discussion and negotiation to clarify any emerging differences.
Eligibility criteria
Since not all the retrieved studies matched the criteria for this meta-analysis, eligibility criteria for both inclusion and exclusion were developed as follows:
The publication language of the included studies was limited to English and Chinese, and the full text could be obtained. Articles that did not meet the publication language and articles not published between 2000 and 2021 were excluded.
The research design of the included studies must be empirical and quantitative studies that can assess the effect of collaborative problem-solving on the development of critical thinking. Articles that could not identify the causal mechanisms by which collaborative problem-solving affects critical thinking, such as review articles and theoretical articles, were excluded.
The research method of the included studies must feature a randomized control experiment or a quasi-experiment, or a natural experiment, which have a higher degree of internal validity with strong experimental designs and can all plausibly provide evidence that critical thinking and collaborative problem-solving are causally related. Articles with non-experimental research methods, such as purely correlational or observational studies, were excluded.
The participants of the included studies were only students in school, including K-12 students and college students. Articles in which the participants were non-school students, such as social workers or adult learners, were excluded.
The research results of the included studies must mention definite signs that may be utilized to gauge critical thinking’s impact (e.g., sample size, mean value, or standard deviation). Articles that lacked specific measurement indicators for critical thinking and could not calculate the effect size were excluded.
Data coding design
In order to perform a meta-analysis, it is necessary to collect the most important information from the articles, codify that information’s properties, and convert descriptive data into quantitative data. Therefore, this study designed a data coding template (see Table 1 ). Ultimately, 16 coding fields were retained.
The designed data-coding template consisted of three pieces of information. Basic information about the papers was included in the descriptive information: the publishing year, author, serial number, and title of the paper.
The variable information for the experimental design had three variables: the independent variable (instruction method), the dependent variable (critical thinking), and the moderating variable (learning stage, teaching type, intervention duration, learning scaffold, group size, measuring tool, and subject area). Depending on the topic of this study, the intervention strategy, as the independent variable, was coded into collaborative and non-collaborative problem-solving. The dependent variable, critical thinking, was coded as a cognitive skill and an attitudinal tendency. And seven moderating variables were created by grouping and combining the experimental design variables discovered within the 36 studies (see Table 1 ), where learning stages were encoded as higher education, high school, middle school, and primary school or lower; teaching types were encoded as mixed courses, integrated courses, and independent courses; intervention durations were encoded as 0–1 weeks, 1–4 weeks, 4–12 weeks, and more than 12 weeks; group sizes were encoded as 2–3 persons, 4–6 persons, 7–10 persons, and more than 10 persons; learning scaffolds were encoded as teacher-supported learning scaffold, technique-supported learning scaffold, and resource-supported learning scaffold; measuring tools were encoded as standardized measurement tools (e.g., WGCTA, CCTT, CCTST, and CCTDI) and self-adapting measurement tools (e.g., modified or made by researchers); and subject areas were encoded according to the specific subjects used in the 36 included studies.
The data information contained three metrics for measuring critical thinking: sample size, average value, and standard deviation. It is vital to remember that studies with various experimental designs frequently adopt various formulas to determine the effect size. And this paper used Morris’ proposed standardized mean difference (SMD) calculation formula ( 2008 , p. 369; see Supplementary Table S3 ).
Procedure for extracting and coding data
According to the data coding template (see Table 1 ), the 36 papers’ information was retrieved by two researchers, who then entered them into Excel (see Supplementary Table S1 ). The results of each study were extracted separately in the data extraction procedure if an article contained numerous studies on critical thinking, or if a study assessed different critical thinking dimensions. For instance, Tiwari et al. ( 2010 ) used four time points, which were viewed as numerous different studies, to examine the outcomes of critical thinking, and Chen ( 2013 ) included the two outcome variables of attitudinal tendency and cognitive skills, which were regarded as two studies. After discussion and negotiation during data extraction, the two researchers’ consistency test coefficients were roughly 93.27%. Supplementary Table S2 details the key characteristics of the 36 included articles with 79 effect quantities, including descriptive information (e.g., the publishing year, author, serial number, and title of the paper), variable information (e.g., independent variables, dependent variables, and moderating variables), and data information (e.g., mean values, standard deviations, and sample size). Following that, testing for publication bias and heterogeneity was done on the sample data using the Rev-Man 5.4 software, and then the test results were used to conduct a meta-analysis.
Publication bias test
When the sample of studies included in a meta-analysis does not accurately reflect the general status of research on the relevant subject, publication bias is said to be exhibited in this research. The reliability and accuracy of the meta-analysis may be impacted by publication bias. Due to this, the meta-analysis needs to check the sample data for publication bias (Stewart et al., 2006 ). A popular method to check for publication bias is the funnel plot; and it is unlikely that there will be publishing bias when the data are equally dispersed on either side of the average effect size and targeted within the higher region. The data are equally dispersed within the higher portion of the efficient zone, consistent with the funnel plot connected with this analysis (see Fig. 2 ), indicating that publication bias is unlikely in this situation.

This funnel plot shows the result of publication bias of 79 effect quantities across 36 studies.
Heterogeneity test
To select the appropriate effect models for the meta-analysis, one might use the results of a heterogeneity test on the data effect sizes. In a meta-analysis, it is common practice to gauge the degree of data heterogeneity using the I 2 value, and I 2 ≥ 50% is typically understood to denote medium-high heterogeneity, which calls for the adoption of a random effect model; if not, a fixed effect model ought to be applied (Lipsey and Wilson, 2001 ). The findings of the heterogeneity test in this paper (see Table 2 ) revealed that I 2 was 86% and displayed significant heterogeneity ( P < 0.01). To ensure accuracy and reliability, the overall effect size ought to be calculated utilizing the random effect model.
The analysis of the overall effect size
This meta-analysis utilized a random effect model to examine 79 effect quantities from 36 studies after eliminating heterogeneity. In accordance with Cohen’s criterion (Cohen, 1992 ), it is abundantly clear from the analysis results, which are shown in the forest plot of the overall effect (see Fig. 3 ), that the cumulative impact size of cooperative problem-solving is 0.82, which is statistically significant ( z = 12.78, P < 0.01, 95% CI [0.69, 0.95]), and can encourage learners to practice critical thinking.

This forest plot shows the analysis result of the overall effect size across 36 studies.
In addition, this study examined two distinct dimensions of critical thinking to better understand the precise contributions that collaborative problem-solving makes to the growth of critical thinking. The findings (see Table 3 ) indicate that collaborative problem-solving improves cognitive skills (ES = 0.70) and attitudinal tendency (ES = 1.17), with significant intergroup differences (chi 2 = 7.95, P < 0.01). Although collaborative problem-solving improves both dimensions of critical thinking, it is essential to point out that the improvements in students’ attitudinal tendency are much more pronounced and have a significant comprehensive effect (ES = 1.17, z = 7.62, P < 0.01, 95% CI [0.87, 1.47]), whereas gains in learners’ cognitive skill are slightly improved and are just above average. (ES = 0.70, z = 11.55, P < 0.01, 95% CI [0.58, 0.82]).
The analysis of moderator effect size
The whole forest plot’s 79 effect quantities underwent a two-tailed test, which revealed significant heterogeneity ( I 2 = 86%, z = 12.78, P < 0.01), indicating differences between various effect sizes that may have been influenced by moderating factors other than sampling error. Therefore, exploring possible moderating factors that might produce considerable heterogeneity was done using subgroup analysis, such as the learning stage, learning scaffold, teaching type, group size, duration of the intervention, measuring tool, and the subject area included in the 36 experimental designs, in order to further explore the key factors that influence critical thinking. The findings (see Table 4 ) indicate that various moderating factors have advantageous effects on critical thinking. In this situation, the subject area (chi 2 = 13.36, P < 0.05), group size (chi 2 = 8.77, P < 0.05), intervention duration (chi 2 = 12.18, P < 0.01), learning scaffold (chi 2 = 9.03, P < 0.01), and teaching type (chi 2 = 7.20, P < 0.05) are all significant moderators that can be applied to support the cultivation of critical thinking. However, since the learning stage and the measuring tools did not significantly differ among intergroup (chi 2 = 3.15, P = 0.21 > 0.05, and chi 2 = 0.08, P = 0.78 > 0.05), we are unable to explain why these two factors are crucial in supporting the cultivation of critical thinking in the context of collaborative problem-solving. These are the precise outcomes, as follows:
Various learning stages influenced critical thinking positively, without significant intergroup differences (chi 2 = 3.15, P = 0.21 > 0.05). High school was first on the list of effect sizes (ES = 1.36, P < 0.01), then higher education (ES = 0.78, P < 0.01), and middle school (ES = 0.73, P < 0.01). These results show that, despite the learning stage’s beneficial influence on cultivating learners’ critical thinking, we are unable to explain why it is essential for cultivating critical thinking in the context of collaborative problem-solving.
Different teaching types had varying degrees of positive impact on critical thinking, with significant intergroup differences (chi 2 = 7.20, P < 0.05). The effect size was ranked as follows: mixed courses (ES = 1.34, P < 0.01), integrated courses (ES = 0.81, P < 0.01), and independent courses (ES = 0.27, P < 0.01). These results indicate that the most effective approach to cultivate critical thinking utilizing collaborative problem solving is through the teaching type of mixed courses.
Various intervention durations significantly improved critical thinking, and there were significant intergroup differences (chi 2 = 12.18, P < 0.01). The effect sizes related to this variable showed a tendency to increase with longer intervention durations. The improvement in critical thinking reached a significant level (ES = 0.85, P < 0.01) after more than 12 weeks of training. These findings indicate that the intervention duration and critical thinking’s impact are positively correlated, with a longer intervention duration having a greater effect.
Different learning scaffolds influenced critical thinking positively, with significant intergroup differences (chi 2 = 9.03, P < 0.01). The resource-supported learning scaffold (ES = 0.69, P < 0.01) acquired a medium-to-higher level of impact, the technique-supported learning scaffold (ES = 0.63, P < 0.01) also attained a medium-to-higher level of impact, and the teacher-supported learning scaffold (ES = 0.92, P < 0.01) displayed a high level of significant impact. These results show that the learning scaffold with teacher support has the greatest impact on cultivating critical thinking.
Various group sizes influenced critical thinking positively, and the intergroup differences were statistically significant (chi 2 = 8.77, P < 0.05). Critical thinking showed a general declining trend with increasing group size. The overall effect size of 2–3 people in this situation was the biggest (ES = 0.99, P < 0.01), and when the group size was greater than 7 people, the improvement in critical thinking was at the lower-middle level (ES < 0.5, P < 0.01). These results show that the impact on critical thinking is positively connected with group size, and as group size grows, so does the overall impact.
Various measuring tools influenced critical thinking positively, with significant intergroup differences (chi 2 = 0.08, P = 0.78 > 0.05). In this situation, the self-adapting measurement tools obtained an upper-medium level of effect (ES = 0.78), whereas the complete effect size of the standardized measurement tools was the largest, achieving a significant level of effect (ES = 0.84, P < 0.01). These results show that, despite the beneficial influence of the measuring tool on cultivating critical thinking, we are unable to explain why it is crucial in fostering the growth of critical thinking by utilizing the approach of collaborative problem-solving.
Different subject areas had a greater impact on critical thinking, and the intergroup differences were statistically significant (chi 2 = 13.36, P < 0.05). Mathematics had the greatest overall impact, achieving a significant level of effect (ES = 1.68, P < 0.01), followed by science (ES = 1.25, P < 0.01) and medical science (ES = 0.87, P < 0.01), both of which also achieved a significant level of effect. Programming technology was the least effective (ES = 0.39, P < 0.01), only having a medium-low degree of effect compared to education (ES = 0.72, P < 0.01) and other fields (such as language, art, and social sciences) (ES = 0.58, P < 0.01). These results suggest that scientific fields (e.g., mathematics, science) may be the most effective subject areas for cultivating critical thinking utilizing the approach of collaborative problem-solving.
The effectiveness of collaborative problem solving with regard to teaching critical thinking
According to this meta-analysis, using collaborative problem-solving as an intervention strategy in critical thinking teaching has a considerable amount of impact on cultivating learners’ critical thinking as a whole and has a favorable promotional effect on the two dimensions of critical thinking. According to certain studies, collaborative problem solving, the most frequently used critical thinking teaching strategy in curriculum instruction can considerably enhance students’ critical thinking (e.g., Liang et al., 2017 ; Liu et al., 2020 ; Cindy, 2004 ). This meta-analysis provides convergent data support for the above research views. Thus, the findings of this meta-analysis not only effectively address the first research query regarding the overall effect of cultivating critical thinking and its impact on the two dimensions of critical thinking (i.e., attitudinal tendency and cognitive skills) utilizing the approach of collaborative problem-solving, but also enhance our confidence in cultivating critical thinking by using collaborative problem-solving intervention approach in the context of classroom teaching.
Furthermore, the associated improvements in attitudinal tendency are much stronger, but the corresponding improvements in cognitive skill are only marginally better. According to certain studies, cognitive skill differs from the attitudinal tendency in classroom instruction; the cultivation and development of the former as a key ability is a process of gradual accumulation, while the latter as an attitude is affected by the context of the teaching situation (e.g., a novel and exciting teaching approach, challenging and rewarding tasks) (Halpern, 2001 ; Wei and Hong, 2022 ). Collaborative problem-solving as a teaching approach is exciting and interesting, as well as rewarding and challenging; because it takes the learners as the focus and examines problems with poor structure in real situations, and it can inspire students to fully realize their potential for problem-solving, which will significantly improve their attitudinal tendency toward solving problems (Liu et al., 2020 ). Similar to how collaborative problem-solving influences attitudinal tendency, attitudinal tendency impacts cognitive skill when attempting to solve a problem (Liu et al., 2020 ; Zhang et al., 2022 ), and stronger attitudinal tendencies are associated with improved learning achievement and cognitive ability in students (Sison, 2008 ; Zhang et al., 2022 ). It can be seen that the two specific dimensions of critical thinking as well as critical thinking as a whole are affected by collaborative problem-solving, and this study illuminates the nuanced links between cognitive skills and attitudinal tendencies with regard to these two dimensions of critical thinking. To fully develop students’ capacity for critical thinking, future empirical research should pay closer attention to cognitive skills.
The moderating effects of collaborative problem solving with regard to teaching critical thinking
In order to further explore the key factors that influence critical thinking, exploring possible moderating effects that might produce considerable heterogeneity was done using subgroup analysis. The findings show that the moderating factors, such as the teaching type, learning stage, group size, learning scaffold, duration of the intervention, measuring tool, and the subject area included in the 36 experimental designs, could all support the cultivation of collaborative problem-solving in critical thinking. Among them, the effect size differences between the learning stage and measuring tool are not significant, which does not explain why these two factors are crucial in supporting the cultivation of critical thinking utilizing the approach of collaborative problem-solving.
In terms of the learning stage, various learning stages influenced critical thinking positively without significant intergroup differences, indicating that we are unable to explain why it is crucial in fostering the growth of critical thinking.
Although high education accounts for 70.89% of all empirical studies performed by researchers, high school may be the appropriate learning stage to foster students’ critical thinking by utilizing the approach of collaborative problem-solving since it has the largest overall effect size. This phenomenon may be related to student’s cognitive development, which needs to be further studied in follow-up research.
With regard to teaching type, mixed course teaching may be the best teaching method to cultivate students’ critical thinking. Relevant studies have shown that in the actual teaching process if students are trained in thinking methods alone, the methods they learn are isolated and divorced from subject knowledge, which is not conducive to their transfer of thinking methods; therefore, if students’ thinking is trained only in subject teaching without systematic method training, it is challenging to apply to real-world circumstances (Ruggiero, 2012 ; Hu and Liu, 2015 ). Teaching critical thinking as mixed course teaching in parallel to other subject teachings can achieve the best effect on learners’ critical thinking, and explicit critical thinking instruction is more effective than less explicit critical thinking instruction (Bensley and Spero, 2014 ).
In terms of the intervention duration, with longer intervention times, the overall effect size shows an upward tendency. Thus, the intervention duration and critical thinking’s impact are positively correlated. Critical thinking, as a key competency for students in the 21st century, is difficult to get a meaningful improvement in a brief intervention duration. Instead, it could be developed over a lengthy period of time through consistent teaching and the progressive accumulation of knowledge (Halpern, 2001 ; Hu and Liu, 2015 ). Therefore, future empirical studies ought to take these restrictions into account throughout a longer period of critical thinking instruction.
With regard to group size, a group size of 2–3 persons has the highest effect size, and the comprehensive effect size decreases with increasing group size in general. This outcome is in line with some research findings; as an example, a group composed of two to four members is most appropriate for collaborative learning (Schellens and Valcke, 2006 ). However, the meta-analysis results also indicate that once the group size exceeds 7 people, small groups cannot produce better interaction and performance than large groups. This may be because the learning scaffolds of technique support, resource support, and teacher support improve the frequency and effectiveness of interaction among group members, and a collaborative group with more members may increase the diversity of views, which is helpful to cultivate critical thinking utilizing the approach of collaborative problem-solving.
With regard to the learning scaffold, the three different kinds of learning scaffolds can all enhance critical thinking. Among them, the teacher-supported learning scaffold has the largest overall effect size, demonstrating the interdependence of effective learning scaffolds and collaborative problem-solving. This outcome is in line with some research findings; as an example, a successful strategy is to encourage learners to collaborate, come up with solutions, and develop critical thinking skills by using learning scaffolds (Reiser, 2004 ; Xu et al., 2022 ); learning scaffolds can lower task complexity and unpleasant feelings while also enticing students to engage in learning activities (Wood et al., 2006 ); learning scaffolds are designed to assist students in using learning approaches more successfully to adapt the collaborative problem-solving process, and the teacher-supported learning scaffolds have the greatest influence on critical thinking in this process because they are more targeted, informative, and timely (Xu et al., 2022 ).
With respect to the measuring tool, despite the fact that standardized measurement tools (such as the WGCTA, CCTT, and CCTST) have been acknowledged as trustworthy and effective by worldwide experts, only 54.43% of the research included in this meta-analysis adopted them for assessment, and the results indicated no intergroup differences. These results suggest that not all teaching circumstances are appropriate for measuring critical thinking using standardized measurement tools. “The measuring tools for measuring thinking ability have limits in assessing learners in educational situations and should be adapted appropriately to accurately assess the changes in learners’ critical thinking.”, according to Simpson and Courtney ( 2002 , p. 91). As a result, in order to more fully and precisely gauge how learners’ critical thinking has evolved, we must properly modify standardized measuring tools based on collaborative problem-solving learning contexts.
With regard to the subject area, the comprehensive effect size of science departments (e.g., mathematics, science, medical science) is larger than that of language arts and social sciences. Some recent international education reforms have noted that critical thinking is a basic part of scientific literacy. Students with scientific literacy can prove the rationality of their judgment according to accurate evidence and reasonable standards when they face challenges or poorly structured problems (Kyndt et al., 2013 ), which makes critical thinking crucial for developing scientific understanding and applying this understanding to practical problem solving for problems related to science, technology, and society (Yore et al., 2007 ).
Suggestions for critical thinking teaching
Other than those stated in the discussion above, the following suggestions are offered for critical thinking instruction utilizing the approach of collaborative problem-solving.
First, teachers should put a special emphasis on the two core elements, which are collaboration and problem-solving, to design real problems based on collaborative situations. This meta-analysis provides evidence to support the view that collaborative problem-solving has a strong synergistic effect on promoting students’ critical thinking. Asking questions about real situations and allowing learners to take part in critical discussions on real problems during class instruction are key ways to teach critical thinking rather than simply reading speculative articles without practice (Mulnix, 2012 ). Furthermore, the improvement of students’ critical thinking is realized through cognitive conflict with other learners in the problem situation (Yang et al., 2008 ). Consequently, it is essential for teachers to put a special emphasis on the two core elements, which are collaboration and problem-solving, and design real problems and encourage students to discuss, negotiate, and argue based on collaborative problem-solving situations.
Second, teachers should design and implement mixed courses to cultivate learners’ critical thinking, utilizing the approach of collaborative problem-solving. Critical thinking can be taught through curriculum instruction (Kuncel, 2011 ; Leng and Lu, 2020 ), with the goal of cultivating learners’ critical thinking for flexible transfer and application in real problem-solving situations. This meta-analysis shows that mixed course teaching has a highly substantial impact on the cultivation and promotion of learners’ critical thinking. Therefore, teachers should design and implement mixed course teaching with real collaborative problem-solving situations in combination with the knowledge content of specific disciplines in conventional teaching, teach methods and strategies of critical thinking based on poorly structured problems to help students master critical thinking, and provide practical activities in which students can interact with each other to develop knowledge construction and critical thinking utilizing the approach of collaborative problem-solving.
Third, teachers should be more trained in critical thinking, particularly preservice teachers, and they also should be conscious of the ways in which teachers’ support for learning scaffolds can promote critical thinking. The learning scaffold supported by teachers had the greatest impact on learners’ critical thinking, in addition to being more directive, targeted, and timely (Wood et al., 2006 ). Critical thinking can only be effectively taught when teachers recognize the significance of critical thinking for students’ growth and use the proper approaches while designing instructional activities (Forawi, 2016 ). Therefore, with the intention of enabling teachers to create learning scaffolds to cultivate learners’ critical thinking utilizing the approach of collaborative problem solving, it is essential to concentrate on the teacher-supported learning scaffolds and enhance the instruction for teaching critical thinking to teachers, especially preservice teachers.
Implications and limitations
There are certain limitations in this meta-analysis, but future research can correct them. First, the search languages were restricted to English and Chinese, so it is possible that pertinent studies that were written in other languages were overlooked, resulting in an inadequate number of articles for review. Second, these data provided by the included studies are partially missing, such as whether teachers were trained in the theory and practice of critical thinking, the average age and gender of learners, and the differences in critical thinking among learners of various ages and genders. Third, as is typical for review articles, more studies were released while this meta-analysis was being done; therefore, it had a time limit. With the development of relevant research, future studies focusing on these issues are highly relevant and needed.
Conclusions
The subject of the magnitude of collaborative problem-solving’s impact on fostering students’ critical thinking, which received scant attention from other studies, was successfully addressed by this study. The question of the effectiveness of collaborative problem-solving in promoting students’ critical thinking was addressed in this study, which addressed a topic that had gotten little attention in earlier research. The following conclusions can be made:
Regarding the results obtained, collaborative problem solving is an effective teaching approach to foster learners’ critical thinking, with a significant overall effect size (ES = 0.82, z = 12.78, P < 0.01, 95% CI [0.69, 0.95]). With respect to the dimensions of critical thinking, collaborative problem-solving can significantly and effectively improve students’ attitudinal tendency, and the comprehensive effect is significant (ES = 1.17, z = 7.62, P < 0.01, 95% CI [0.87, 1.47]); nevertheless, it falls short in terms of improving students’ cognitive skills, having only an upper-middle impact (ES = 0.70, z = 11.55, P < 0.01, 95% CI [0.58, 0.82]).
As demonstrated by both the results and the discussion, there are varying degrees of beneficial effects on students’ critical thinking from all seven moderating factors, which were found across 36 studies. In this context, the teaching type (chi 2 = 7.20, P < 0.05), intervention duration (chi 2 = 12.18, P < 0.01), subject area (chi 2 = 13.36, P < 0.05), group size (chi 2 = 8.77, P < 0.05), and learning scaffold (chi 2 = 9.03, P < 0.01) all have a positive impact on critical thinking, and they can be viewed as important moderating factors that affect how critical thinking develops. Since the learning stage (chi 2 = 3.15, P = 0.21 > 0.05) and measuring tools (chi 2 = 0.08, P = 0.78 > 0.05) did not demonstrate any significant intergroup differences, we are unable to explain why these two factors are crucial in supporting the cultivation of critical thinking in the context of collaborative problem-solving.
Data availability
All data generated or analyzed during this study are included within the article and its supplementary information files, and the supplementary information files are available in the Dataverse repository: https://doi.org/10.7910/DVN/IPFJO6 .
Bensley DA, Spero RA (2014) Improving critical thinking skills and meta-cognitive monitoring through direct infusion. Think Skills Creat 12:55–68. https://doi.org/10.1016/j.tsc.2014.02.001
Article Google Scholar
Castle A (2009) Defining and assessing critical thinking skills for student radiographers. Radiography 15(1):70–76. https://doi.org/10.1016/j.radi.2007.10.007
Chen XD (2013) An empirical study on the influence of PBL teaching model on critical thinking ability of non-English majors. J PLA Foreign Lang College 36 (04):68–72
Google Scholar
Cohen A (1992) Antecedents of organizational commitment across occupational groups: a meta-analysis. J Organ Behav. https://doi.org/10.1002/job.4030130602
Cooper H (2010) Research synthesis and meta-analysis: a step-by-step approach, 4th edn. Sage, London, England
Cindy HS (2004) Problem-based learning: what and how do students learn? Educ Psychol Rev 51(1):31–39
Duch BJ, Gron SD, Allen DE (2001) The power of problem-based learning: a practical “how to” for teaching undergraduate courses in any discipline. Stylus Educ Sci 2:190–198
Ennis RH (1989) Critical thinking and subject specificity: clarification and needed research. Educ Res 18(3):4–10. https://doi.org/10.3102/0013189x018003004
Facione PA (1990) Critical thinking: a statement of expert consensus for purposes of educational assessment and instruction. Research findings and recommendations. Eric document reproduction service. https://eric.ed.gov/?id=ed315423
Facione PA, Facione NC (1992) The California Critical Thinking Dispositions Inventory (CCTDI) and the CCTDI test manual. California Academic Press, Millbrae, CA
Forawi SA (2016) Standard-based science education and critical thinking. Think Skills Creat 20:52–62. https://doi.org/10.1016/j.tsc.2016.02.005
Halpern DF (2001) Assessing the effectiveness of critical thinking instruction. J Gen Educ 50(4):270–286. https://doi.org/10.2307/27797889
Hu WP, Liu J (2015) Cultivation of pupils’ thinking ability: a five-year follow-up study. Psychol Behav Res 13(05):648–654. https://doi.org/10.3969/j.issn.1672-0628.2015.05.010
Huber K (2016) Does college teach critical thinking? A meta-analysis. Rev Educ Res 86(2):431–468. https://doi.org/10.3102/0034654315605917
Kek MYCA, Huijser H (2011) The power of problem-based learning in developing critical thinking skills: preparing students for tomorrow’s digital futures in today’s classrooms. High Educ Res Dev 30(3):329–341. https://doi.org/10.1080/07294360.2010.501074
Kuncel NR (2011) Measurement and meaning of critical thinking (Research report for the NRC 21st Century Skills Workshop). National Research Council, Washington, DC
Kyndt E, Raes E, Lismont B, Timmers F, Cascallar E, Dochy F (2013) A meta-analysis of the effects of face-to-face cooperative learning. Do recent studies falsify or verify earlier findings? Educ Res Rev 10(2):133–149. https://doi.org/10.1016/j.edurev.2013.02.002
Leng J, Lu XX (2020) Is critical thinking really teachable?—A meta-analysis based on 79 experimental or quasi experimental studies. Open Educ Res 26(06):110–118. https://doi.org/10.13966/j.cnki.kfjyyj.2020.06.011
Liang YZ, Zhu K, Zhao CL (2017) An empirical study on the depth of interaction promoted by collaborative problem solving learning activities. J E-educ Res 38(10):87–92. https://doi.org/10.13811/j.cnki.eer.2017.10.014
Lipsey M, Wilson D (2001) Practical meta-analysis. International Educational and Professional, London, pp. 92–160
Liu Z, Wu W, Jiang Q (2020) A study on the influence of problem based learning on college students’ critical thinking-based on a meta-analysis of 31 studies. Explor High Educ 03:43–49
Morris SB (2008) Estimating effect sizes from pretest-posttest-control group designs. Organ Res Methods 11(2):364–386. https://doi.org/10.1177/1094428106291059
Article ADS Google Scholar
Mulnix JW (2012) Thinking critically about critical thinking. Educ Philos Theory 44(5):464–479. https://doi.org/10.1111/j.1469-5812.2010.00673.x
Naber J, Wyatt TH (2014) The effect of reflective writing interventions on the critical thinking skills and dispositions of baccalaureate nursing students. Nurse Educ Today 34(1):67–72. https://doi.org/10.1016/j.nedt.2013.04.002
National Research Council (2012) Education for life and work: developing transferable knowledge and skills in the 21st century. The National Academies Press, Washington, DC
Niu L, Behar HLS, Garvan CW (2013) Do instructional interventions influence college students’ critical thinking skills? A meta-analysis. Educ Res Rev 9(12):114–128. https://doi.org/10.1016/j.edurev.2012.12.002
Peng ZM, Deng L (2017) Towards the core of education reform: cultivating critical thinking skills as the core of skills in the 21st century. Res Educ Dev 24:57–63. https://doi.org/10.14121/j.cnki.1008-3855.2017.24.011
Reiser BJ (2004) Scaffolding complex learning: the mechanisms of structuring and problematizing student work. J Learn Sci 13(3):273–304. https://doi.org/10.1207/s15327809jls1303_2
Ruggiero VR (2012) The art of thinking: a guide to critical and creative thought, 4th edn. Harper Collins College Publishers, New York
Schellens T, Valcke M (2006) Fostering knowledge construction in university students through asynchronous discussion groups. Comput Educ 46(4):349–370. https://doi.org/10.1016/j.compedu.2004.07.010
Sendag S, Odabasi HF (2009) Effects of an online problem based learning course on content knowledge acquisition and critical thinking skills. Comput Educ 53(1):132–141. https://doi.org/10.1016/j.compedu.2009.01.008
Sison R (2008) Investigating Pair Programming in a Software Engineering Course in an Asian Setting. 2008 15th Asia-Pacific Software Engineering Conference, pp. 325–331. https://doi.org/10.1109/APSEC.2008.61
Simpson E, Courtney M (2002) Critical thinking in nursing education: literature review. Mary Courtney 8(2):89–98
Stewart L, Tierney J, Burdett S (2006) Do systematic reviews based on individual patient data offer a means of circumventing biases associated with trial publications? Publication bias in meta-analysis. John Wiley and Sons Inc, New York, pp. 261–286
Tiwari A, Lai P, So M, Yuen K (2010) A comparison of the effects of problem-based learning and lecturing on the development of students’ critical thinking. Med Educ 40(6):547–554. https://doi.org/10.1111/j.1365-2929.2006.02481.x
Wood D, Bruner JS, Ross G (2006) The role of tutoring in problem solving. J Child Psychol Psychiatry 17(2):89–100. https://doi.org/10.1111/j.1469-7610.1976.tb00381.x
Wei T, Hong S (2022) The meaning and realization of teachable critical thinking. Educ Theory Practice 10:51–57
Xu EW, Wang W, Wang QX (2022) A meta-analysis of the effectiveness of programming teaching in promoting K-12 students’ computational thinking. Educ Inf Technol. https://doi.org/10.1007/s10639-022-11445-2
Yang YC, Newby T, Bill R (2008) Facilitating interactions through structured web-based bulletin boards: a quasi-experimental study on promoting learners’ critical thinking skills. Comput Educ 50(4):1572–1585. https://doi.org/10.1016/j.compedu.2007.04.006
Yore LD, Pimm D, Tuan HL (2007) The literacy component of mathematical and scientific literacy. Int J Sci Math Educ 5(4):559–589. https://doi.org/10.1007/s10763-007-9089-4
Zhang T, Zhang S, Gao QQ, Wang JH (2022) Research on the development of learners’ critical thinking in online peer review. Audio Visual Educ Res 6:53–60. https://doi.org/10.13811/j.cnki.eer.2022.06.08
Download references
Acknowledgements
This research was supported by the graduate scientific research and innovation project of Xinjiang Uygur Autonomous Region named “Research on in-depth learning of high school information technology courses for the cultivation of computing thinking” (No. XJ2022G190) and the independent innovation fund project for doctoral students of the College of Educational Science of Xinjiang Normal University named “Research on project-based teaching of high school information technology courses from the perspective of discipline core literacy” (No. XJNUJKYA2003).
Author information
Authors and affiliations.
College of Educational Science, Xinjiang Normal University, 830017, Urumqi, Xinjiang, China
Enwei Xu, Wei Wang & Qingxia Wang
You can also search for this author in PubMed Google Scholar
Corresponding authors
Correspondence to Enwei Xu or Wei Wang .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors.
Informed consent
Additional information.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary tables, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Xu, E., Wang, W. & Wang, Q. The effectiveness of collaborative problem solving in promoting students’ critical thinking: A meta-analysis based on empirical literature. Humanit Soc Sci Commun 10 , 16 (2023). https://doi.org/10.1057/s41599-023-01508-1
Download citation
Received : 07 August 2022
Accepted : 04 January 2023
Published : 11 January 2023
DOI : https://doi.org/10.1057/s41599-023-01508-1
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
This article is cited by
Impacts of online collaborative learning on students’ intercultural communication apprehension and intercultural communicative competence.
- Hoa Thi Hoang Chau
- Hung Phu Bui
- Quynh Thi Huong Dinh
Education and Information Technologies (2024)
Exploring the effects of digital technology on deep learning: a meta-analysis
Sustainable electricity generation and farm-grid utilization from photovoltaic aquaculture: a bibliometric analysis.
- A. A. Amusa
- M. Alhassan
International Journal of Environmental Science and Technology (2024)
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies

- lol Badge Feed
- win Badge Feed
- trending Badge Feed
Browse links
- © 2024 BuzzFeed, Inc
- Consent Preferences
- Accessibility Statement
Beauty + Personal Care
Sports + Fitness
We hope you love our recommendations! Some may have been sent as samples, but all were independently selected by our editors. Just FYI, BuzzFeed and its publishing partners may collect a share of sales and/or other compensation from the links on this page.
26 Products That Deserve An Award For All The Problems They'll Solve In 2022
Maybe in 2022, the CDC will print wallet-sized vaccine cards but until that happens, keeps yours safe with a cute vax card holder.

BuzzFeed Staff
1. Dishwasher cleaning tablets so the machine you rely on to clean the things you use to eat isn't gunking them up even more.

These tablets remove odor-causing residue and help get rid of lime and mineral build-up that naturally occurs inside dishwashers. The tablet is designed to last throughout the entire wash cycle, and is recommended for use about once a month. These are safe to use in stainless-steel tub and plastic tub dishwashers.
Promising review: "After using this product, I am happy to report that my $5 investment saved me over $500. I was ready to replace my dishwasher due to super cloudy glasses, residue, and just not getting clean. Then, I became aware that the water softener no longer was doing its job, so I had the rental company replace it. Dishwasher performance improved somewhat. I decided to do two more loads before deciding to purchase a new one. Then I saw a product test review for Affresh in a magazine. I was ordering some stuff from Amazon anyway, so I added that to my order. When it came, I tossed one of the tablets into the bottom of the full machine, and ran the regular cycle. I did not expect the results I got! My glassware that I thought was permanently etched and ruined came out like new. Same with cutlery. The difference is unbelievable. I will use this faithfully on a monthly basis, as recommended. I can even put it on my subscribe and save order, so I will get a new pack every six months. I am amazed!" — Sheila
Get a pack of six from Amazon for $5.99 .
2. And while you're at it, you'll want to add this pack of washing machine cleaning tablets to your cart as well!

These are safe to use with front-load washing machines and top-load washing machines, and both high efficiency and conventional machines. Recommended to use once a month!
Promising review: "I have been using bleach to clean my machine for some time, but decided to give this a try a few months ago. My very first clean with Affresh left me surprised and delighted, for not only did it clean my machine, it eliminated the nasty smell that always transferred to my clothes thanks to a build-up of mold I didn't even know about. Every month now, I toss a tablet into the drum and let it work its magic. Now, my machine is cleaner than ever, and my clothes always smell wonderfully fresh. I highly recommend this to everyone." — Kelli Crawford
Get a pack of six from Amazon for $10.79 .
3. A pet hair roller because everything about our little friends is absolutely perfect except for the fact that their fur and hair get on everything we own. But we still love them, right?

Promising review: "Where has this been all my cat-loving life? Sticky rollers work fine for clothes, but this is the only product that has ever COMPLETELY removed all the cat hair from my bed. I have a long-haired, 20-pound tabby, and if you run your hands up his back a few times and fling the hair everywhere, it looks like it's snowing — he never stops shedding no matter what I do. After using the ChomChom, I can put on a black dress and roll around on my bed and not get a single hair on me. It's absolutely amazing. Everyone is getting one for Christmas, even if they don't have a pet. I don't care; it's THAT good." — Stephanie
Get it from Amazon for $24.95 .
4. Water bottle cleaning tablets for getting your beloved drinking bottle back to the condition it was in when you first fell in love with it. Not to mention the fact that you should only ever consume water from a CLEAN bottle.

Tablets are biodegradable, chlorine-free, all-natural, and environmentally safe. They're individually packaged, and don't require any additional brushing or scrubbing. Good for use on stainless-steel bottles, mugs, hydration reservoirs, coolers, dishes, and hard-to-clean plastic containers and bottles.
Promising review: "In all fairness, I first heard of this product while watching Shark Tank, and their pitch was impressive so I gave the underdog a try. Now, I'm on my fourth re-order. My whole family drinks out of various name brand bottles, coffee mugs, etc. The fact is, they are rarely cleaned because they are a part of our daily lives and they are a pain in the ar$e to clean, because of the inconvenience that they are not dishwasher-safe, or don't fit. The answer is these tablets. They work and they're simple to use." — K.R.
Get them from Amazon for $8/12 tablets .
5. A touch-up paint pen to fill with your paint color of choice and apply to any imperfections you're trying to cover up.

Promising review: "Love this — absolutely perfect for touchin' up little spots that need touchin' up. I have several sets filled with different paints and so far they've stayed usable, without the paint drying out. I rinse the brush really well after each use (latex paints) and recap it. It would be nice if the manufacturer put an area on the pen where you could easily label the paint info, but I use a permanent marker, and it works okay." — Hooked on Amazon!
Get a pack of two from Amazon for $17.99 .
6. And this little bottle of paint touch-up so you can quickly fix chips, cracks, and stains on your walls without having to re-do the whole thing.

This paint is nontoxic, zero VOC, low-odor, and solvent-free, so if you're sensitive to chemical smells, this stuff is A-OK!! What makes this different than the one above? Great question! This bottle is already filled with paint so if it's a neutral color you're trying to cover up or you simply don't have the original jar of paint (or remember what the shade was called), this is great. Whereas the pen above is ideal for more specific paint colors and those who still have easy access to the paint color they need.
Promising review: "This product is excellent. It goes on easily and covers paint scraps very well. I used it on a door frame that had been chipped. Now the chip is practically unnoticeable. I asked for a sample of colors before buying and received a color chart promptly. I appreciate the customer-friendly attitude of this company." — Educator
Get it from Amazon for $14.95 (available in eight shades).
7. A bug bite suction tool to help get rid of itchy bites. Kinda rude that little buggies get to munch on our skin and blood, and we have to deal with itchiness after.

This works by suctioning up insect venom, saliva, and other irritants under the skin, which in turn prevents your body from producing a reaction to said irritant.
Promising review: "I am a magnet for bites of all kinds and carry topical and medicines with me at all times — so I figured this would be a good product to see if it really works. It arrived on Monday and on Tuesday morning I woke up with a bug bite on my arm. I used this little tool (3x per the instructions) and documented with photos. Immediately after using, it stopped itching! And less than 24 hours later the bump/bite was gone! There is a very faint red mark from using the thing but a small price to pay IMO. Bottom line: it’s awesome. I’m carrying it with me everywhere!" — Rebecca
Get it from Amazon for $9.95 (available in three colors).
8. A eucalyptus and lavender shower/bath pouch that'll help give you a spa experience right from the comfort of home. These may also help provide some relief from colds, congestions, and stress.

Eucalyptus Blooms is an Etsy shop based in Charlotte, North Carolina that sells eucalyptus and lavender shower and bath products and bouquets.
Promising review: "Not only does these enhance my shower experience, but my whole bathroom smells nice all the time!" — Edward
Get it from Eucalyptus Blooms on Etsy for $13.59/three pouches or $17.84/five pouches .
9. A dental health powder you simply sprinkle onto your pup's food as if you're a magical fairy giving them the mystical gift of clean teeth and fresh breath.

Promising review: "I began to use this product on my Doberman at about 1 year. He is now 4 years old, and the vet says his teeth and gums are amazing. I have never done any dental work with him and do not brush his teeth. He has fresh breath and no tooth decay or gum issues. I absolutely credit Perio Support for his healthy mouth and will always use it on my dogs." — HappytoGrill
Get it from Amazon for $20 .
10. Soundproof door strips for those whose bedroom currently doubles as a home office, and their new "co-workers" (aka roomies, family members, and pets) are kinda noisy. These also help prevent cold air escape in the summer, and warmth escape in the winter, so you can save energy, too!

Promising review: "Product works really well! I needed a quick fix to my home office situation. I live in an apartment in Manhattan and never noticed how much sound comes in and out, until I had to be on conference calls working from home! This little tape made a big difference, took me a couple of minutes to install." — Sandra Revueltas
Get a pack of two from Amazon for $7.97+ (available in four colors).
11. A FlexiSnake so you can unclog your hair-filled drain by simply ~snaking~ this tool down there, letting it grab the hair, pulling it back up, and deciding whether you should be marveled at its abilities or gag.

More than 4,000 hook and loop micro-hooks cover the full 18-inch span of the snake. It's reusable! Just remove hair after use, and clean with soap, water, and a brush. It's compatible with most bathroom drains, without needing to take off the stopper.
Promising review: "I didn’t expect this to be professional grade or anything, but hey, for the price, this definitely did the job. Our bathroom sink was starting to drain really slowly, so I bought this. In less than two minutes, it had fed down the drain easily and pulled up two separate disgusting chunks of hair and soap scum. I wore cleaning gloves to clean that gunk off the snake, but it wasn’t too difficult. Drain worked perfectly after. I use it maybe once a month to maintain. Good value!" — KB
Get it from Amazon for $8.99 .
12. Or a TubShroom that'll collect your hair while in the shower/bath, so it doesn't go down the drain and clog in the first place.

This fits any standard 1.5 inch tub drain or bathroom sink drain. But, if you want to keep your hair catching separate between your tub and sink, then treat yourself and your home to the SinkShroom !
Promising review: "This is absolutely worth every penny. Kudos to the inventor of this product. I have thick long dark hair, and after two months of moving into my own apartment, my shower drain was completely clogged with all my hair. After being disgusted at the amount of hair I had to clean out with a snake (which is NOT a fun task), I decided I needed to purchase something to prevent it from happening again. I read about this product on a BuzzFeed article, and I have no regrets. It is so satisfying to clean out, and it does not lie when it says it catches every single hair. I have had it for close to 4 months without once instance of my shower drain backing up. This product is absolutely worth it." — JT
Get it from Amazon for $12.95+ (available in five colors).
13. A car vent face mask holder to provide a more organized, cleaner space in your vehicle to keep masks. Whether it's a mask you're already wearing while running errands, or just keeping some extra masks on-hand, this baby will be super useful.

ArchersDesignShop is a small business based in Indianapolis, IN that sells 3D printed goods for your car so that belongings like face masks and sunglasses are in a tidy area, rather than strewn on the seats, floors, or worse... in hard-to-reach areas.
Get it from ArchersDesignShop on Etsy for $4.50 (available in four colors).
14. Acne patches you can apply to areas where you're breaking out. Let it sit overnight or throughout the day, peel it off, and watch it take all the pore-clogging gunk with it.

These patches contain hydrocolloid dressing with a hint of tea tree oil, calendula oil, and cica. The ingredients in this are gentle, ideal for all skin types and tones!
Promising review: "I can't believe how much money I've spent on acne products over the years before I found this. Of all the products with glowing reviews, these patches have been the most effective and worth their cost. I have sensitive combo skin and deal with adult acne on a daily basis. Since my face has dry areas, I'm also more likely to pick at it (TMI, sorry). It's terribly embarrassing to go to work with these kinds of issues day after day, so in addition to taking a prescription, I've been on the hunt for anything topical that would help. The first time I used one of these patches, I put it on at night. The next morning, I woke up and was kind of shocked. It actually did what it was supposed to do. You peel off the patch, and with it comes at least 90% of the nastiness that was clogging your skin. It DRASTICALLY reduces the size of the zit. I've also experimented with using these on cystic acne, and they work wonders for speeding up the clearing and healing process. Also, they're comfortable to wear and stay on your face pretty well overnight!" — Greta H
Get a pack of 40 from Amazon for $8.49 .
15. Window screen repair tape that'll only takes about 30 seconds to apply, is super strong and durable, and will be a heck of a lot cheaper than having to replace an entire screen.

Promising review: "Holy cow! This stuff WORKS! I had been using regular packing tape to patch up my screen door that was riddled with holes and tears, but those mosquitoes were making their way in, and it looked terrible. I picked up a roll of this just to check it out, and man, the repair is practically like I installed a new screen! I thought it was going to be tape with the net pattern printed on it, but IT'S REAL NETTING with adhesive on one side, so it really is a solid repair! Highly recommend!" — SteveBFX
Get it from Amazon for $9.99+ (available in two colors).
16. A vaccine card holder to keep that very important little card safe and secure on the go. You may need to keep it handy when dining out, attending shows, or traveling. Since it's slightly too big to keep in your wallet, why not ensure it stays extra safe?

FamiliarPaws is an Etsy shop that sells personalized pet supplies and leather accessories.
Get it from FamiliarPaws on Etsy for $12.99+ (available in eight colors and with or without personalization).
17. Or spice things up with the Stitch (AKA Experiment 626) one on the left or the Hamilton one on the right.

DeBoop Shop is based in Lexington-Fayette, Kentucky that sells coasters, embroidered keychains, face masks, and more. SnarkandFandoms is based in Pennsylvania and sells pet toys, key tags, ornaments, and more.
Get them from Etsy: the Stitch (Experiment 626) card holder on the left from DeBoop Shop for $15 and the Hamilton "I'm not throwin' away my shot" card holder on the right from SnarkandFandoms for $20 (available in four colors and three styles).
18. A quick-dry top coat because the worst part of painting your nails is shaving time off your precious day to wait for them to dry. On average, this stuff will help your nails dry in about 10 minutes!

I am the (or at least used to be) the queen of smudging my nails immediately after drying them. I'd sit at the salon or in my house for about 20 minutes allowing my nails to dry just to learn the hard way that 20 minutes wasn't long enough. I can't help that I'm an impatient person! I learned about this amazing top coat about two years ago and it's a true game-changer — I even bring it to the salon with me to cut down on drying time, that's how much I love it! It really does get your nails dry in about 10 minutes (even less if you use an express dry nail polish like the new Expressie quick-dry nail polish from Essie, which I also love). Less time drying my nails and less smudging = happy me.
Get it from CVS for $11.99 .
19. A Snuggle Puppy that's basically a miracle solution to helping ease your pup's loneliness and separation anxiety — it's especially perfect for those crate-training their furry bbs.

Last year my family made the wonderful decision to get an adorable Havanese puppy named Bailey (pictured left). Bailey experienced some major separation anxiety in those first few days/nights and we knew for the sake of our sanity and sleep schedule that we had to find a solution. Enter: The Snuggle Puppy.
It comes with a little red heartbeat ticker and heat packs (we actually didn't even use the heat packs), that you simply place into the middle of the dog, velcro it shut, and it's heartbeat helps to make your puppy feel less alone and simulate the feeling of cuddling up to their mom. I swear this thing must be made with pixie dust because within an hour of putting this in his crate, Bailey stopped crying and was fast asleep next to it. If you opt to get the kit (we did), it also comes with two toys and a fleece blanket.
Bailey is a little over a year old now so he doesn't use the puppy for comfort like he did those first few weeks, but it's STILL his favorite toy. Seriously, he loves it so much that he is constantly attempting to see if he can pick it up and bring it with him outside when we go on walks. We got him another one for his birthday and he loves it just as much as he loves the first one. It's on the pricy side for a plush dog toy, but considering how much it helped save our sanity and how much Bailey still adores it, it's a million percent worth it. This is always at the top of the list of my recommendations for friends bringing home puppies because it's just that good.
Get it from Amazon: the Snuggle Puppy for $26.98+ (available in five colors), and the Snuggle Puppy kit for $55.96 .
20. A pack of furniture touch-up sticks to quickly restore wooden furniture back to the condition it was in when you first decided to buy it. If these touch-up pens would've existed when you were a kid, perhaps your parents would've actually thanked you for drawing on the furniture.

Includes six repair markets, six paper-wrapped wax sticks, and one wax stick sharpener packaged in a blister card. Plus, it comes with six different colors — maple, oak, cherry, walnut, mahogany, and black. To use, just draw over a scratch/scuff/discoloration on your wooden furniture, allow it to dry quickly, and bam! It's magic.
Promising review: "Better than expected. Blends perfectly and leaves a beautiful sheen. Used them on different shades of wood cherry, oak, and mahogany. I blended several shades of markers on each piece. Blended easily and matched perfectly to the different shades of woods. Used on claw foot dining table, chippendale chair legs, Grandfather clock, china cabinet. All look sensational. Covered sweeper scuffs well. They look new now, not touched up. These stain quickly, so wear disposable gloves and cover floors where you are working. Excellent results." — PhoebeS
Get a pack of 13 from Amazon for $9.99 .
21. A measurement conversion decal so you can refer to this handy cheat sheet while cooking and baking instead of having to constantly rely on a Google search.

LatigoLace is a small business that sells these super helpful, aesthetically-pleasing kitchen measurement decals to seriously help simplify the task of figuring out the right conversions.
Promising review: "I am so happy with this purchase! It was one of the things on my list of things to better organize my kitchen! Great quality and just what I had hoped for!" — Ann Riley
Get it from LatigoLace on Etsy for $13+ (available in four sizes, and two colors).
22. An antiseptic spray to help treat infections your fluffy friend might get, such as yeast infections, hot spots, ringworm, and pyoderma.

Promising review: "Do your dogs smell like bread dough? Or Fritos? Do their ears smell REALLY bad? Do they lick their paws often? Do they bite their legs, back, hips, or hind end? Do they lick their bellies often? Have you noticed small, scablike spots in their undercarriage? Brown spots on their skin? Red skin? Or the ultimate — a darkening of the skin that rubs off? If so, then your dogs probably have a yeast problem, which you might not ever have heard of, but this spray will provide instant relief! Most doctors first diagnose yeast problems simply by smell, so save yourself the vet bill and try this first! You can't get rid of it just by giving them a bath — you need a medicated shampoo or spray like this in order to effectively manage the yeast, and you have to use it for at least three months. I know it seems like a long time, but trust me, I learned the hard way. Yes, veterinarians can also diagnose by scraping skin cells and looking at them under a microscope, but generally they will diagnose a yeast infection in dogs simply by smelling them. Most pet owners never even know that dogs can get yeast infections. I didn't know, and I've had dogs for at least 15 years. This spray is the same strength you would get from a veterinarian's office, but without the cost of that bill. I highly, highly, highly recommend this spray for treating yeast and fungal infections in dogs. I'll try to update with more symptoms and photos as I can and as I think of them. I didn't take a lot of photos when I started treating the dogs and when they started having problems, but I'm always happy to help other pet owners navigate this horrible, horrible affliction. If you have any questions, feel free to ask — I'd rather help others so they can get their pets treated right the first time and for a fraction of the cost of going to the vet." — Amazoncustomer
Get it from Amazon for $12.99+ (available in two sizes).
23. The Spatty — a two-piece set of flexible, tiny spatulas that'll ensure the little bits of makeup or food remnants in the hard-to-reach crevices of the jar won't go to waste.

These are FDA- and USDA-approved, and BPA-free, and can fit into virtually any bottle. Plus, they're made of sturdy, resilient, and flexible material, and they're dishwasher-safe! Check out our review of The Spatty (#1)!
Promising review: "So worth it! I'm so happy with it. You will definitely save money using this. I think about how much I could have saved if this was invented 30 years ago. I mostly use it for small makeup jars. I tested out the longer one on a 18 oz. lotion and it worked fine. Some reviews complain about not being able to get every curve and corner of their container... oh please! You get so much more than you would without it." — Liz
Get a set of two from Amazon for $11.99 .
24. Debrox earwax removal drops to give your ears the clean they not only want, but truly need — think of how much clearer listening to Red (Taylor's Version) on repeat all day will sound now. Pure bliss.

This cleaner uses micro-foam action to safely soften and remove earwax in a nonirritating manner.
Promising review: "My right ear was totally plugged so I went to the pharmacy and the pharmacist said that this is the one doctors usually tell patients to get. I put the drops in, waited, then flushed my ear out with very warm water and OH MY GOSH... the gunk that came flowing out onto the towel blew my mind! It's amazing that I was ever able to hear at all with all that crap in my ear. This stuff works." — CD
Get it from Amazon for $5.98 .
25. A jewelry cleaning pen so you can give your precious gems a quick swipe of a pen to get them looking brand new.

Promising review: "I was so excited to see the huge difference in how clean my jewelry looked. The cleaning process took less than five minutes and now it sparkles like new!" — Jackie_X
Get it from Amazon for $7.51 .
26. BluApple produce fresheners to help extend the life of your precious fruits and veggies two to three times longer. All you need to do is toss 'em into the produce drawer in the fridge and let them work their magic.

Promising review: "I'm so happy with my purchase because these keep my produce fresher for much longer than normal. Nothing is worse than buying red bell peppers at the store and having them start wilting after four days. These should be in everyone's fridges!" — The Waites
Get a pack of two from Amazon for $11.99 .
Looking for the perfect gift for any occasion? Check out all of BuzzFeed’s gift guides !

Reviews have been edited for length and/or clarity.
Share This Article
- Business Essentials
- Leadership & Management
- Credential of Leadership, Impact, and Management in Business (CLIMB)
- Entrepreneurship & Innovation
- Digital Transformation
- Finance & Accounting
- Business in Society
- For Organizations
- Support Portal
- Media Coverage
- Founding Donors
- Leadership Team

- Harvard Business School →
- HBS Online →
- Business Insights →
Business Insights
Harvard Business School Online's Business Insights Blog provides the career insights you need to achieve your goals and gain confidence in your business skills.
- Career Development
- Communication
- Decision-Making
- Earning Your MBA
- Negotiation
- News & Events
- Productivity
- Staff Spotlight
- Student Profiles
- Work-Life Balance
- AI Essentials for Business
- Alternative Investments
- Business Analytics
- Business Strategy
- Business and Climate Change
- Design Thinking and Innovation
- Digital Marketing Strategy
- Disruptive Strategy
- Economics for Managers
- Entrepreneurship Essentials
- Financial Accounting
- Global Business
- Launching Tech Ventures
- Leadership Principles
- Leadership, Ethics, and Corporate Accountability
- Leading Change and Organizational Renewal
- Leading with Finance
- Management Essentials
- Negotiation Mastery
- Organizational Leadership
- Power and Influence for Positive Impact
- Strategy Execution
- Sustainable Business Strategy
- Sustainable Investing
- Winning with Digital Platforms
What Is Creative Problem-Solving & Why Is It Important?

- 01 Feb 2022
One of the biggest hindrances to innovation is complacency—it can be more comfortable to do what you know than venture into the unknown. Business leaders can overcome this barrier by mobilizing creative team members and providing space to innovate.
There are several tools you can use to encourage creativity in the workplace. Creative problem-solving is one of them, which facilitates the development of innovative solutions to difficult problems.
Here’s an overview of creative problem-solving and why it’s important in business.
Access your free e-book today.
What Is Creative Problem-Solving?
Research is necessary when solving a problem. But there are situations where a problem’s specific cause is difficult to pinpoint. This can occur when there’s not enough time to narrow down the problem’s source or there are differing opinions about its root cause.
In such cases, you can use creative problem-solving , which allows you to explore potential solutions regardless of whether a problem has been defined.
Creative problem-solving is less structured than other innovation processes and encourages exploring open-ended solutions. It also focuses on developing new perspectives and fostering creativity in the workplace . Its benefits include:
- Finding creative solutions to complex problems : User research can insufficiently illustrate a situation’s complexity. While other innovation processes rely on this information, creative problem-solving can yield solutions without it.
- Adapting to change : Business is constantly changing, and business leaders need to adapt. Creative problem-solving helps overcome unforeseen challenges and find solutions to unconventional problems.
- Fueling innovation and growth : In addition to solutions, creative problem-solving can spark innovative ideas that drive company growth. These ideas can lead to new product lines, services, or a modified operations structure that improves efficiency.

Creative problem-solving is traditionally based on the following key principles :
1. Balance Divergent and Convergent Thinking
Creative problem-solving uses two primary tools to find solutions: divergence and convergence. Divergence generates ideas in response to a problem, while convergence narrows them down to a shortlist. It balances these two practices and turns ideas into concrete solutions.
2. Reframe Problems as Questions
By framing problems as questions, you shift from focusing on obstacles to solutions. This provides the freedom to brainstorm potential ideas.
3. Defer Judgment of Ideas
When brainstorming, it can be natural to reject or accept ideas right away. Yet, immediate judgments interfere with the idea generation process. Even ideas that seem implausible can turn into outstanding innovations upon further exploration and development.
4. Focus on "Yes, And" Instead of "No, But"
Using negative words like "no" discourages creative thinking. Instead, use positive language to build and maintain an environment that fosters the development of creative and innovative ideas.
Creative Problem-Solving and Design Thinking
Whereas creative problem-solving facilitates developing innovative ideas through a less structured workflow, design thinking takes a far more organized approach.
Design thinking is a human-centered, solutions-based process that fosters the ideation and development of solutions. In the online course Design Thinking and Innovation , Harvard Business School Dean Srikant Datar leverages a four-phase framework to explain design thinking.
The four stages are:

- Clarify: The clarification stage allows you to empathize with the user and identify problems. Observations and insights are informed by thorough research. Findings are then reframed as problem statements or questions.
- Ideate: Ideation is the process of coming up with innovative ideas. The divergence of ideas involved with creative problem-solving is a major focus.
- Develop: In the development stage, ideas evolve into experiments and tests. Ideas converge and are explored through prototyping and open critique.
- Implement: Implementation involves continuing to test and experiment to refine the solution and encourage its adoption.
Creative problem-solving primarily operates in the ideate phase of design thinking but can be applied to others. This is because design thinking is an iterative process that moves between the stages as ideas are generated and pursued. This is normal and encouraged, as innovation requires exploring multiple ideas.
Creative Problem-Solving Tools
While there are many useful tools in the creative problem-solving process, here are three you should know:
Creating a Problem Story
One way to innovate is by creating a story about a problem to understand how it affects users and what solutions best fit their needs. Here are the steps you need to take to use this tool properly.
1. Identify a UDP
Create a problem story to identify the undesired phenomena (UDP). For example, consider a company that produces printers that overheat. In this case, the UDP is "our printers overheat."
2. Move Forward in Time
To move forward in time, ask: “Why is this a problem?” For example, minor damage could be one result of the machines overheating. In more extreme cases, printers may catch fire. Don't be afraid to create multiple problem stories if you think of more than one UDP.
3. Move Backward in Time
To move backward in time, ask: “What caused this UDP?” If you can't identify the root problem, think about what typically causes the UDP to occur. For the overheating printers, overuse could be a cause.
Following the three-step framework above helps illustrate a clear problem story:
- The printer is overused.
- The printer overheats.
- The printer breaks down.
You can extend the problem story in either direction if you think of additional cause-and-effect relationships.
4. Break the Chains
By this point, you’ll have multiple UDP storylines. Take two that are similar and focus on breaking the chains connecting them. This can be accomplished through inversion or neutralization.
- Inversion: Inversion changes the relationship between two UDPs so the cause is the same but the effect is the opposite. For example, if the UDP is "the more X happens, the more likely Y is to happen," inversion changes the equation to "the more X happens, the less likely Y is to happen." Using the printer example, inversion would consider: "What if the more a printer is used, the less likely it’s going to overheat?" Innovation requires an open mind. Just because a solution initially seems unlikely doesn't mean it can't be pursued further or spark additional ideas.
- Neutralization: Neutralization completely eliminates the cause-and-effect relationship between X and Y. This changes the above equation to "the more or less X happens has no effect on Y." In the case of the printers, neutralization would rephrase the relationship to "the more or less a printer is used has no effect on whether it overheats."
Even if creating a problem story doesn't provide a solution, it can offer useful context to users’ problems and additional ideas to be explored. Given that divergence is one of the fundamental practices of creative problem-solving, it’s a good idea to incorporate it into each tool you use.
Brainstorming
Brainstorming is a tool that can be highly effective when guided by the iterative qualities of the design thinking process. It involves openly discussing and debating ideas and topics in a group setting. This facilitates idea generation and exploration as different team members consider the same concept from multiple perspectives.
Hosting brainstorming sessions can result in problems, such as groupthink or social loafing. To combat this, leverage a three-step brainstorming method involving divergence and convergence :
- Have each group member come up with as many ideas as possible and write them down to ensure the brainstorming session is productive.
- Continue the divergence of ideas by collectively sharing and exploring each idea as a group. The goal is to create a setting where new ideas are inspired by open discussion.
- Begin the convergence of ideas by narrowing them down to a few explorable options. There’s no "right number of ideas." Don't be afraid to consider exploring all of them, as long as you have the resources to do so.
Alternate Worlds
The alternate worlds tool is an empathetic approach to creative problem-solving. It encourages you to consider how someone in another world would approach your situation.
For example, if you’re concerned that the printers you produce overheat and catch fire, consider how a different industry would approach the problem. How would an automotive expert solve it? How would a firefighter?
Be creative as you consider and research alternate worlds. The purpose is not to nail down a solution right away but to continue the ideation process through diverging and exploring ideas.

Continue Developing Your Skills
Whether you’re an entrepreneur, marketer, or business leader, learning the ropes of design thinking can be an effective way to build your skills and foster creativity and innovation in any setting.
If you're ready to develop your design thinking and creative problem-solving skills, explore Design Thinking and Innovation , one of our online entrepreneurship and innovation courses. If you aren't sure which course is the right fit, download our free course flowchart to determine which best aligns with your goals.

About the Author
Addressing employee burnout: Are you solving the right problem?
The COVID-19 pandemic has accelerated and exacerbated long-standing corporate challenges to employee health and well-being , and in particular employee mental health. 1 When used in this article, “mental health” is a term inclusive of positive mental health and the full range of mental, substance use, and neurological conditions. This has resulted in reports of rapidly rising rates of burnout 2 When used in this article, “burnout” and “burnout symptoms” refer to work-driven burnout symptoms (per sidebar “What is burnout?”). around the world (see sidebar “What is burnout?”).
About the authors
This article is a collaborative effort by Jacqueline Brassey , Erica Coe , Martin Dewhurst, Kana Enomoto , Renata Giarola, Brad Herbig, and Barbara Jeffery , representing the views of the McKinsey Health Institute.
Many employers have responded by investing more into mental health and well-being than ever before. Across the globe, four in five HR leaders report that mental health and well-being is a top priority for their organization. 3 McKinsey Health Institute Employee Mental Health and Wellbeing Survey, 2022: n (employee) = 14,509; n (HR decision maker) = 1,389. Many companies offer a host of wellness benefits such as yoga, meditation app subscriptions, well-being days, and trainings on time management and productivity. In fact, it is estimated that nine in ten organizations around the world offer some form of wellness program. 4 Charlotte Lieberman, “What wellness programs don’t do for workers,” Harvard Business Review , August 14, 2019.
As laudable as these efforts are, we have found that many employers focus on individual-level interventions that remediate symptoms, rather than resolve the causes of employee burnout. 5 Anna-Lisa Eilerts et al., “Evidence of workplace interventions—A systematic review of systematic reviews,” International Journal of Environmental Research and Public Health , 2019, Volume 16, Number 19. Employing these types of interventions may lead employers to overestimate the impact of their wellness programs and benefits 6 Katherine Baicker et al., “Effect of a workplace wellness program on employee health and economic outcomes: A randomized clinical trial,” JAMA , 2019, Volume 321, Number 15; erratum published in JAMA , April 17, 2019. and to underestimate the critical role of the workplace in reducing burnout and supporting employee mental health and well-being. 7 Pascale M. Le Blanc, et al., “Burnout interventions: An overview and illustration,” in Jonathan R. B. Halbesleben’s Handbook of Stress and Burnout in Health Care , New York, NY: Nova Science Publishers, 2008; Peyman Adibi et al., “Interventions for physician burnout: A systematic review of systematic reviews,” International Journal of Preventive Medicine , July 2018, Volume 9, Number 1.
What is burnout?
According to the World Health Organization, burnout is an occupational phenomenon. It is driven by a chronic imbalance between job demands 1 Job demands are physical, social, or organizational aspects of the job that require sustained physical or mental effort and are therefore associated with certain physiological and psychological costs—for example, work overload and expectations, interpersonal conflict, and job insecurity. Job resources are those physical, social, or organizational aspects of the job that may do any of the following: (a) be functional in achieving work goals; (b) reduce job demands and the associated physiological and psychological costs; (c) stimulate personal growth and development such as feedback, job control, social support (Wilmar B. Schaufeli and Toon W. Taris, “A critical review of the job demands-resources model: Implications for improving work and health,” from Georg F. Bauer and Oliver Hämmig’s Bridging Occupational, Organizational and Public Health: A Transdisciplinary Approach , first edition, Dordrecht, Netherlands: Springer, 2014). (for example, workload pressure and poor working environment) and job resources (for example, job autonomy and supportive work relationships). It is characterized by extreme tiredness, reduced ability to regulate cognitive and emotional processes, and mental distancing. Burnout has been demonstrated to be correlated with anxiety and depression, a potential predictor of broader mental health challenges. 2 Previous meta-analytic findings demonstrate moderate positive correlations of burnout with anxiety and depression—suggesting that anxiety and depression are related to burnout but represent different constructs (Katerina Georganta et al., “The relationship between burnout, depression, and anxiety: A systematic review and meta-analysis,” Frontiers in Psychology , March 2019, Volume 10, Article 284). When used in this article, burnout does not imply a clinical condition.
Research shows that, when asked about aspects of their jobs that undermine their mental health and well-being, 8 Paula Davis, Beating Burnout at Work: Why Teams Hold the Secret to Well-Being and Resilience , Philadelphia, PA: Wharton School Press, 2021. employees frequently cite the feeling of always being on call, unfair treatment, unreasonable workload, low autonomy, and lack of social support. 9 Jennifer Moss, The Burnout Epidemic: The Rise of Chronic Stress and How We Can Fix It , Boston, MA: Harvard Business Review Press, 2021. Those are not challenges likely to be reversed with wellness programs. In fact, decades of research suggest that interventions targeting only individuals are far less likely to have a sustainable impact on employee health than systemic solutions, including organizational-level interventions. 10 Hanno Hoven et al., “Effects of organisational-level interventions at work on employees’ health: A systematic review,” BMC Public Health , 2014, Volume 14, Number 135.
Since many employers aren’t employing a systemic approach, many have weaker improvements in burnout and employee mental health and well-being than they would expect, given their investments.
Organizations pay a high price for failure to address workplace factors 11 Gunnar Aronsson et al., “A systematic review including meta-analysis of work environment and burnout symptoms,” BMC Public Health , 2017, Volume 17, Article 264. that strongly correlate with burnout, 12 Sangeeta Agrawal and Ben Wigert, “Employee burnout, part 1: The 5 main causes,” Gallup, July 12, 2018. such as toxic behavior. 13 The high cost of a toxic workplace culture: How culture impacts the workforce — and the bottom line , Society for Human Resource Management, September 2019. A growing body of evidence, including our research in this report, sheds light on how burnout and its correlates may lead to costly organizational issues such as attrition. 14 Caio Brighenti et al., “Why every leader needs to worry about toxic culture,” MIT Sloan Management Review, March 16, 2022. Unprecedented levels of employee turnover—a global phenomenon we describe as the Great Attrition —make these costs more visible. Hidden costs to employers also include absenteeism, lower engagement, and decreased productivity. 15 Eric Garton, “Employee burnout is a problem with the company, not the person,” Harvard Business Review , April 6, 2017.
The McKinsey Health Institute: Join us!
The McKinsey Health Institute (MHI) is an enduring, non-profit-generating global entity within McKinsey. MHI strives to catalyze actions across continents, sectors, and communities to achieve material improvements in health, empowering people to lead their best possible lives. MHI is fostering a strong network of organizations committed to this aspiration, including employers globally who are committed to supporting the health of their workforce and broader communities.
MHI has a near-term focus on the urgent priority of mental health, with launch of a flagship initiative around employee mental health and well-being. By convening leading employers, MHI aims to collect global data, synthesize insights, and drive innovation at scale. Through collaboration, we can truly make a difference, learn together, and co-create solutions for workplaces to become enablers of health—in a way that is good for business, for employees, and for the communities in which they live.
To stay updated about MHI’s initiative on employee mental health and well-being sign up at McKinsey.com/mhi/contact-us .
In this article, we discuss findings of a recent McKinsey Health Institute (MHI) (see sidebar “The McKinsey Health Institute: Join us!”) global survey that sheds light on frequently overlooked workplace factors underlying employee mental health and well-being in organizations around the world. We conclude by teeing up eight questions for reflection along with recommendations on how organizations can address employee mental-health and well-being challenges by taking a systemic approach focused on changing the causes rather than the symptoms of poor outcomes. While there is no well-established playbook, we suggest employers can and should respond through interventions focused on prevention rather than remediation.
We are seeing persistent burnout challenges around the world
To better understand the disconnection between employer efforts and rising employee mental-health and well-being challenges (something we have observed since the start of the pandemic ), between February and April 2022 we conducted a global survey of nearly 15,000 employees and 1,000 HR decision makers in 15 countries. 16 Argentina, Australia, Brazil, China, Egypt, France, Germany, India, Japan, Mexico, South Africa, Switzerland, Turkey, the United Kingdom, and the United States. The combined population of the selected countries correspond to approximately 70 percent of the global total.
The workplace dimensions assessed in our survey included toxic workplace behavior, sustainable work, inclusivity and belonging, supportive growth environment, freedom from stigma, organizational commitment, leadership accountability, and access to resources. 17 The associations of all these factors with employee health and well-being have been extensively explored in the academic literature. That literature heavily informed the development of our survey instrument. We have psychometrically validated this survey across 15 countries including its cross-cultural factorial equivalence. For certain outcome measures we collaborated with academic experts who kindly offered us their validated scales including the Burnout Assessment Tool (BAT), the Distress Screener, and the Adaptability Scale referenced below. Those dimensions were analyzed against four work-related outcomes—intent to leave, work engagement, job satisfaction, and organization advocacy—as well as four employee mental-health outcomes—symptoms of anxiety, burnout, depression, and distress. 18 Instruments used were the Burnout Assessment Tool (Steffie Desart et al., User manual - Burnout assessment tool [BAT ] , - Version 2.0, July 2020) (burnout symptoms); Distress Screener (4DSQ; JR Anema et al., “Validation study of a distress screener,” Journal of Occupational Rehabilitation , 2009, Volume 19) (distress); GAD-2 assessment (Priyanka Bhandari et al., “Using Generalized Anxiety Disorder-2 [GAD-2] and GAD-7 in a primary care setting,” Cureus , May 20, 2021, Volume 12, Number 5) (anxiety symptoms); and the PHQ-2 assessment (Patient Health Questionnaire [PHQ-9 & PHQ-2], American Psychological Association) (depression symptoms). Individual adaptability was also assessed 19 In this article, “adaptability” refers to the “affective adaptability” which is one sub-dimension of The Adaptability Scale instrument (Michel Meulders and Karen van Dam, “The adaptability scale: Development, internal consistency, and initial validity evidence,” European Journal of Psychological Assessment , 2020, Volume 37, Number 2). (see sidebar “What we measured”).
What we measured
Workplace factors assessed in our survey included:
- Toxic workplace behavior: Employees experience interpersonal behavior that leads them to feel unvalued, belittled, or unsafe, such as unfair or demeaning treatment, noninclusive behavior, sabotaging, cutthroat competition, abusive management, and unethical behavior from leaders or coworkers.
- Inclusivity and belonging: Organization systems, leaders, and peers foster a welcoming and fair environment for all employees to be themselves, find connection, and meaningfully contribute.
- Sustainable work: Organization and leaders promote work that enables a healthy balance between work and personal life, including a manageable workload and work schedule.
- Supportive growth environment: Managers care about employee opinions, well-being, and satisfaction and provide support and enable opportunities for growth.
- Freedom from stigma and discrimination: Freedom from the level of shame, prejudice, or discrimination employees perceive toward people with mental-health or substance-use conditions.
- Organizational accountability: Organization gathers feedback, tracks KPIs, aligns incentives, and measures progress against employee health goals.
- Leadership commitment: Leaders consider employee mental health a top priority, publicly committing to a clear strategy to improve employee mental health.
- Access to resources: Organization offers easy-to-use and accessible resources that fit individual employee needs related to mental health. 1 Including adaptability and resilience-related learning and development resources.
Health outcomes assessed in our survey included:
- Burnout symptoms: An employee’s experience of extreme tiredness, reduced ability to regulate cognitive and emotional processes, and mental distancing (Burnout Assessment Tool). 2 Burnout Assessment Tool, Steffie Desart et al., “User manual - Burnout assessment tool (BAT), - Version 2.0,” July 2020.
- Distress: An employee experiencing a negative stress response, often involving negative affect and physiological reactivity (4DSQ Distress Screener). 3 Distress screener, 4DSQ; JR Anema et al., “Validation study of a distress screener,” Journal of Occupational Rehabilitation , 2009, Volume 19.
- Depression symptoms: An employee having little interest or pleasure in doing things, and feeling down, depressed, or hopeless (PHQ-2 Screener). 4 Kurt Kroenke et al., “The patient health questionnaire-2: Validity of a two-item depression screener,” Medical Care , November 2003, Volume 41, Issue 11.
- Anxiety symptoms: An employee’s feelings of nervousness, anxiousness, or being on edge, and not being able to stop or control worrying (GAD-2 Screener). 5 Kurt Kroenke et al., “Anxiety disorders in primary care: Prevalence, impairment, comorbidity, and detection,” Annals of Internal Medicine , March 6, 2007, Volume 146, Issue 5.
Work-related outcomes assessed in our survey included:
- Intent to leave: An employee’s desire to leave the organization in which they are currently employed in the next three to six months.
- Work engagement: An employee’s positive motivational state of high energy combined with high levels of dedication and a strong focus on work.
- Organizational advocacy: An employee’s willingness to recommend or endorse their organization as a place to work to friends and relatives.
- Work satisfaction: An employee’s level of contentment or satisfaction with their current job.
Our survey pointed to a persistent disconnection between how employees and employers perceive mental health and well-being in organizations. We see an average 22 percent gap between employer and employee perceptions—with employers consistently rating workplace dimensions associated with mental health and well-being more favorably than employees. 20 Our survey did not link employers and employees’ responses. Therefore, these numbers are indicative of a potential gap that could be found within companies.
In this report—the first of a broader series on employee mental health from the McKinsey Health Institute—we will focus on burnout, its workplace correlates, and implications for leaders. On average, one in four employees surveyed report experiencing burnout symptoms. 21 Represents global average of respondents experiencing burnout symptoms (per items from Burnout Assessment Tool) sometimes, often, or always. These high rates were observed around the world and among various demographics (Exhibit 1), 22 Our survey findings demonstrate small but statistically significant differences between men and women, with women reporting higher rates of burnout symptoms (along with symptoms of distress, depression, and anxiety). Differences between demographic variables across countries will be discussed in our future publications. and are consistent with global trends. 23 Ashley Abramson, “Burnout and stress are everywhere,” Monitor on Psychology , January 1, 2022, Volume 53, Number 1.
So, what is behind pervasive burnout challenges worldwide? Our research suggests that employers are overlooking the role of the workplace in burnout and underinvesting in systemic solutions.
Employers tend to overlook the role of the workplace in driving employee mental health and well-being, engagement, and performance
In all 15 countries and across all dimensions assessed, toxic workplace behavior was the biggest predictor of burnout symptoms and intent to leave by a large margin 24 Measured as a function of predictive power of the dimensions assessed; predictive power was estimated based on share of outcome variability associated with each dimension; based on regression models applied to cross-sectional data (that is, measured at one point in time), rather than longitudinal data (that is, measured over time); causal relationships have not been established. —predicting more than 60 percent of the total global variance. For positive outcomes (including work engagement, job satisfaction, and organization advocacy), the impact of factors assessed was more distributed—with inclusivity and belonging, supportive growth environment, sustainable work, and freedom from stigma predicting most outcomes (Exhibit 2).
In all 15 countries and across all dimensions assessed, toxic workplace behavior had the biggest impact predicting burnout symptoms and intent to leave by a large margin.
The danger of toxic workplace behavior—and its impact on burnout and attrition
Across the 15 countries in the survey, toxic workplace behavior is the single largest predictor of negative employee outcomes, including burnout symptoms (see sidebar “What is toxic workplace behavior?”). One in four employees report experiencing high rates of toxic behavior at work. At a global level, high rates were observed across countries, demographic groups—including gender, organizational tenure, age, virtual/in-person work, manager and nonmanager roles—and industries. 25 Differences between demographic variables across countries will be discussed in our future articles.
What is toxic workplace behavior?
Toxic workplace behavior is interpersonal behavior that leads to employees feeling unvalued, belittled, or unsafe, such as unfair or demeaning treatment, non-inclusive behavior, sabotaging, cutthroat competition, abusive management, and unethical behavior from leaders or coworkers. Selected questions from this dimension include agreement with the statements “My manager ridicules me,” “I work with people who belittle my ideas,” and “My manager puts me down in front of others.”
Toxic workplace behaviors are a major cost for employers—they are heavily implicated in burnout, which correlates with intent to leave and ultimately drives attrition. In our survey, employees who report experiencing high levels of toxic behavior 26 “High” represents individuals in the top quartile of responses and “low” represents individuals in the bottom quartile of responses. at work are eight times more likely to experience burnout symptoms (Exhibit 3). In turn, respondents experiencing burnout symptoms were six times more likely to report they intend to leave their employers in the next three to six months (consistent with recent data pointing to toxic culture as the single largest predictor of resignation during the Great Attrition, ten times more predictive than compensation alone 27 Charles Sull et al., “Toxic culture is driving the Great Resignation,” MIT Sloan Management Review, January 11, 2022. and associated with meaningful organizational costs 28 Rasmus Hougaard, “To stop the Great Resignation, we must fight dehumanization at work,” Potential Project, 2022. ). The opportunity for employers is clear. Studies show that intent to leave may correlate with two- to three-times higher 29 Bryan Bohman et al., “Estimating institutional physician turnover attributable to self-reported burnout and associated financial burden: A case study,” BMC Health Services Research , November 27, 2018, Volume 18, Number 1. rates of attrition; conservative estimates of the cost of replacing employees range from one-half to two times their annual salary. Even without accounting for costs associated with burnout—including organizational commitment 30 Michael Leiter and Christina Maslach, “The impact of interpersonal environment on burnout and organizational commitment,” Journal of Organizational Behavior , October 1988, Volume 9, Number 4. and higher rates of sick leave and absenteeism 31 Arnold B. Bakker et al., “Present but sick: A three-wave study on job demands, presenteeism and burnout,” Career Development International , 2009, Volume 14, Number 1. —the business case for addressing it is compelling. The alternative—not addressing it—can lead to a downward spiral in individual and organizational performance. 32 Arnold B. Bakker et al., “Present but sick: A three-wave study on job demands, presenteeism and burnout,” Career Development International , 2009, Volume 14, Number 1.
Individuals’ resilience and adaptability skills may help but do not compensate for the impact of a toxic workplace
Toxic behavior is not an easy challenge to address. Some employers may believe the solution is simply training people to become more resilient.
There is merit in investing in adaptability and resiliency skill building . Research indicates that employees who are more adaptable tend to have an edge in managing change and adversity. 33 Karen van Dam, “Employee adaptability to change at work: A multidimensional, resource-based framework,” from The Psychology of Organizational Change: Viewing Change from the Employee’s Perspective , Cambridge, England: Cambridge University Press, 2013; Jacqueline Brassey et al., Advancing Authentic Confidence Through Emotional Flexibility: An Evidence-Based Playbook of Insights, Practices and Tools to Shape Your Future , second edition, Morrisville, NC: Lulu Press, 2019; B+B Vakmedianet B.V. Zeist, Netherlands (to be published Q3 2022). We see that edge reflected in our survey findings: adaptability acts as a buffer 34 Estimated buffering effect illustrated in Exhibit 4. to the impact of damaging workplace factors (such as toxic behaviors), while magnifying the benefit of supportive workplace factors (such as a supportive growth environment) (Exhibit 4). In a recent study, employees engaging in adaptability training experienced three times more improvement in leadership dimensions and seven times more improvement in self-reported well-being than those in the control group. 35 McKinsey’s People and Organization Performance - Adaptability Learning Program; multirater surveys showed improvements in adaptability outcomes, including performance in role, sustainment of well-being, successfully adapting to unplanned circumstances and change, optimism, development of new knowledge and skills; well-being results were based on self-reported progress as a result of the program.
However, employers who see building resilience and adaptability skills in individuals as the sole solution to toxic behavior and burnout challenges are misguided. Here is why.
Individual skills cannot compensate for unsupportive workplace factors. When it comes to the effect of individual skills, leaders should be particularly cautious not to misinterpret “favorable” outcomes (for example, buffered impact of toxic behaviors across more adaptable employees) as absence of underlying workplace issues that should be addressed. 36 Tomas Chamorro-Premuzic, “To prevent burnout, hire better bosses,” Harvard Business Review , August 23, 2019.
Also, while more adaptable employees are better equipped to work in poor environments, they are less likely to tolerate them. In our survey, employees with high adaptability were 60 percent more likely to report intent to leave their organization if they experienced high levels of toxic behavior at work than those with low adaptability (which may possibly relate to a higher level of self-confidence 37 Brassey et al. found that as a result of a learning program, employees who developed emotional flexibility skills, a concept related to affective adaptability but also strongly linked to connecting with purpose, developed a higher self-confidence over time; Jacqueline Brassey et al., “Emotional flexibility and general self-efficacy: A pilot training intervention study with knowledge workers,” PLOS ONE , October 14, 2020, Volume 15, Number 10. ). Therefore, relying on improving employee adaptability without addressing broader workplace factors puts employers at an even higher risk of losing some of its most resilient, adaptable employees.
Employees with high adaptability were 60 percent more likely to report intent to leave their organization if they experienced high levels of toxic behavior at work than those with low adaptability.
What this means for employers: Why organizations should take a systemic approach to improving employee mental health and well-being
We often think of employee mental health, well-being, and burnout as a personal problem. That’s why most companies have responded to symptoms by offering resources focused on individuals such as wellness programs.
However, the findings in our global survey and research are clear. Burnout is experienced by individuals, but the most powerful drivers of burnout are systemic organizational imbalances across job demands and job resources. So, employers can and should view high rates of burnout as a powerful warning sign that the organization—not the individuals in the workforce—needs to undergo meaningful systematic change.
Employers can and should view high rates of burnout as a powerful warning sign that the organization—not the individuals in the workforce—needs to undergo meaningful systematic change.
Taking a systemic approach means addressing both toxic workplace behavior and redesigning work to be inclusive, sustainable, and supportive of individual learning and growth, including leader and employee adaptability skills. It means rethinking organizational systems, processes, and incentives to redesign work, job expectations, and team environments.
As an employer, you can’t “yoga” your way out of these challenges. Employers who try to improve burnout without addressing toxic behavior are likely to fail. Our survey shows that improving all other organization factors assessed (without addressing toxic behavior) does not meaningfully improve reported levels of burnout symptoms. Yet, when toxic behavior levels are low, each additional intervention contributes to reducing negative outcomes and increasing positive ones.
The interactive graphic shows the estimated interplay between the drivers and outcomes, based on our survey data (Exhibit 5).
Taking a preventative, systemic approach—focused on addressing the roots of the problem (as opposed to remediating symptoms)—is hard. But the upside for employers is a far greater ability to attract and retain valuable talent over time.
The good news: Although there are no silver bullets, there are opportunities for leaders to drive material change
We see a parallel between the evolution of global supply chains and talent. Many companies optimized supply chains for “just in time” delivery, and talent was optimized to drive operational efficiency and effectiveness. As supply chains come under increasing pressure, many companies recognize the need to redesign and optimize supply chains for resilience and sustainability, and the need to take an end-to-end approach to the solutions. The same principles apply to talent.
We acknowledge that the factors associated with improving employee mental health and well-being (including organizational-, team-, and individual-level factors) are numerous and complex. And taking a whole-systems approach is not easy.
Would you like to learn more about the McKinsey Health Institute ?
Despite the growing momentum toward better employee mental health and well-being (across business and academic communities), we’re still early on the journey. We don’t yet have sufficient evidence to conclude which interventions work most effectively—or a complete understanding of why they work and how they affect return on investment.
That said, efforts to mobilize the organization to rethink work—in ways that are compatible with both employee and employer goals—are likely to pay off in the long term. To help spark that conversation in your organization, we offer eight targeted questions and example strategies with the potential to address some of the burnout-related challenges discussed in this article.
Do we treat employee mental health and well-being as a strategic priority?
This is fundamental to success. When a large organization achieved a 7 percent reduction in employee burnout rates (compared with an 11 percent increase in the national average within the industry over the same period), the CEO believed that leadership and sustained attention from the highest level of the organization were the “key to making progress.” 38 John H. Noseworthy and Tait D Shanafelt, “Executive leadership and physician well‐being: Nine organizational strategies to promote engagement and reduce burnout,” Mayo Clinic Proceedings , January 2017, Volume 92, Number 1. Senior executives recognized employee mental health and well-being as a strategic priority. Executives publicly acknowledged the issues and listened to employee needs through a wide range of formats—including town halls, workshops, and employee interviews (our research suggests that leaders are not listening to their people nearly enough). They prioritized issues and defined clear, time-bound measurable goals around them—with a standardized measure of burnout being given equal importance to other key performance metrics (financial metrics, safety/quality, employee turnover, and customer satisfaction). Although anonymous at the level of the individual, results were aggregated at division/department level to allow executive leadership to focus attention and resources where they were most needed. 39 Liselotte Dyrbye et al., “Physician burnout: Contributors, consequences and solutions,” Journal of Internal Medicine , 2018, Volume 283, Number 6. This example highlights how CEOs have the ability to create meaningful change through listening to employees and prioritizing strategies to reduce burnout.
Do we effectively address toxic behaviors?
Eliminating toxic workplace behavior is not an easy task. Organizations that tackle toxic behavior effectively deploy a set of integrated work practices to confront the problem, 40 Robert I. Sutton, The No Asshole Rule: Building a Civilized Workplace and Surviving One That Isn’t , first edition, New York, NY: Business Plus, 2010. and see treatment of others as an integral part of assessing an employee’s performance. Manifestations of toxic behavior 41 “Why every leader,” 2022. are flagged, repeat offenders either change or leave, and leaders take time to become aware of the impact their behavior has on others. If you lead part of an organization, looking at your own behaviors, and what you tolerate in your own organization, is a good place to start. 42 “ Author Talks: How to handle your work jerk ,” March 29, 2022.
Leaders with higher self-regulation may be better, less toxic leaders
Research shows that leaders’ development of self-regulation increases followers’ ratings of their effectiveness and is associated with higher team financial performance as well as a higher final team grade compared with a control group. The benefits of self-regulation also improved leaders’ development of task-relevant competencies. 1 Robin Martin and JooBee Yeow, “The role of self-regulation in developing leaders: A longitudinal field experiment,” Leadership Quarterly , October 2013, Volume 24, Number 5. Furthermore, building employees’ resilience and adaptability skills leads to a higher sense of agency and self-efficacy, 2 Jacqueline Brassey et al., “Emotional flexibility and general self-efficacy: A pilot training intervention study with knowledge workers,” PLOS ONE , October 14, 2020, Volume 15, Number 10; and Jacqueline Brassey et al., Advancing Authentic Confidence Through Emotional Flexibility: An Evidence-Based Playbook of Insights, Practices and Tools to Shape Your Future , second edition, Morrisville, NC: Lulu Press, 2019; B+B Vakmedianet B.V. Zeist, Netherlands (to be published Q3 2022). which is related to reduced burnout and improved performance. 3 Charles Benight et al., “Associations between job burnout and self-efficacy: A meta-analysis,” Anxiety, Stress, & Coping , 2016, Volume 29, Issue 4; and Alex Stajkovic, “Self-efficacy and work-related performance: A meta-analysis,” Psychological Bulletin , 1998, Volume 124, Number 2.
Another component of eliminating toxic behavior is cultivating supportive, psychologically safe work environments , where toxic behaviors are less likely to spread across the organization. 43 Annie McKee, “Neutralize your toxic boss,” Harvard Business Review , September 24, 2008. Effective leaders know that emotional contagion 44 John T. Cacioppo et al., Emotional Contagion , Cambridge, England: Cambridge University Press, 1994. may go both ways: displaying vulnerability and compassion fuels more compassionate teams; displaying toxic behavior fuels more toxic teams. 45 Michael Housman and Dylan Minor, Toxic workers , Harvard Business School working paper, No. 16-057, October 2015 (revised November 2015). There are two caveats: toxic behavior may not be intentional—particularly if individuals are not equipped to respond with calm and compassion under pressure—and regardless of intent, toxic behavior spreads faster and wider than good behavior. 46 “To prevent burnout,” 2019. To prevent unintentional dissemination of toxic behaviors, role modeling from adaptable , self-regulating, compassionate leaders may help (see sidebar “Leaders with higher self-regulation may be better, less toxic leaders”).
Do we create inclusive work environments?
Most leaders recognize the established associations between performance and inclusion , but inclusion does not happen by accident . Inclusion is a multifaceted construct that must be addressed comprehensively and proactively. Most companies define inclusion too narrowly and thus address it too narrowly as well. Over the past three years, we’ve broadened our perspective on how to create truly inclusive workplaces and developed a modern inclusion model . The model includes 17 practices (based on frequency of desired behaviors) and six outcomes (based on perceptions of effectiveness). Each practice falls into one of three relationships that shape workplace inclusion: organizational systems, leaders, and peers/teammates.
The 17 inclusive-workplace practices , when done consistently well, drive workplace inclusion and equity for all employees by providing clarity into actions that matter. For example, among employees working in hybrid models , work–life support was the top practice employees desired improvements on—with nearly half of employees recommending prioritizing policies that support flexibility—including extended parental leave, flexible hours, and work-from-home policies.
A truly inclusive workplace implements systems that minimize conscious and unconscious bias , allowing employees to express themselves and connect with each other. It also features leaders who not only advocate for team members and treat them impartially but also uphold and support all organizational systems and practices . For example, one employer defined data-driven targets for the representation and advancement of diverse talent across dimensions (beyond gender and ethnicity) and role types (executive, management, technical, board)—leveraging powerful analytics to track progress and foster transparency along the way.
Do we enable individual growth?
Evidence suggests that individual growth, learning, and development programs are effective 47 Arnold B. Bakker and Evangelia Demerouti, “Towards a model of work engagement,” Career Development International , 2008, Volume 13, Issue 3. ways to combat burnout and to retain and engage employees, and therefore are important for addressing growing talent and skills shortages within organizations. Employers who “double down” on talent redeployment, mobility, reskilling, and upskilling tend to see improvement across a range of financial, organizational, and employee experience metrics. In a recent study of extensive employee data, offering lateral career opportunities was two-and-half times more predictive of employee retention than compensation, and 12 times more predictive than promotions 48 “Why every leader,” 2022. —signaling an opportunity for leaders to support employee desires to learn, explore, and grow way beyond traditional career progression.
Investing in your employees’ capabilities can drive financial returns, is often cheaper than hiring, and signals to employees that they are valued and have an important role in the organization.
Do we promote sustainable work?
Promoting sustainable work goes beyond managing workload. It’s about enabling employees to have a sense of control and predictability, flexibility, and sufficient time for daily recovery. It’s also about leading with compassion and empathy 49 “It’s time to eliminate bad bosses. They are harmful and expensive,” Potential Project, The Human Leader, April 2022. —tailoring interventions based on where, when, and how work can be done , and how different groups are more likely to (re)establish socio-emotional ties after a long period of isolation and loss of social cohesion .
One technology company is using real-time data on employee preferences to rapidly test and iterate solutions that work for specific groups around return-to-office options. To find solutions that work for your employees, consider adopting a test-and-learn mindset. This approach can help the organization make progress while adapting as context evolves (a hallmark of more productive organizations).
Are we holding leaders accountable?
Many organizations consider people leadership criteria in their performance management. Yet, there is substantial room to grow when it comes to employers providing transparency around employee mental-health and well-being objectives and metrics. 50 Workplace Mental Health Blogs , One Mind, “Fix performance management by aligning it with employee mental health,” blog entry by Daryl Tol, March 2, 2022; Garett Slettebak, “Measuring progress on workplace mental health”, One Mind at Work, March 24, 2022.
Organizations that are doing this well have set clear expectations for managers to lead in a way that is supportive of employee mental health and well-being. 51 Taylor Adams et al., Mind the workplace: Work health survey 2021 , Mental Health America, 2021. They offer training to help managers identify, proactively ask about, and listen to employees’ mental-health and well-being needs. They also introduce mental-health “pulse” checks and incorporate relevant questions into the broader employee satisfaction surveys, to establish a baseline and track trends in how employees are feeling. Discussion on employee mental health and well-being can be incorporated into regular leadership meetings, including concerns, risks, and potential actions.
To encourage leaders to lead by example and increase their accountability, some employers embed employee mental-health support into leaders’ reviews based on anonymous upward feedback from their teams. Finally, some companies are exploring if they can go even further and tie incentives to short- and long-term employee mental-health and well-being objectives.
Are we effectively tackling stigma?
As noted in a previous McKinsey article , the majority of employers and employees acknowledge the presence of stigma 52 In the context of employee mental health, stigma is defined as a level of shame, prejudice, or discrimination toward people with mental-health or substance-use conditions. in their workplaces. Stigma has been shown to have real costs to workforce productivity, often exacerbating underlying conditions because of people being afraid to seek help for mental-health needs and driving down an employee’s self-worth and engagement.
We see several actions that organizations are taking to eliminate stigma. 53 Erica Coe, Jenny Cordina, Kana Enomoto, and Nikhil Seshan, “ Overcoming stigma: Three strategies toward better mental health in the workplace ,” July 23, 2021. Leading by example can make a difference, with senior leaders stepping forward to describe personal struggles with mental health, using nonstigmatizing language. 54 Evelien Brouwers et al., “To disclose or not to disclose: A multi-stakeholder focus group study on mental health issues in the work environment. Journal of Occupational Rehabilitation , 2020, Volume 30, Number 1. Leaders showing vulnerability helps to remove shame and promote a psychologically safe culture. 55 Global thriving at work framework , MindForward Alliance, 2020.
Stigma can also be reduced by companies prioritizing mental wellness as critical for peak performance instead of rewarding overwork at the expense of rest and renewal—rewarding an “athlete” mindset instead of overemphasizing a “hero.” This can begin to shift perception of signs of burnout or other mental-health needs as being indicative of a moral failing. Finally, creating a dedicated role to support employee mental health and well-being and appointing a senior leader, such as chief wellness officer, will increase awareness and show commitment.
Do our resources serve employee needs?
Leaders should evaluate whether mental-health and well-being resources are at parity with physical-health benefits and how frequently they are being used by employees. An increasing number of employers have expanded access to mental-health services 56 Charles Ingoglia, “Now more than ever, employers must provide mental health support for employees,” National Council for Mental Wellbeing, May 4, 2022. ; however, research shows that almost 70 percent of employees find it challenging to access those services.
In a previous survey , 45 percent of respondents who had left their jobs cited the need to take care of family as an influential factor in their decision (with a similar proportion of respondents who are considering quitting also citing the demands of family care). Expanding childcare, nursing services, or other home- and family-focused benefits could help keep such employees from leaving and show that you value them. Patagonia, long the standard-bearer for progressive workplace policies, retains nearly 100 percent of its new mothers with on-site childcare and other benefits for parents.
Never in history have organizations around the world devoted so much attention and capital to improving employee mental health and well-being. It is lamentable that these investments are not always providing a good return regarding improved outcomes. Employers that take the time to understand the problem at hand—and pursue a preventative, systemic approach focused on causes instead of symptoms—should see material improvements in outcomes and succeed in attracting and retaining valuable talent. More broadly, employers globally have an opportunity to play a pivotal role in helping people achieve material improvements in health. With collaboration and shared commitment, employers can make a meaningful difference in the lives of their employees and the communities they live in.
The McKinsey Health Institute (MHI) is collaborating with leading organizations around the world to achieve material improvements in health—adding years to life and life to years. As part of that, MHI is focused on improving employee mental health and well-being at scale—in a way that is good for business, for employees, and for the communities they live in.
To stay updated about MHI’s initiative on employee mental health and well-being, sign up at McKinsey.com/mhi/contact-us .
Jacqueline Brassey is a director of research science in McKinsey’s Luxemburg office, Erica Coe is a partner in the Atlanta office, Martin Dewhurst is a senior partner in the London office, Kana Enomoto is a senior expert in the Washington, DC, office, and Barbara Jeffery is a partner in the London office; they are all leaders with McKinsey Health Institute (MHI). Renata Giarola , in the Southern California office, and Brad Herbig , in the Philadelphia office, are consultants with MHI.
The authors wish to thank Yueyang Chen, Elena Chit, Aaron de Smet, Soheil Eshghi, Lars Hartenstein, Tom Latkovic, David Mendelsohn, Roxy Merkand, Isidora Mitic, Bill Schaninger, Wilmar Schaufeli, Jeris Stueland, Berend Terluin, Karen van Dam, and Marieke van Hoffen for their contributions to this article.
This article was edited by Allan Gold, a senior editorial advisor in Washington, DC, and Elizabeth Newman, an executive editor in the Chicago office.
Explore a career with us
Related articles.

Adding years to life and life to years

National surveys reveal disconnect between employees and employers around mental health need

The state of burnout for women in the workplace
- Financial Information
- Our History
- Our Leadership
- The Casey Philanthropies
- Workforce Composition
- Child Welfare
- Community Change
- Economic Opportunity
- Equity and Inclusion
- Evidence-Based Practice
- Juvenile Justice
- Leadership Development
- Research and Policy
- Child Poverty
- Foster Care
- Juvenile Probation
- Kinship Care
- Racial Equity and Inclusion
- Two-Generation Approaches
- See All Other Topics
- Publications
- KIDS COUNT Data Book
- KIDS COUNT Data Center
2024 KIDS COUNT Data Book
2024 state trends in child well-being.

The 35th edition of the Annie E. Casey Foundation's KIDS COUNT ® Data Book examines the unprecedented declines in student math and reading proficiency brought on by the COVID-19 pandemic's effect on education . The latest data from the National Assessment of Educational Progress reveals that between 2019 and 2022, fourth-grade reading and eighth-grade math scores plummeted, representing decades of lost progress. This alarming trend underscores the urgent need for action to address the growing academic disparities among U.S. students.
Today's students, who will comprise America's future workforce, are ill-prepared for the high-level reading, math and problem-solving skills required in a competitive global economy. The failure to adequately prepare our children will have dire consequences for their futures and for the economic vitality of our nation.
Learn more about pandemic learning loss and Casey's recommendations to ensure student success
National Trends in Child Well-Being
In 2022, as COVID-19 restrictions eased, the impact of the pandemic on child well-being became evident. Six indicators worsened between 2019 and 2022, including educational achievement and the child and teen death rate. Between 2019 and 2021, the percentage of children scoring proficient or above in reading and math declined sharply. While this trend may have stabilized in 2022, the data indicate a significant setback in educational attainment. The child and teen death rate also remained elevated in 2022, with 17.0 deaths per 100,000 children and adolescents, compared to 14.7 in 2019.
However, some positive trends emerged:
- Parents' economic security improved significantly, with 62.4% of children living in economically secure homes in 2022, compared to 58.4% in 2021.
- The child poverty rate decreased from 17.2% in 2021 to 15.9% in 2022, returning to pre-pandemic levels.
Health and Family
Positive trends were also observed in the family and community domains. Fewer children lived with parents lacking a high school diploma, and the number of children living in high-poverty communities decreased. The teen birth rate reached a record low in 2021 and remained stable in 2022 at 14 births per 1,000 teen females.
These positive changes demonstrate how effective policies that address the root causes of challenges can contribute to significant improvements and create a brighter future for young people.
Trends in Racial Inequities
Racial inequities in America persist, with American Indian/Alaska Native, Black and Latino children facing significant disparities. Nearly all well-being indicators show disparate outcomes by race and ethnicity, with American Indian/Alaska Native children and Black children experiencing the lowest well-being levels.
Generations of inequity and discrimination contribute to these disparities. Black children have higher rates of single-parent households and poverty, while American Indian/Alaska Native children are more likely to lack health insurance and live in resource-limited neighborhoods. Latino children have higher rates of obesity and live in households where the head may lack a high school diploma.
And despite overall better outcomes for Asian and Pacific Islander children, disaggregated data reveal significant disparities within this population. Burmese, Mongolian and Thai children experience higher rates of poverty and lack of high school diplomas in their households. Today, children of color constitute the majority of the nation's children, highlighting the importance of ensuring their success for the future of America.
Data Book Extras
- 2024 KIDS COUNT Data Book Interactive
- National News Release
- Comunicado de prensa nacional en español
- State News Releases
- Auxiliary Data Tables
- Copyright Information
- Other reports in this series
State Data Profiles on Child Well-Being
View the national data profile or download your state's data profile as a PDF below:
- Connecticut
- Massachusetts
- Mississippi
- New Hampshire
- North Carolina
- North Dakota
- Pennsylvania
- Puerto Rico
- Rhode Island
- South Carolina
- South Dakota
- Washington, D.C.
- West Virginia
State Data Profiles on Child Well-Being in Spanish
View the 2024 national data profile in Spanish or download your state's data profile as a PDF below:
- Distrito de Columbia
- Nuevo Hampshire
- Nueva Jersey
- Nuevo México
- Carolina del Norte
- Dakota del Norte
- Pensilvania
- Carolina del Sur
- Dakota del Sur
- Virginia Occidental
State Trends in Overall Child Well-Being
The Foundation calculates a composite index of overall child well-being for each state by combining data across four domains: (1) Economic Well-Being, (2) Education, (3) Health and (4) Family and Community. These scores are then translated into state rankings. Explore overall child well-being in the interactive KIDS COUNT Data Book .

Northeast States Rank High for Overall Well-Being
Distinct regional patterns emerge from the state rankings. Five of the top 10 states in terms of overall child well-being are in the Northeast — Vermont (fourth), New Jersey (sixth) and Connecticut (eighth).
Household Income Has a Direct Effect on Well-Being
States in Appalachia, as well as the Southeast and Southwest — where families have the lowest levels of household income — populate the bottom of the overall rankings. In fact, except for Alaska, the 15 lowest-ranked states are in these regions.
Some States' Rankings Vary Dramatically
Although most state rankings did not vary dramatically across domains, there are a few exceptions. For example, North Dakota ranks 40th in Education but first for Economic Well-Being. New York ranks 44th in Economic Well-Being and 8th for Health. For all states, the index identified bright spots and room for improvement.
Economic Well-Being
To help children grow into prepared, productive adults, parents need jobs with family-sustaining pay, affordable housing and the ability to invest in their children’s future. Explore economic well-being in the interactive KIDS COUNT Data Book .

The Child Poverty Rate Has Improved
Nationally, 16% of children (11.6 million) lived in families below the poverty line. The child poverty rate has improved since 2019 (17%).
When parents are unemployed or earn low wages, their access to resources to support their kids’ development is more limited, which can undermine their children’s health and prospects for success in school and beyond. The negative effects of poverty on kids can extend into their teenage years and young adulthood, as they are more likely to contend with issues such as teen pregnancy and failing to graduate from high school.

Parental Employment Instability Returned to the Pre-Pandemic Rate
In 2022, 26% or 18.6 million children lived in families where no parent had full-time, year-round employment. The large increase seen between 2019 and 2021 in parental employment instability was erased by the economic recovery the country experienced in 2022. The rate in 2022 returned to the pre-pandemic rate.
Secure employment is a key contributor to families' financial stability and well-being. The COVID-19 pandemic pushed the unemployment rate to near-record highs and caused millions to leave the labor market. In 2022, job openings reached a record high as the labor market recovered. Even so, employment insecurity is a reality for more than a quarter of families living in the United States. It disrupts daily living and relationships and limit families’ access to resources to invest in their children’s development, which can, in turn, diminish children’s achievement in school and chances of future success.
High Housing-Cost Burden Remains Unchanged
In 2022, 30% of children (21.8 million) lived in families with a high housing cost burden. The rate remained unchanged since 2019.
Housing is typically one of the largest family expenses. High housing costs weigh more heavily on low-income families, who are more likely to struggle with finding affordable housing, often spending more than 30% of pretax income on a home, whether they rent or own. Paying too much for housing limits the resources families have for other necessities such as child care, food, health care and transportation as well as their ability to save and achieve financial stability.
The early years of a child’s life lay the foundation for lifelong success. Establishing the conditions that promote educational achievement for children is critical. Explore educational well-being in the interactive KIDS COUNT Data Book .
Low-Income Families Continue to Lack Access to High-Quality Early Education
During 2018–2022, 4.3 million children, ages 3 to 4 were not in school. That accounts for more than half of all children in that age group (54%).
High-quality preschool programs for 3- to 4-year-olds help set the stage for future skill development, well-being and learning, particularly for those from low-income households. These programs play an important role in preparing children for success and lead to higher levels of educational attainment, career advancement and earnings. Although Head Start and the expansion of state-funded programs since the 1990s have increased access to preschool and kindergarten, many kids — especially 3-year-olds and children living in low-income families — continue to be left out, exacerbating socioeconomic differences in educational achievement.

Improvements in Fourth-Grade Reading Mastery Erased by Pandemic
Sixty-eight percent of fourth graders in public schools were not proficient readers in 2022, an alarming rate that increased from 2019, when 66% were not proficient. Any improvement made over the past decade was erased by the pandemic.
Reading proficiency by the end of third grade is a critical marker in a child’s educational development. By fourth grade, children use reading to learn other subjects. Therefore, reading mastery at this level becomes important for students to keep up academically. Children who reach fourth grade without being able to read proficiently are more likely to struggle academically and eventually drop out of school. Low reading proficiency also can reduce earning potential and chances for career success as adults. Although there have been some improvements since the early 1990s, progress has been slow on literacy gains, and racial and income disparities remain. Unfortunately, the pandemic has erased progress made in reading proficiency levels.
Match Achievement Worsened Across Eighth Grade Groups
Eighth-grade math achievement worsened across all racial and ethnic groups between 2019 and 2022. The largest percentage point drops in proficiency were seen among white and multiracial students.
As technology continues to transform the economy, the demand grows for a workforce with aligned math and science skills and training that can keep pace with technological advancement. Students with strong math and science skills are more likely to graduate from high school, attend and complete college, earn higher incomes and take advantage of future opportunities. Even for young people who do not attend college, basic math skills and numerical literacy help with everyday tasks and personal financial management and improve employability. Ensuring kids have early and ongoing access to high-quality math education is critical for their success in school and life.
Children’s good health is fundamental to their overall development, and ensuring kids are born healthy is the first step toward improving their life chances. Poor health in childhood affects other critical aspects of children’s lives, such as school readiness and attendance, and can have lasting consequences on their future health and well-being. Explore health indicators in the interactive KIDS COUNT Data Book .

The Rate of Low Birth-Weight Babies Increased
Nationally, low birth-weight babies represented 8.6% of all live births in 2022. An increase from 2019 (8.3%). This is the highest rate witnessed in the last decade.
Birth weight is an important indicator of an infant’s health. Babies born at a low birth weight (less than 5.5 pounds) have a high probability of experiencing developmental problems and short- and long-term disabilities. They also are at greater risk of dying within the first year of life. Infections, multiple births, obesity, poor nutrition, poverty, smoking, stress and violence can increase the chances of a baby being born at a low birth weight. Compared with other affluent countries, the United States has among the highest percentage of babies born at a low birth weight, right behind Japan, Greece and Colombia.

Close to Four Million Children Lacked Health Insurance
Across the nation, 5% of children aged 18 and under (3.9 million) lacked health insurance in 2022.
Children with health insurance are more likely to have a regular source of health care they can access for preventive care services and developmental screenings, to treat acute and chronic conditions or to address injuries when they occur. Children without coverage are less likely than insured children to receive care when they need it. Having health insurance can protect families from financial crisis when a child experiences a serious or chronic illness and can help kids remain active, healthy and in school ready to learn.

Child and Teen Mortality Rate Increase Stalled
In 2022, 23,137 children and youth ages 1 to 19 died in the United States, which translates into a mortality rate of 30 deaths per 100,000 children and teens. After seeing a 20% increase between 2019 and 2021, the child and teen mortality rate increase stalled in 2022.
Accidents, primarily those involving motor vehicles, were the leading cause of death for children and youth, accounting for 28% of all deaths among children ages 1 to 14.46 As children move further into their teenage years, they encounter new, and potentially deadly, risks. In 2022, accidents, homicides and suicides accounted for 76% of deaths for teens ages 15 to 19.47. For the second year, in a row firearm-related deaths are the leading cause of death among teens.
Family and Community
Children who live in nurturing families and supportive communities have stronger personal connections and higher academic achievement. Explore familial and community well-being in the interactive KIDS COUNT Data Book .
The Percentage of Children in Single-Parent Families Did Not Change
The percentage of children living in single-parent families remains unchanged between 2019 and 2022, at 34%. In 2022, 23.3 million children lived in single-parent families.
Even with the best efforts of parents, children growing up in single-parent families typically have access to fewer economic resources and valuable time with adults than children in two-parent families in which child-raising responsibilities can be shared. For example, in 2022, 28% of single-parent families had incomes below the poverty line, compared with 6% of married couples with children. The effects of growing up in single-parent families go beyond economics, increasing the likelihood of children dropping out of school, being disconnected from the labor market and becoming teen parents.
The Rate of Parents Who Lacked a High School Diploma Improved
In 2022, 11% of children lived in households headed by an adult without a high school diploma. This is a slight improvement from 2019, where the rate was 12%. While this is only a slight improvement, the rate has been cut in half since 1990, when 22% of children lived with parents who lacked a high school diploma.
Children growing up in households with highly educated adults are better positioned for future success. These parents often are better able to provide the financial stability and security they need to foster their children’s development. Higher levels of parental education are strongly associated with better outcomes for children, including kids’ own higher educational attainment and achievement.

Fewer than 10% of Children Lived in High-Poverty Areas from 2018–2022
During the period from 2018–2022, 8% of children lived in high-poverty areas, representing a total of 5.7 million children.
High-poverty neighborhoods — where poverty rates for the total population are 30% or more — come with several challenges that affect the children and families who live there. Residents of these neighborhoods contend with poorer health, higher rates of crime and violence, poor-performing schools due to inadequate funding and limited access to support networks and job opportunities. They also experience higher levels of financial instability. These barriers make it much harder for families to move up the economic ladder.
Additional Resources on Child Well-Being
- About KIDS COUNT
- KIDS COUNT State Organizations
- The KIDS COUNT Data Center
Copyright of the text materials contained in this website is owned by the Annie E. Casey Foundation, and any use should include an appropriate citation. Read More .
How We Create the Data Book
- The KIDS COUNT Index
- Definitions and Sources
Subscribe to our newsletter to get our data, reports and news in your inbox.
The split ladder of policy problems, participation, and politicization: constitutional water change in Ecuador and Chile
- Original Paper
- Open access
- Published: 19 June 2024
Cite this article
You have full access to this open access article

- Margot Hurlbert 1 &
- Joyeeta Gupta 2
There is debate about whether complex problems should be addressed technocratically or whether they should be politicized. While many tend to favour technocratic decision-making and evidence based policy, for others politicization of policy problems is fundamental for significant policy change. But politicization does not always lead to problem solving. Nor is it always necessary. This paper addresses the question: Under what circumstances should problems be politicized, and what is the effect of such politicization? It adds politicization, through windows of opportunity, to the split ladder of participation to assess policy change through two case studies: successful and unsuccessful constitutional change in Ecuador (2008) and Chile respectively (2022). It argues that where there is no agreement on either science or policy, politicization is required to address lack of consensus in values, but constitutional protection is needed to protect minorities and the vulnerable, their access and human right to water. De-politicization stymies policy change potentially harming democracy. This paper argues for a citizen engaged exploration of the complex problem of climate change and its impacts on water, but a targeted politicization coincident with, but developed well in advance of, windows of opportunity. Moreover, policy framing correlated with complex problems continues to be a key consideration. Furthermore, alliances of disparate actors, elections of new political leaders and considerations of property rights and justice issues are paramount. Significant constitutional policy change reflects social learning, but subsequent court actions by policy entrepreneurs is required to effectively implement this change. Framing constitutional change to protect rights to water and effect international agreements (including the Warsaw International Mechanism under the climate change regime) advances water justice and may increase success.
Avoid common mistakes on your manuscript.
1 Introduction
Climate change is exacerbating water scarcity, drought, and lack of access to water, resulting in breaches of human rights and unattainable Sustainable Development Goals (SDGs). Central and South American countries have been experiencing severe drought conditions consistently since 2019, if not longer (Toreti et al., 2023 ). These national level water stresses highlight water politics and tensions in meeting international obligations for rights to water for drinking, sanitation and hygiene. Further exposed are economic considerations surrounding water as a public or private good, and processes and outcomes affecting international environmental agreements and principles of reasonable water use and participation in decision making (Mirumachi & Hurlbert, 2022 ). In Ecuador and Chile, water tensions have emerged in national politics and specifically constitutional amendment discussions.
Water tensions expose the “very contested, power-laden nature of water governance” (Mirumachi & Hurlbert, 2022 : 1) calling for anticipating, adapting and planning for its allocation between uses and users, based on stakeholder engagement (Behnassi et al., 2019 ; Bosch et al., 2019 ). Stakeholder participation in complex socio-ecological systems (SES) reduces transaction costs, increases acceptance of adaptive strategies, trust in information and management processes and willingness to accept uncertainty and unintended consequences (Conallin et al., 2017 ; Jurgilevich et al., 2021 ; Smyth et al., 2021 ).
However, some scientists favour technocratic science informed policy and decision making thereby instrumentally neutralizing ideologies and power asymmetries (Saltelli & Giampietro, 2017 ); they mis-understand the policy process. Such technocratic solutions proposed to a captive audience of policymakers misses the mark (Cairney & Oliver, 2017 ). These solutions include attempts to blend natural and social science (such as adaptive management) (Conallin et al., 2017 ) and adaptive co-management, where they become a façade for traditional hierarchical and market based management regimes (Pearson & Dare, 2019 ). Problematically, complex earth and SES problems are not always regarded as holistic, interconnected SES problems, and even policymakers often advance technocratic response to policy problems (Hurlbert, 2018 ).
The Split Ladder of Participation (Hurlbert & Gupta, 2015 ) aims to address this issue of policy framing (see Fig. 1 ). It conceptualizes the relevance and impacts of participation for different policy problem types (ranging from structured problems with little disagreement on science and values to unstructured policy problems with disagreement on science and values) together with differing communication styles, levels of trust, and nature of learning and governance needed. This Ladder has advanced participation science in relation to considerations of the nature and frame of policy problems (Basco-Carrera et al., 2017 ; Panten et al., 2018 ) and has been applied to transboundary fisheries (Morf et al., 2019 ), and knowledge production in climate, and development planning (Harvey et al., 2019 ; Wood et al.,. 2018 ).

Split Ladder of Participation; source: Hurlbert & Gupta, 2015
The Split Ladder of Participation recognized uncertainty, values, and diverse constructions of issues in both problem structuring and stakeholder engagement (ranging from manipulation and placation to the possibility that consensus is out of reach). To illustrate the Split Ladder as a strategic, evaluation and diagnostic tool we used case studies which possibly advanced the ‘rationality project’ of policy sciences (Stone, 1988 ), recognizing the ‘bounded rationality’ of the space within which policy decision-makers operate (Fischer, 2003 ).
Here, we go beyond to explore the tension between addressing complex policy problems technocratically or through the subject of politicization. We ask: under what circumstances should problems be politicized, and what is the effect of such politicization? We employ the Split Ladder as a diagnostic and evaluation tool to analyze Chile and Ecuador’s water constitutional case studies to offer insights on policy agenda setting.
Politicization is the act of making an issue that was previously unpolitical, political; or transporting an issue into the field of politics (Schmidt, 2004 ). The Split Ladder of Participation recognizes technocratic decision making in quadrant 2; politicization conversely occurs within the center of the framework where debate, discussion, and potentially political decisions are made (Hurlbert and Gupta 2018 ). Not only do we envision a systems-theoretical view of politics but also our ‘framing’ of policy allows for a discourse theoretical approach (Zurn et al., 2012 ). While the Split Ladder has been applied in situations where issues are depoliticized, or ‘rendered technical’ (Li, 2007 ; for Split Ladder application Kinnunen ( 2021 ), this paper focuses on the politicization of water in the context of constitutional reform.
First, we revisit the Split Ladder and literature that has applied it, add the ideas of windows of opportunity and expand on the element of politicization in the center of the Split Ladder figure, then with a focus on water governance we review Chile’s recent attempt at constitutional amendment (2022), and Ecuador’s successful 2008 constitutional amendment. This comparative case study contributes to a theory of politicization and complex social problems.
2 The split ladder and politicization
We elaborate further on the Split Ladder (Hurlbert & Gupta, 2015 ) in respect of politicization: (a) we expand on windows of opportunity, when problems, policies and politics come together at critical junctures resulting in policy change (Kingdon, 2011 ); (b) we consider how policy problems come to the attention of people in and around government, which requires a discussion of policy and stakeholders.
2.1 Windows of opportunity
Policy scholars document incremental and path dependent policy change based on gradual evolution of policy change. Policymakers may draw lessons from existing policies in other jurisdictions or sectors for their specific context (Rose, 1993 ). This is typical of quadrant two of the Split Ladder when structured problems (where there is a consensus on science and values) result in technocratic policymaking; here problems are not politicized. Examples include: Dunlop and Rushton’s ( 2022 ) application of quadrant two decision making for redesigning the school curriculum and advancing climate change education in a participatory, interdisciplinary creative manner to advance learning; Potting’s ( 2022 ) analysis of science and engineering knowledge production and decision making in the seaweed industry infrastructure.
However, where there is no consensus on science and/or values, politicization is needed. This may happen through focusing events such as programme review, relicensing of infrastructure (Brian & Hannah, 2017 ), crises and disasters (Birkmann et al., 2008), monitoring, and/or changes in indicators (Kingdon, 2011 ). In these situations, rapid change and ecological crises may promote the emergence of new networks and governance forms providing a window of opportunity (Folke et al., 2005 ). When applying the split ladder to groundwater, Cuadrado-Quesada and Gupta ( 2019 ) conclude that meaningful participation and policy change is unlikely unless there is a ‘water crisis.’ This crisis enables discussion in the unstructured complex problem quadrant four and the possibility of policy change and social learning.
Policy changes result from a fortuitous constellation of problems, policy proposals, and politics creating a window of opportunity. First developed in 1984, this has been widely applied (Cairney & Jones, 2016 ). Windows of opportunity open, facilitated by policy entrepreneurs (Catney & Henneberry, 2016 ), or changing political landscape (Dubois & Saunders, 2017 ). Policy entrepreneurs push their agendas softening the system, thereby building knowledge, technical feasibility, capacity of policy makers, and public acceptance. The turnover of elected officials and an administration change can open space for changing policy. These dynamics, combined with perceived national mood, set the stage for an ‘idea whose time has come’ (Kingdon, 2011 ). This enables a paradigm shift (or triple loop social learning) whereby policy changes as a result of change in values and assumptions (Prutzer et al., 2021 ).
2.2 Policy and stakeholders
While the Split Ladder conflated actors and policies (however, expanded in Hurlbert et al., 2019 ), this article widens the discussion. While the policy ecology is metaphorically described as a garbage can model of organizational choice (Cohen et al., 1972 ), others describe it as a ‘policy primeval soup’ in which specialists try out combinations of ideas from a smorgasbord of policies (Kingdon, 2011 ). Policy proposals survive when they meet criteria from technical feasibility, fit with dominant values and current national mood, budgetary workability, and political support (ibid.).
Policies depend on the support and attention of policy actors. Elected officials, and bureaucrats under their direction, make policy by agenda setting, specifying alternative policy choices, legislating and implementing decisions. Policy change occurs through interactions between theorists who propose ideas, framers who transmit ideas like gatekeepers (bureaucrats, academics), constituents representing public sentiments (voters) and brokers who transport ideas (acting as public relations experts, advisors, think tanks and epistemic communities)(Campbell, 2004 ). This can happen through advocacy coalitions of actors from different institutions who share basic beliefs and jointly propose policies (Sabatier & Jenkins-Smith, 1993 ) possibly based on narrative storylines (Hajer, 2005 ). Since political contestations deliver policy change, policy may not be congruent to surveyed public opinion (Kinnunen, 2021 ).
Water and climate governance is inherently political as it brings together conflicting values (such as support or opposition to fossil fuel development (Roth et al., 2017 ) or competing human rights to water (Robina Ramírez & Sañudo-Fontaneda, 2018 ). Depoliticizing such complex issues reduces trust in government and harms democracy (Roth et al., 2017 ; Dunlop et al., 2021 ; Hoogesteger, 2012 ). To assess quadrant four of the Split Ladder of Participation and policy change, this paper compares Ecuador and Chile’s attempts at constitutional change.
3 Case study method
We use a qualitative comparative case study to understand when problems should be politicized, and the effect of such politicization. We study two cases of (un)successful constitutional change to explore the politicization and the mechanisms of change. Here constitutional change is synonymous with policy change defined as, “a course of action or principle adopted or proposed by a government, part, business, or individual” (OECD 2008: n.p.) and a recognized heuristic, complex, unit of case study analysis of legal change (Husa, 2020 ).
We present a narrative of decision processes of national constitutional change (Yin, 2017 ; Jensen and Rogers 2001 ). While the dependent variable is constitutional water politicization, the independent variables are institutional and structural dimensions of citizen engagement, emergent framing narratives (Schmidt, 2010 ), and consequences (or outcomes); these dimensions influence the flow of ideas, influence and actions (Parreira do Amaral, 2022 ; Bartlett & Vavrus, 2017 ). The narratives are based on a literature review, secondary sources, constitutional texts and proposals, and relevant submissions or positions of interested parties.
3.1 Two constitutional water cases
3.1.1 the chilean water constitution case.
South America in general, and Chile in particular, is suffering from the impacts of climate variability and change especially through glacier mass loss worldwide (20–60% in the Andes since 1985), extreme floods and droughts, and resulting impacts on agriculture (Castellanos et al., 2022 ). The ‘Central Chile Mega Drought’ entered its thirteenth year in 2022; central Chile has had a 76% deficit in rainfall in the 2020s of a ‘normal’ year. This is the longest drought in a thousand years (Zyri 2022 ; UN, 2022 ). Competition over water may worsen and degrade ecosystems putting 31 million people in water stress in South America (Castellanos et al., 2022 ). Falling rain levels by 20–40% since 2010 and atrophying glaciers and aquifers have made Chile a top country facing water stress (World Resources Institute, 2015 ).
The 1981 Pinochet coup ushered in a Constitution that privatized water, granting perpetual property rights allowing powerful mining, energy and export agriculture interests to usurp community drinking water and traditional local water practices (Hurlbert, 2018 ). It promoted an export economy of large scale irrigated agri-business producing high-value crops like fruits, vegetables and grapes (Reyes, 2009 ) advancing a narrative of user pay and full water cost at the expense of human rights to water (Larrain, 2014 ). Agriculture now uses 72% of water followed by drinking water (12%), industrial consumption (7%), hydroelectric/grazing (5%) and mining (4%) (Ramirez, 2022 ). Footnote 1 Export agriculture has meant wealth for some in Chile. In 2021, Chile’s real GDP was $25,400 per capita and the Gini index score of 44.9 situates Chile as a leading South American country (CIA 2023).
And yet, 8% of the population don’t have access to water to fulfil their human rights Langrand et al. ( 2022 ) and rural communities compete with large companies for water and are hit the worst. While a single avocado exported to North American and European supermarkets takes 320 L of water, some people only receive 15–20 L per day (flushing the toilet takes 10 L) (Langrand et al., 2022 ).
Chilean water governance is dominated by its privatized market water interests (Hurlbert & Diaz, 2013 ) but attempts to protect vulnerable people and the ecosystem have occurred (including protecting ecological flows and a levy for unused water rights to prevent hoarding)(Hurlbert, 2018 ). However, such attempts have little impact on prior constitutionally protected water owners (Hurlbert, 2018 ). In times of drought (defined as a river flowing at less than 70% of average) the Chilean Water Code (Article 314) allows irrigators to request a Presidential Declaration of Drought Zones. Upon Declaration, proportional reduction of water to each rights holder in turns is employed for a maximum of six months (Hurlbert, 2018 ).
After the Chilean plebiscite to return to democracy in 1988, the government severed links with social movements for fear of social unrest returning Chile to an autocratic state (Somma, 2017 ). However, early this Century, discontent with markets and political elites resulted in student protests (against expensive higher education), environmental protests (against externalities of forestry, energy and mining companies), and Indigenous protests (such as the Mapuche against the impacts of development on their lifestyles and environment) (Somma, 2017 ). Recently, the number of protests and participants has increased steeply (Larsson, 2019 ).
3.1.2 The window of opportunity
In 2019 a million protesters demanded President Pinera’s resignation (Larsson, 2019 ) and a new constitution (McGowan, 2019 ). Protests were linked to the rise in metro fees. Footnote 2 Other reasons included lack of education, poor public health care, and crippling inequality experienced through increasing costs of living, low wages and pensions. Chile embarked on drafting a new constitution after President Gabriel Boric defeated conservative Jose Antonio Kast in the 2021 election.
Since political exclusion fuelled the protests, Chile’s constitutional convention (2021–2022) included nationwide deliberative meetings, local town hall meetings, self-convened meetings by citizens, consultation with Indigenous peoples, and a digital public participation platform. Further, public hearings received hundreds of expert and citizen submissions. Public constituent hearings also occurred with people in the different Chilean constituents. 2486 citizen initiatives were supported by 220,000 people with ten gaining enough support to be discussed by the Convention including issues of education, religious freedom, animal rights, and nationalization of mining companies (Fuentes, 2022 ).
In September 2022, Chile’s constitutional assembly finalized a new Constitution of 388 articles. It replaced the Senate with a ‘Chamber of Regions’, decentralized taxing powers to regions, provided social services (healthcare, housing, education), and switched water and resource rights to temporary revocable permits (Burns, 2022 ). It defined Chile as a ‘pluri-national’ state including the customary law of Indigenous people and declaring water rights ‘ incomerciables ’ or ‘unsalable.’ These provisions were however unclear (ibid.) and the constitution was rejected (Surma, 2022 ). Reasons cited include fake news orchestrated by well-organized negative campaigns (Fuentes, 2022 ), mandatory voting of all citizens (while many had not participated) (People Powered, 2022 ), early term poor performance of Boric’s government and its failure to tackle rising crime and terrorism concerns, too much change from the 1981 Constitution, inflation, and a sluggish economy (Rodriguez, 2022 ). Instead of uniting people, the rejection of the new constitution possibly reflected a rejection of the process, as the elected representatives of the Constituent Convention were delegitimized having lost citizen trust in their ability to guarantee an adequate framework. The constitutional failure was also seen as a rejection of President Boric’s performance (Edelman Gobal Advisory 2022). Since then, a new constitutional writing plan commenced. Drafters included 50 members of an elected Constitutional Council; 24 experts and 14 jurists formed the ‘Admissibility Technical Commission’ and acted as arbitrator (Nodal, 2022 ). This newest constitutional endeavor also failed with 56% of the electorate voting against it in December 2023 (Villegas, 2023 ).
Meanwhile, a new water code has been passed which prioritizes water for human consumption and allows government to temporarily suspend usage rights on threatened watercourses (Langrand, 2022 ; Ramirez, 2022 ). Water permits will be granted under a 30-year renewable concession (or less) based on water availability or Aquifer sustainability; unused water permits can be revoked (Ramirez, 2022 ). Registration of water rights is mandatory (only 4% are presently registered). This code excludes the 90% of water rights already granted (Langrand, 2022 ). As a result, uncertainty surrounding water shares continues within Chile (Ramirez, 2022 ).
3.1.3 Ecuador
Glacier loss, precipitation variability and land use changes have impacted livelihoods and water resources (Castellanos et al., 2022 ). ENSO causes heavy rains, storms, floods, landslides and increasing heat waves and consecutive dry days; this trend may increase in the future (ibid.). With natural assets including the Galapagos and Amazon, Ecuador has led the world on equity and sustainability in its laws and policies, (but suffers economic and functional challenges in implementation) (Wingfield et al., 2021 ). Ecuador’s per-capita GDP is $10,700 (less than half of Chile’s) and its Gini Index is 47.3 (more unequal than Chile) (CIA 2023); per capita water availability is three times the international average (Instituto Geografico Militar 2013 ). While 60.3% of rural people use safely managed sanitation, only 31.2% of urban people do (UN, 2023 ). While 74.7% of urban people use safely managed drinking water, only 52.8% of rural people do (ibid.). Poor technical and infrastructure capacity challenges water management; moreover, decentralized drinking water and irrigation management conflicts with the national responsibility for water control and management (Wingfield et al., 2021 ). Ecuador has a decentralized administration of 24 provinces (van den Berg & Danilenko, 2019 ).
Pre-1960, water privatization was allowed with water viewed as a commodity rather than a public good (Martínez-Moscoso et al., 2018 ). Between 1970 and 1990 Ecuador’s water laws advanced decentralized and privatized state resources (Cremers et al., 2005 ), but water was declared a public good in the early 1990s effectively ending privatization (Martínez-Moscoso et al. 2019 ). But privatization again emerged with new public management in the 1998 Constitution. The state’s role was minimized and private irrigation management prioritized (Law of Decentralization and Irrigation Management Transfer programmes; Hoogesteger et al. 2013). This process was aided by the development of oil exports and the predominant influence of these companies (Shade, 2015 ; Mena-Vásconez 2017 ) and Chinese investment (Ray and Chimienti 2017 ). An export economy reliant on water-intensive floriculture production (roses) has developed (Damonte, 2019 ), paying one quarter of the water rate of community users (Hidalgo et al., 2017 ). Further, the principle of buen vivir has successfully been argued in court to protect the mining livelihood of small scale gold miners. These successes have resulted in environmental protestors of mining expansion being prosecuted criminally. As a result, the argument of buen vivir has protected a mining livelihood at the expense of the environment (Valladares & Boelens, 2019 ).
The window of opportunity.
In the early 2000s a window of opportunity opened when people protested privatization and neoliberal reform. Since the 1980s, Indigenous and environmental organizations opposed the exploitation of oil, water, and precious metals protesting pollution, deforestation and the use of genetically modified organisms. Rural people fought against privatization of oil, electricity and telecommunications in the 2000s and momentum grew (Dosh and Kilgerman 2009 ). In 2007, thousands of people lobbied for a new constitution to be drafted by the Constituent Assembly and its 1,230 delegates. The draft document had 444 articles.
This draft constitution moved away from privatization (Asamblea Nacional, 2014 ). Water was declared a human right in 2008 (Asamblea Nacional Constituyente 2008). It recognized the rights of ‘Pachamama’ or Mother Earth. It incorporated sumac kawsay harmonizing human development and environment protection by recognizing the innate rights of nature and buen vivir to improve living conditions (Kauffman et al. 2014 , Tanasescu, 2013 ). The window of opportunity partly arose due to the resistance to neoliberal privatization policies (Hoogesteger, 2012 ). Over 60% of voters backed President Correa’s new constitution; Correa was elected to fight long standing corruption, ban foreign military bases, allow same sex marriage, and greater national control over oil and mining industries (Britannica, 2023 ). This was a “moment of unity between Ecuador’s popular movements and the electoral left” (Dosh & Kligerman, 2009 : n.p.).
Popular movements clarified that their support for the Constitution in 2008 wasn’t support for the President (Dosh & Kligerman, 2009 ). Subsequent clashes over mining through 2008–2009 demonstrated that these groups had different interests (ibid.) and effecting the constitutional change in relation to water did not happen immediately. In fact, the Constitution allowed an exception to enable privatizing natural resources and water, allowing the president to give permission to extract resources. This was dubbed by the former government communications secretary as “one of the biggest deceptions of the Constitution” (ibid.). The deceptive rules allowing Presidential exceptions were incongruent with the minga model granting access to community members due to their work rather than a payment (Hoogesteger, 2012 ), a practice that informs local community water management to this day (Hoogesteger, 2013 , Wingfield 2021 ).
Widespread demonstrations after 2008 protested a new mining law to allow Canadian mining corporations to begin operations (Dosh and Kilgerman 2009). On the day of the Mining Law’s passage, 4,000 Indigenous people blockaded a highway in the south and tens of thousands mobilized in Quito, Cuenca, the Amazon and on the coast (Zibechi, 2009 ). The President of Acción Ecológica in 2009 argued that the state would not be able to protect natural resources and that the President had ‘politicized’ the problem by stating that his principal enemy was ecologists (Dosh and Kilgerman 2009 ). Other protests included the Caminata del Agua movement of 2014 and those led by Carlos Perez Guartambel ( Yaku ) protesting mining activities near water resources (Kolirin, 2020 ). These protests centered on water, but also larger protests occurred on entry requirements impeding hundreds of thousands of students attending university, labour unions and teachers against anti-union prohibitions, indefinite re-election laws for the President, and against the continuous criminalization of social protest (Picq 2014). These local demonstrations garnered some success in the courts including prevention of expansion of an access road that would have increased contamination risks to the Vilcabamba River in 2011 (Dupuits et al., 2020 ).
In 2014 water was declared a national strategic asset for public use and privatization effectively outlawed (Asemblea Nacional 2014 ). Local community or individual water management is allowed pursuant to this law in the event of finance and construction of the main water infrastructure (Asemblea Nacional 2014 ). Municipal governments must provide potable water, and sewage and wastewater treatment and are forbidden from suspending these services (Art 264(4); 326(15) Asemblea Nacional 2008). However, this is subject to the Water Secretary’s authority and national regulative body that prioritizes use as human consumption first, irrigation that guarantees food sovereignty, ecological flow, and lastly productive activities. This has reduced the role of private companies in water management.
Ecuadorian courts have embraced the constitutional water laws prioritizing them over mining and development. They have implemented the rights of nature laws in a ruling in favour of mangroves and also Los Cedros protected area’s right to flourish (thereby stymying mining activities). The court recognized the inherent value of nature that must be recognized in and of itself without consideration of ‘usefulness’ for people (Surma, 2021 ). Further, a September 2020 ruling of the constitutional court halted mining activity in the Cuenca region (Primicias, 2020 ). While constitutional change occurred in 2008, its consolidation in Ecuadorian law and practice was realized in the ensuing years.
3.2 Analysis
3.2.1 policy problem framing.
Where there is agreement on science and values, there is no need to politicize an issue as single loop learning is adequate. Prior to Ecuador’s constitutional reform, water was managed in a privatized, decentralized technocratic manner advancing irrigation interests. Chile had administered its water resource within quadrant two of the Split Ladder of Participation where water rights are private property interests protected within legal institutions in a technocratic manner. Both case study countries’ windows of opportunity arose through a combination of policy problem framing and participatory contestation or politicization. These case studies demonstrate that the window of opportunity for significant change involved complex multi-faceted political problems.
Table 1 displays the policy problem framing in Chile and Ecuador within the text of the constitutional amendment and the resulting constitutional changes (effected in Ecuador and defeated in Chile). While Chile’s predominant framing was in relation to addressing social inequality and the high cost of living, Ecuador’s centered on advancing a liberal agenda, good governance (anti-corruption), and national control of oil and mining. Overturning water privatization was not the predominant problem framing for Ecuador.
As we (Hurlbert & Gupta, 2015 ) originally concluded, exploration, discussion and participation in solving complex problems results in the creation of policy sub-problems, the combination of which may address the complex problem. The Chilean constitutional renewal was laudable, but it proved to be an insurmountable task. Where enduring patriarchical institutions, widening social inequality, looming climate change impacts of drought and fire were ravaging the Chilean landscape, remedial hopes with one participatory constitutional engagement were laudable, but unrealistic (The Economist, 2022 ). The Ecuadorian ‘problem’ included foreign exploitation of oil and mining effectively addressing inherent contradictions of sustainable ‘development’ and the environment (Reid, 2023 ); this problem framing was missing in Chile.
3.2.2 Policies and actors
In both countries the window of opportunity also arose due to the election of a new President with a new political agenda; each embarked on renewing the constitution embracing a quadrant four politicization. For both countries politicization was needed, but in Chile, as is often the case, the problem was not solved in the short term (Smyth et al., 2021 ). In Chile, the complex water problem arose due to both the omnipresence of climate change (and the mega drought) and the widespread malaise surrounding Chile’s constitutionalized private water market.
If only symbolic participation is advanced, and there is consensus on either science, or values, but not both, politicization will lead to non-decisions and reproduction of injustices. In Chile, the consensus on mega drought science is irrefutable, but the symbolic participation in the Constitutional amendment foreshadowed its failure (People Powered, 2022 ). Although the scope and ambit of the constitutional renewal process was good, COVID reduced participation. Hence, Chile’s endemic social problems are jettisoned back to a problem of mega drought adaptation science. Here zero loop learning plays out as historic processes continue to be employed in water reductions, perpetuating Chilean water injustice (lack of poor people’s access to water), and without addressing the root problem. Constitutional protection of a human right to water is missing.
The Ecuador case study reflects successful policy solutions and social learning where complex problems were reduced to broad constitutional reform principles (see Table 1 ). Ecuador’s 2008 Constitutional amendments advanced Nature’s rights, showing how complex problems are reduced to lesser sub problems, and addressed in a productive manner moving into quadrant three increasing citizen power. While consensus on water and development issues was not immediately achieved with the constitutional reform, citizens obtained their human rights to water and the creation of Nature’s rights to advance consensus through legal remedies. The Ecuadorian case importantly illustrates that mere Constitutional textual reform, while it appears as significant ‘change,’ may not result in actual change. Policy change should be carefully defined as ‘radical’ change where overarching terms of policy discourse associated with paradigmatic shift occur and a wholesale change in ‘ideas’ and social interests (Hall, 1993 ).
Engagement in complex politicized problems in quadrant four is no easy task; meaningful involvement of social scientists is paramount and in respect of restoring freshwater ecosystem services in the context of local and global change, policy change, paradigm shift and significant social learning may not be feasible in the short term (Smyth et al., 2021 ). The Chilean case illustrates the tension of requiring a high level of value consensus for constitutional change to protect the vulnerable. While the Ecuador case contained value consensus of protecting national interests in oil and mining and pushing back on privatization of water, the Chilean case did not. While the Ecuador case involved consensus of actors for the constitutional solution (but not necessarily their endorsement of the President), the Chilean case could not achieve this.
These two case studies do not necessarily support the conclusion that the Ecuadorian value against privatized water must exist for triple loop learning and water law reform. In Sharma and Kumar ( 2020 ) the Split Ladder analysis of water, energy and food confirmed a two-step process for consumers and producers whereby the market dictated the first step in the process of decision making for water access and allocation, but then the triple rights of people to water, energy and food determined the second step in the allocation and access decision making distributing these assets. It may be that in Chile, such a two-step process is more fitting and palatable.
Procedural justice and power in politicization are fundamental considerations. Holistic power analysis that advance understanding of contextual factors that favour stakeholder participation increase success (Wood et al., 2016 ). However, politicization of issues may exclude the interests of the minority, including Indigenous peoples. Addressing these concerns may not occur without successful Constitutional amendment to protect minority rights. Chile’s Water Code amendments are a start, but lack the power of constitutional status protecting recognized Chilean rights. Continued politicization of Indigenous and water rights and participation of people in decision making through all avenues, including legal ones are required. In the Ecuador case study the 2008 and 2014 constitutional reforms and subsequent legal actions illustrate this point. In Ecuador Indigenous people continue to oppose Presidential decrees to increase oil production and pipelines in their lands and advance their constitutional rights including the requirement for their consent prior to development initiatives (Waorani Pastaza Organization vs. Ecuador 2019; A’I Kofan community of Sinangoe vs. Ecuador 2022).
Policy windows are essential for double or triple loop learning. The multiple streams approach has primarily been applied to analyze a policy change after the fact. Thus, policy windows are often viewed as an opportunity rather than intentionally created. Hence, while literature has documented strategies of policy entrepreneurs to advance policy change and prepare for a policy window (Brouwer & Biermann, 2011 ), there is scant literature documenting methods that have intentionally and successfully created policy windows (Hermansen, 2015 ). While Chile’s new Constitutional Council (commencing in 2023) will have a window of opportunity to make significant change through double or triple loop learning, its success will depend on its policy entrepreneurs (actors) and their ability to set a water policy agenda. The Split Ladder of Participation provides a framework to analyze complex policy problems and prospectively set agendas for participation advancing their resolution.
4 Conclusion
This article interrogates significant policy change and public participation in relation to constitutional change. Politicization doesn’t always lead to problem solving, but it can open a window of opportunity for change and be important for a healthy resilient democracy. This paper addresses the question: Under what circumstances should problems be politicized, and what is the effect of such politicization? It builds on the split ladder of participation to develop a theory on politicization of complex societal problems.
This paper explores people’s participation in solving complex policy problems through problem framing and windows of opportunity. While responding to complex problems through public engagement and politicization is often touted as optimal, this paper explores how problem solving is best achieved in relation to significant policy change – specifically constitutional reform. Two case studies provide illustration: the successful 2008 constitutional reform of Ecuador and the unsuccessful 2022 Chile attempt at constitutional reform. This paper argues for a holistic exploration of a complex problem such as water governance, which is often situated in relation to overarching policy problems of development and inequality. Policy entrepreneurs are well advised to continue to advance needed reforms creating and seizing the moment afforded by windows of opportunity; our conclusion is that politicization is required for significant policy change and agenda setting, and recommended.
When there is agreement on science and policy, quadrant two suffices and politicization is not needed. Policy systems are advanced enough to repair and modify instruments to address problems. Where there is no agreement on either science or policy, politicization may be needed to address lack of consensus in values (Islam & Susskind, 2018 ), but cannot be sufficient. Here constitutional protection is needed to protect minorities and the vulnerable and avoid the reproduction of injustices. Inadequate politicization (and accompanying participation of people and civil society as in the Chilean case) can lead to zero order learning and the reproduction of injustices. In turn policy windows can close with growing distrust. Participation in water decisions is most importantly informed by ecological and social inclusion through considerations of human dignity and equality, rather than legal and economic considerations (Pouw & Gupta, 2017 ).
Stakeholder participation and politicization do not guarantee that minority rights, or rights of nature will be protected. Such protection needs to be guaranteed by constitutions at the national and global level. Politicization and constitutional discussions are also preconditions for addressing the increasing interconnections of water scarcity, drought, and groundwater between states and normative principles of equitable and reasonable use and participation within Article 5 of the United Nations Watercourses Convention. The 2010 recognition of the human right to water and sanitation by the UN General Assembly (UN, 2010 ) enabled human rights claims as a legal strategy to advance climate adaptation and mitigation efforts; courts are becoming increasingly receptive (Peel & Osofsky, 2015 ). Such claims can be anchored in the Warsaw International Mechanism under the climate change regime or before the United Nations Human Rights Council and the Office of the High Commissioner for Human Rights. However, such claims are not assured, given the advancement of water futures trading on Wall Street: since 2020 investors can hedge against or for the potential of water scarcity effectively transforming citizens into clients (Fox, 2020 ).
While national constitutional protection is easier than global protection, the Ecuador case demonstrates that constant vigilance through participation, including in the legal system is still required. And perhaps, advancing constitutional change to align a nation’s law with international legal obligations would increase the success of constitutional water initiatives. Although constitutional reform can promotedoctrinal legal change, it is not until behavioural assumptions and social relations change, that a paradigmatic change has occurred (Hall, 1993 ; Daigneault, 2014 ). Policy change is not only required, but also demonstrated change in values, conceptions of what the problem actually is, ideas about which policy ends to pursue and appropriate policy means to achieve those ends (Daigneault, 2014 ) all of which may take time. As we are moving into the world of increasingly unstructured problems, we need overall values that both bind us and empower us to live in a safe and just world. And we need statesmanship; these cases demonstrate the importance of new political leaders.
The limitations of this research are that it is contextualized, case study research. More case studies, with different policy problems, different levels of study (international, sub-national etc.), and geographies need to consider these issues and depoliticization in the context of the Split Ladder, or policy change and citizen engagement. While deep insights are provided in this comparative case study, more studies exploring these phenomena would advance our understanding of when politicization is needed and what are the effects of politicization.
A counter narrative is provided by over 1900 rural water cooperatives, many existing since 1964, often headed by women that provide drinking water for nearly two million rural inhabitants (Langrand et al., 2022 ).
Students, however, had been protesting over the past decade (Larsson, 2019 ) over high tuition.
Abbreviations
Measure of inequality proposed by Corrado Gini
Socio-ecological systems
United Nations
A’I Kofan community of Sinangoe vs. Ecuador, (2022).
Asamblea Nacional Constituyente (Constitución Ecuatoriana del 2008). República del Ecuador: Montecristi, Ecuador, 2008.
Asamblea Nacional. (2014). Ley Orgánica De Recursos Hídricos, Usos, Y Aprovechamiento Del Agua; República Del Ecuador . Quito.
Bartlett, L., & Vavrus, F. (2017). Rethinking case study research. A comparative approach . Routledge.
Basco-Carrera, L., van Beek, E., Jonoski, A., Benitez Avila, C. A., & Guntoro, F. P. (2017). Collaborative Modelling for Informed Decision Making and Inclusive Water Development. Water Resources Management , 31 (9), 2611–2625. https://doi.org/10.1007/s11269-017-1647-0 .
Article Google Scholar
Behnassi, M., Pollmann, O., & Gupta, H. (2019). Climate Change, Food Security and Natural Resource Management Regional Case Studies from Three Continents (1st ed. 2019. ed.): Cham: Springer International Publishing: Imprint: Springer.
Bosch, S., Rathmann, J., & Schwarz, L. (2019). The Energy transition between profitability, participation and acceptance – considering the interests of project developers, residents, and environmentalists. Advances in Geosciences , 49 , 19–29. https://doi.org/10.5194/adgeo-49-19-2019 .
Brian, C. C., & Hannah, G. (2017). Beyond mandatory fishways: Federal Hydropower Relicensing as a window of opportunity for dam removal and adaptive governance of Riverine landscapes in the United States. Water Alternatives , 10 (3), 819–839.
Google Scholar
Britannica (2023). Ecuador from the late 20th century. Encyclopedia Britannica, Inc. https://www.britannica.com/place/Ecuador/Ecuador-from-the-late-20th-century .
Brouwer, S., & Biermann, F. (2011). Towards Adaptive Management: Examining the Strategies of Policy Entrepreneurs in Dutch Water Management. Ecology and Society , 16 (4), 5–20.
Burns, N. (2022). Chile’s Proposed Constitution: 7 Key Points. https://www.americasquarterly.org/article/chiles-proposed-constitution-7-key-points/ .
Cairney, P., & Jones, M. D. (2016). Kingdon’s multiple streams Approach: What is the empirical impact of this Universal Theory? Kingdon’s multiple streams Approach. Policy Studies Journal , 44 (1), 37–58. https://doi.org/10.1111/psj.12111 .
Cairney, P., & Oliver, K. (2017). Evidence-based policymaking is not like evidence-based medicine, so how far should you go to bridge the divide between evidence and policy? Health Research Policy and Systems , 15 (1), 35. https://doi.org/10.1186/s12961-017-0192-x .
Campbell, J. L. (2004). Institutional change and globalization . Princeton, N.J.: Princeton University Press.
Castellanos, E., Lemos, M. F., Astigarraga, L., Chacón, N., Cuvi, N., Huggel, C., Miranda, L., Moncassim Vale, M., Ometto, J. P., Peri, P. L., Postigo, J. C., Ramajo, L., Roco, L., & Rusticucci, M. (2022). Central and South America. In O. Pörtner, D. C. Roberts, M. Tignor, E. S. Poloczanska, K. Mintenbeck, A. Alegría, M. Craig, S. Langsdorf, S. Löschke, V. Möller, A. Okem, & B. Rama (Eds.), Climate Change 2022: Impacts, adaptation, and vulnerability. Contribution of Working Group II to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change [H (pp. 1689–1816). Cambridge University Press. https://doi.org/10.1017/9781009325844.014 .
Catney, P., & Henneberry, J. M. (2016). Public entrepreneurship and the politics of regeneration in multi-level governance. Environment and Planning C: Government and Policy , 34 (7), 1324–1343. https://doi.org/10.1177/0263774X15613357 .
Cohen, M. D., March, J. G., & Olsen, J. P. (1972). A Garbage can Model of Organizational Choice. Administrative Science Quarterly , 17 (1), 1–25. https://doi.org/10.2307/2392088 .
Conallin, J., Wilson, E., & Campbell, J. (2017). Implementation of Environmental flows for Intermittent River systems: Adaptive management and stakeholder participation facilitate implementation. Environmental Management (New York) , 61 (3), 497–505. https://doi.org/10.1007/s00267-017-0922-4 .
Cremers, L., Ooijevaar, M., & Boelens, R. (2005). Institutional reform in the Andean irrigation sector: Enabling policies for strengthening local rights and water management. Nat Resour Forum , 29 , 37–50.
Cuadrado-Quesada, G., & Gupta, J. (2019). Participation in groundwater governance – outlining a path to inclusive development. Water Policy , 21 , 1050–1064.
C.I.A. (2023). World Factbook. https://www.cia.gov/the-world-factbook/field/gini-index-coefficient-distribution-of-family-income/country-comparison/ .
Daigneault, P. M. (2014). Reassessing the Concept of Policy paradigm: Aligning Ontology and Methodology in Policy studies. Journal of European Public Policy , 21 (3), 453–469.
Damonte, G. H. (2019). The constitution of hydrosocial power: Agribusiness and water scarcity in Ica. Peru Ecol Soc , 24 , 221.
Dosh, P., & Kligerman, N. (2009). Correa vs. Social Movements: Showdown in Ecuador. Available at.
Dubois, J., & Saunders, K. (2017). Explaining the resurgence of Métis rights: Making the most of windows of opportunity. Canadian Public Administration , 60 (1), 48–67. https://doi.org/10.1111/capa.12196 .
Dunlop, L., & Rushton, E. A. C. (2022). Putting climate change at the heart of education: Is England’s strategy a placebo for policy? British Educational Research Journal , 1–19. https://doi.org/10.1002/berj.3816 .
Dunlop, L., Atkinson, L., & Turkenburg-van Diepen, M. (2021). It’s our future. Youth and fracking justice in England. LOCAL ENVIRONMENT , 26 (1), 110–130. https://doi.org/10.1080/13549839.2020.1867837 .
Dupuits, E., Baud, M., Boelens, R., de Castro, F., & Hogenboom, B. (2020). Scaling up but losing out? Water commons’ dilemmas between transnational movements and grassroots struggles in Latin America. Ecological Economics , 172 , 6625.
Edelman Global Advisory (2022). The Advisory Chilean citizens vote to reject the new Constitution. September 5, 2022. https://www.edelmanglobaladvisory.com/insights/Chilean-citizens-vote-to-reject-the-new-Constitution .
Fischer, F. (2003). Reframing Public Policy: Discursive politics and deliberative practices . Oxford: Oxford University Press.
Folke, C., Hahn, T., Olsson, P., & Norberg, J. (2005). ADAPTIVE GOVERNANCE OF SOCIAL-ECOLOGICAL SYSTEMS. Annual Review of Environment and Resources , 30 (1), 441–473. https://doi.org/10.1146/annurev.energy.30.050504.144511 .
Fotiadou (Ed.). Routledge Handbook of Comparative Constitutional Change. 1 edn.
Fox, M. (2020). Water futures set to join likes of gold and oil and trade on Wall Street for first time ever. Markets Insider. December 7, 2020. https://markets.businessinsider.com/news/stocks/water-futures-to-trade-on-wall-street-first-time-ever-2020-12-1029870836?miRedirects=1 .
Fuentes, C. (2022). Citizens’ Participation at the Chilean Constitutional Convention: Balancing Expectations and Efficiency. Constitutionnet. Supporting Constitution Builders Globally. January 25, 2022. https://constitutionnet.org/news/citizens-participation-chilean-constitutional-convention-balancing-expectations-and-efficiency .
Hajer, M. A. (2005). Setting the stage: A dramaturgy of policy deliberation. Administration & Society , 36 (6), 624–647. https://doi.org/10.1177/0095399704270586 .
Hall, P. A. (1993). Policy paradigms, social learning and the state: The case of economic policymaking in Britain. Comparative Politics , 25 (3), 275–296.
Harvey, B., Cochrane, L., & Van Epp, M. (2019). Charting knowledge co-production pathways in climate and development. Environmental Policy and Governance , 29 (2), 107–117. https://doi.org/10.1002/eet.1834 .
Hermansen, E. A. T. (2015). Policy window entrepreneurship: The backstage of the world’s largest REDD + initiative. Environmental Politics , 24 (6), 932–950. https://doi.org/10.1080/09644016.2015.1063887 .
Hidalgo, J. P., Boelens, R., & Vos, J. (2017). De-colonizing water. Dispossession, water insecurity, and indigenous claims for resources, authority, and territory. Water Hist , 9 , 67–85.
Hoogesteger, J. (2012). Democratizing water governance from the grassroots: The development of interjuntas-chimborazo in the Ecuadorian Andes. Hum Organ , 71 , 76–86.
Hoogesteger, J. (2013). Social capital in water user organizations of the Ecuadorian highlands. Hum Organ , 72 , 347–357.
Hurlbert, M. (2018). Adaptive Governance of Disaster Drought and Flood in Rural Areas (1st ed. 2018. ed.): Cham: Springer International Publishing: Imprint: Springer.
Hurlbert, M., & Diaz, H. (2013). Water Governance in Chile and Canada: A comparison of adaptive characteristics. Ecology and Society , 18 (4), art61. https://doi.org/10.5751/ES-06148-180461 .
Hurlbert, M., & Gupta, J. (2015). The split ladder of participation: A diagnostic, strategic, and evaluation tool to assess when participation is necessary. Environmental Science & Policy , 50 , 100–113. https://doi.org/10.1016/j.envsci.2015.01.011 .
Hurlbert, M., Gupta, J., & Verrest, H. (2019). A comparison of drought instruments and livelihood capitals: Combining livelihood and institutional analyses to Study Drought Policy instruments. Climate and Development , 11 (10), 863–872. https://doi.org/10.1080/17565529.2019.1585318 .
Husa, J. (2020). Comparative methodology and constitutional change . In X Contiades & A.
Instituto Geográfico Militar (IGM). (2013). Atlas Geográfico De La República Del Ecuador . Quito, Ecuador.
Islam, S., & Susskind, L. (2018). Using complexity science and negotiation theory to resolve boundary-crossing water issues. JOURNAL OF HYDROLOGY , 562 , 589–598. https://doi.org/10.1016/j.jhydrol.2018.04.020 .
Jensen, J. L., & Rodgers, R. (2001). Cumulating the Intellectual Gold of Case Study Research. Public Administration Review , 61 (2), 235–246. https://doi.org/10.1111/0033-3352.00025 .
Jurgilevich, A., Rasanen, A., & Juhola, S. (2021). Assessing the dynamics of urban vulnerability to climate change: Case of Helsinki, Finland. ENVIRONMENTAL SCIENCE & POLICY , 125 , 32–43. https://doi.org/10.1016/j.envsci.2021.08.002 .
Kauffman, C. M., & Martin, P. L. (2014). Scaling up Buen Vivir: Globalizing local environmental governance from Ecuador. Global Environ Politics , 14 , 40–58.
Kingdon, J. W. (2011). Agendas, Alternatives, and Public Policies, 1976, 1977, 1978, 1979 [United States]. In (2011-03-18. ed.). Ann Arbor, Mich: Ann Arbor, Mich. Inter-university Consortium for Political and Social Research distributor.
Kinnunen, M. (2021). Weak congruence between public opinion and policy outcome in energy and climate policy—Is there something wrong with Finnish democracy? ENERGY RESEARCH & SOCIAL SCIENCE , 79 . https://doi.org/10.1016/j.erss.2021.102014 .
Kolirin, L. (2020). The Trees are my Grandparents: The Ecuador Tribe Trying to Save Its Culture. The Guardian. 16 April 2020, pp. 5–8. Available online: https://www.theguardian.com/world/2020/apr/16/the-trees-are-my-grandparents-the-ecuador-tribe-tryingto .
Langrand, M. (2022). Part II: women lead community-run efforts to tackle Chile’s water crisis. Geneva Solutions. The Water We Share No 02. https://genevasolutions.news/explorations/the-water-we-share/part-ii-women-lead-community-run-efforts-to-tackle-chile-s-water-crisis .
Langrand, M., Jefford, K., & Cook, P. (2022). The water we share. Geneva Solutions. https://genevasolutions.news/explorations/the-water-we-share .
Larrain, S. (2014). Presentation as Directora Progama Chile Sustentable to Seminario Internacional, Governanza Del Aqua: Desde lo global a lo local . Universidad Catolica de Chile.
Larsson, M. (2019). Chile protests: More than one million bring Santiago to a halt. Aljazeera. October 26, 2019. https://www.aljazeera.com/economy/2019/10/26/chile-protests-more-than-one-million-bring-santiago-to-a-halt/ .
M Li, T. (2007). The Will to improve: Governmentality, Development, and the practice of politics. Duke University Press , Duke (NC), USA–2007.
Martínez-Moscoso, A., & Larson, R. (2019). Forestry management and water law: Comparing Ecuador and Arizona. Water International , 44 , 337–353.
Martínez-Moscoso, A., Feijó, V. G. A., & Silva, T. V. (2018). The vital minimum amount of drinking water required in Ecuador. Resources , 7 , 15.
McGowan, C. (2019). Chile protests: What prompted the unrest? Aljazeera, October 30, 2019. https://www.aljazeera.com/news/2019/10/30/chile-protests-what-prompted-the-unrest?traffic_source=KeepReading .
Mena-Vásconez, P., Vincent, L., Vos, J., & Boelens, R. (2017). Fighting over water values: Diverse framings of flower and food production with communal irrigation in the Ecuadorian Andes. Water International , 42 , 443–461.
Mirumachi, N., & Hurlbert, M. (2022). Reflecting on twenty years of international agreements concerning water governance: Insights and key learning. International Environmental Agreements Law and Politics . https://doi.org/10.1007/s10784-022-09564-9 .
Morf, A., Kull, M., Piwowarczyk, J., & Gee, K. (2019). In J. Zaucha, & K. Gee (Eds.), Towards a ladder of Marine/Maritime spatial planning participation (1 ed., Vol. 1). Palgrave MacMillan.
Nodal (2022). Avanza reforma que habilita proceso constituyent: Comision de Constitutcion del Sanado aprueba en general y abra plazo para indicaciones. Noticias de. America Latina y El Caribe. December 26, 2022. https://www.nodal.am/2022/12/chile-la-comision-de-constitucion-del-senado-aprobo-en-general-la-reforma-constitucional-que-surgio-tras-el-acuerdo-por-chile/ .
O.E.C.D. (2008). Glossary of Statistical Terms. https://doi.org/10.1787/9789264055087-en https://www.oecd-ilibrary.org/economics/oecd-glossary-of-statistical-terms_9789264055087-en .
Panten, K., van Heel, B. F., Fliervoet, J. M., & van den Born, R. J. G. (2018). Cross-border collaboration in River Management: Views on participation in a dutch-german case study. Water Resources Management , 32 (12), 4063–4078. https://doi.org/10.1007/s11269-018-2039-9 .
Parreira do Amaral, M. (2022). Comparative Case Studies: Methodological Discussion. In Benasso, S., Bouillet, D., Neves, T., Parreira do Amaral, M. (Eds.) Landscapes of Lifelong Learning Policies across Europe. Palgrave Studies in Adult Education and Lifelong Learning. Palgrave Macmillan, Chamn. 41–60. https://doi.org/10.1007/978-3-030-96454-2_3 .
Pearson, L. J., & Dare, M. (2019). Framing up the stretching of Co-management. Society & Natural Resources , 32 (4), 363–381. https://doi.org/10.1080/08941920.2018.1544677 .
Peel, J., & Osofsky, H. M. (2015). Climate change litigation: Regulatory pathways to cleaner energy . Cambridge University Press.
People Powered (2022). Report from Chile: Why the new constitution was rejected and what we can learn. Global Hub for Participatory Democracy. https://www.peoplepowered.org/news-content/why-chile-constitution-rejected .
Potting, J., Thomas, J-B., & Grondahl, F. (2022). Stakeholder participation in sustainability assessment of non-wicked problems: The case of a future seaweed industry in Sweden. Ambio , 51 , 901–913.
Pouw, N., & Gupta, J. (2017). Inclusive development: A multi-disciplinary approach. CURRENT OPINION IN ENVIRONMENTAL SUSTAINABILITY , 24 , 104–108. https://doi.org/10.1016/j.cosust.2016.11.013 .
Primicias (2020). Corte Constitucional da Paso a Consulta Minera en Cuenca; Primicias: Quito, Ecuador.
Prutzer, M., Morf, A., & Nolbrant, P. (2021). Social Learning: Methods Matter but Facilitation and supportive context are key – insights from Water Governance in Sweden. Water , 13 , 2335. https://doi.org/10.3390/w13172335 .
Ramirez, N. (2022). Modernization of Chile’s Water Code. Report Number CI2022-0002, https://apps.fas.usda.gov/newgainapi/api/Report/DownloadReportByFileName?fileName=Modernization%20of%20Chile%27s%20Water%20Code_Santiago_Chile_01-18-2022.pdf .
Ray, R., & Chimienti, A. A. (2017). A Line in the Equatorial Forests: Chinese investment and the environmental and social impacts of extractive industries in Ecuador. In China and Sustainable Development in Latin America ; Ray, R., Gallagher, K., López, A., Sanborn, C., Eds.; Anthem Press: London, UK, pp. 1?51.
Reid, E. (2023). The shape of Environment rights Opportunity structures for the Anthropocene Chap. 9 in Baber. In J. R. May (Ed.), Environmental Human Rights in the Anthropocene. Concepts, contexts, and challenges . Cambridge University Press.
Reyes, B. (2009). Chile governance assessment final report . PARC. Regina.
Robina Ramírez, R., & Sañudo-Fontaneda, L. (2018). Human Aspects of Water Management at impoverished settlements. The case of Doornkop. Soweto Water , 10 (3), 330. https://doi.org/10.3390/w10030330 .
Rodriguez, M. R. (2022). Chile’s New Constitution is Dead in the Water. Opinion. Newsweek. August 24, 2022. https://www.newsweek.com/chiles-new-constitution-dead-water-opinion-1735667 .
Rose, R. (1993). Lesson-drawing in public policy: A guide to learning across time and space . Chatham House. Chatham, N.J.
Roth, D., Vink, M., Warner, J., & Winnubst, M. (2017). Watered-down politics? Inclusive water governance in the Netherlands. OCEAN & COASTAL MANAGEMENT , 150 , 51–61. https://doi.org/10.1016/j.ocecoaman.2017.02.020 .
Sabatier, P. A., & Jenkins-Smith, H. C. (1993). Policy change and learning: An advocacy coalition approach . Boulder, Colo.: Westview.
Saltelli, A., & Giampietro, M. (2017). What is wrong with evidence based policy, and how can it be improved? Futures: The Journal of Policy Planning and Futures Studies , 91 , 62–71. https://doi.org/10.1016/j.futures.2016.11.012 .
save-its-culture.
Schmidt, M. G. (2004). Wörterbuch Zur Politik . Alfred Kröner.
Schmidt, V. (2010). Taking ideas and discourse seriously: Explaining change through discursive institutionalism as the fourth ‘new institutionalism’. European Political Science Review , 2 (1), 1–25.
Shade, L. (2015). Sustainable development or sacrifice zone? Politics below the surface in post-neoliberal Ecuador. Extr. Ind. Soc . 2015, 2, 775–784.
Sharma, P., & Kumar, S. N. (2020). The global governance of water, energy, and food nexus: Allocation and access for competing demands. Intl Environ Agreements , 20 , 377–391. https://doi.org/10.1007/s10784-020-09488-2 .
Smyth, R., Fatima, U., Segarra, M., Borre, L., Zilio, M., Reid, B., Pincetl, S., Astorga, A., Cisneros, M., Conde, D., Harmon, T., Hoyos, N., Escobar, J., Lozoya, J., Perillo, G., Piccolo, M., Rusak, J., & Velez, M. (2021). Engaging stakeholders across a socio-environmentally diverse network of water research sites in North and South America. ENVIRONMENTAL DEVELOPMENT , 38 . https://doi.org/10.1016/j.envdev.2020.100582 .
Somma, N. M. (2017). Discontent, collective Protest, and Social Movement in Chile. Chapter 2 in Malaise. In A. Joignant, M. Morales, & C. Fuentes (Eds.), Representation in Latin American Countries. Chile, Argentina and Uruguay . Palgrave McMillan.
Stone, D. (1988). Policy Paradox and political reason . Scott, Foresman and Company.
Surma, K. (2021). Ecuador’s High Court Affirms Constitutional Protections for the Rights of Nature in a Landmark Decision. Today’s Climate. https://insideclimatenews.org/news/03122021/ecuador-rights-of-nature/ .
Surma (2022). Chilean Voters Reject a New Constitution That Would have Provided Ground breaking Protections for the Rights of Nature. Inside Climate News. https://www.newsweek.com/chiles-new-constitution-dead-water-opinion-1735667 .
Tanasescu, M. (2013). The rights of nature in Ecuador: The making of an idea. International Journal of Environmental Studies , 70 , 846–861.
The Economist. (2022). Common sense prevails as chileans reject a new constitution. September 5, 2022. Santiago. The Americas . The Economist.
Toreti, A., Bavera, D., Acosta Navarro, J., Arias Munoz, C., Barbosa, P., de Jager, A., Di Ciollo, C., Fioraventi, G., Grimaldi, S., Essenfelder, G., Maetens, A., MAgni, W., Masante, D., Mazzeschi, D., McCormick, M., Salamon, N., & Spinoni, P. (2023). J. Drought in South America April 2023. JRC Technical Report. Luxembourg: Publications Office of the European Union. Available at: edo.jrc.ec.europa.eu.
Toussaint, P., & Blanco, A. M. (2019). A human rights-based approach to loss and damage under the climate change regime. Climate Policy . https://doi.org/10.1080/14693062.2019.1630354 .
UN (2010). Resolution Recognizing Access to Clean Water, Sanitation as Human Right. GA/10967 July 28, 2010.
UN (2023). UNdata. A world of information. https://data.un.org/en/index.html .
UN (2022). Mega-drought, glacier melt, and deforestation plague Latin America and the Caribbean. UN News. Global perspective Human Stories. July 22, 2022. United Nations. https://news.un.org/en/story/2022/07/1123032 .
Valladares, C., & Boelens, R. (2019). Mining for mother Earth. Governmentalities, sacred waters and nature’s rights in Ecuador. Geoforum , 100 , 68–79.
van den Berg, C., & Danilenko, A. (2019). The IBNET Water Supply and Sanitation Performance Blue Book, The International Benchmarking Network for Water and Sanitation Utilities Databook; The World Bank WSP: Washington, DC, USWaorani Pastaza Organization vs. Ecuador 2019\USA, 2011.
Villegas, A. (2023). Chileans reject conservative constitution to replace dictatorship era text. Reuters. Retrieved 18 December 2023. https://apnews.com/article/chile-new-constitution-referendum-f7be231ff564856f6a5e1b0c0ac12c57 .
Wingfield, S., Martínez-Moscoso, A., Quiroga, D., & Ochoa-Herrera, V. (2021). Challenges to Water Management in Ecuador: Legal authorization, Quality parameters, and socio-political responses. Water , 13 (8), 1017. https://doi.org/10.3390/w13081017 .
Wood, B. T., Dougill, A. J., Quinn, C. H., & Stringer, L. C. (2016). Exploring power and Procedural Justice within Climate Compatible Development Project Design: Whose priorities are being considered? Journal of Environment & Development , 25 (4), 363–395. https://doi.org/10.1177/1070496516664179 .
Wood, B., Dougill, A., Stringer, L., & Quinn, C. (2018). Implementing climate-compatible development in the context of power: Lessons for encouraging Procedural Justice through Community-Based projects. Resources (Basel) , 7 (2), 36. https://doi.org/10.3390/resources7020036 .
World Resources Institute (2015). Ranking the World’s Most Water-Stressed Countries in 2040. August 26, 20`5 by Andrew Maddocks, Rober Samuel young and Paul Reig. https://www.wri.org/insights/ranking-worlds-most-water-stressed-countries-2040 .
Yin, R. K. (2017). Case Study Research and Applications: Design and Methods. 6th Edition. Sage Publications.
Zibechi, R. (2009). Ecuador: The Logic of Development Clashes With Movements, Americas Program Report, March 17, 2009, americas.irc-online.org/am/5965 .
Zurn, M., Binder, M., & Ecker-Ehrhardt, M. (2012). International authority and its politicization. International Theory , 4 (1), 69–106. https://doi.org/10.1017/S1752971912000012 .
Zyri (2022). World. Chile faces the largest mega-drought in its history: Our country has changed forever. World. https://www.zyri.net/2022/04/13/chile-faces-the-largest-mega-drought-in-its-history-our-country-has-changed-forever/ .
Download references
Acknowledgements
The first author acknowledges the funding of the Canadian Research Chair Program and the Social Sciences and Humanities Research Council of Canada Partnership Grants (895-2021-0044); the second author acknowledges the research time of the University of Amsterdam and funding from the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation programme (contract number 101020082) and the Netherlands Enterprise Agency (RVO), under grant number 5000005700 and case number 31184622.
Author information
Authors and affiliations.
Centre for the Study of Science and Innovation Policy, Johnson-Shoyama Graduate School of Public Policy, University of Regina, 2155 College Avenue, Regina, SK, S4P 4V5, Canada
Margot Hurlbert
Governance and Inclusive Development, Amsterdam Institute for Social Science Research, University of Amsterdam, Nieuwe Achtergracht, Amsterdam, 1018 WV, The Netherlands
Joyeeta Gupta
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Joyeeta Gupta .
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Hurlbert, M., Gupta, J. The split ladder of policy problems, participation, and politicization: constitutional water change in Ecuador and Chile. Int Environ Agreements (2024). https://doi.org/10.1007/s10784-024-09644-y
Download citation
Accepted : 24 May 2024
Published : 19 June 2024
DOI : https://doi.org/10.1007/s10784-024-09644-y
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Participation
- Problem framing
- Policy change
- Windows of opportunity
- Water governance
- Water justice
- Constitutional change
- Find a journal
- Publish with us
- Track your research
2022 AIME II
2022 AIME II problems and solutions. The test was held on Wednesday, February 16, 2022. The first link will contain the full set of test problems. The rest will contain each individual problem and its solution.
- Entire Test
| ( • • ) | ||
| Preceded by | Followed by | |
Something appears to not have loaded correctly.
Click to refresh .
- Introduction
- Conclusions
- Article Information
BOLD indicates blood oxygen level dependent. b1 indicates the direct effect of videogaming on BOLD signal. b2 and b3 represent for each covariate the direct effects on videogaming and BOLD signal, respectively. The dashed blue arrow and the black arrow represent the indirect and total effects of each covariate on BOLD signal, respectively. Circled arrows represent the variance of each variable in the model.
A-D, Adjusted means and standard errors from linear mixed models accounting for sociodemographic factors are visualized. F, A t score of 59 or less indicates nonclinical symptoms, a t score between 60 and 64 indicates that the child is at risk for problem behaviors, and a t score of 65 or greater indicates clinical symptoms. The t score of 60 is visually represented with a dashed blue line on the graph. Whiskers represent SEs. ADHD indicates attention-deficit/hyperactivity disorder; OCD, obsessive-compulsive disorder; RT, reaction time; and SSRT, stop signal reaction time.
a Significant differences with false discovery rate–corrected P < .05.
b D' was calculated as the z -transformed hit rate minus the z -transformed false alarm rate.
SST indicates stop signal task.
eMethods. Stop Signal Task (SST), n-back Task, and fMRI Acquisition and Preprocessing
eMethods and eResults. List Sorting and Rey Auditory Verbal Learning Test
Retracted Article With Errors Highlighted
Replacement Article With Corrections Highlighted
- Clarifications for Variables and Findings and Corrections to Figures JAMA Network Open Correction August 8, 2023
- Video Games—Cognitive Help or Hindrance? JAMA Network Open Invited Commentary October 24, 2022 Kirk M. Welker, MD
See More About
Sign up for emails based on your interests, select your interests.
Customize your JAMA Network experience by selecting one or more topics from the list below.
- Academic Medicine
- Acid Base, Electrolytes, Fluids
- Allergy and Clinical Immunology
- American Indian or Alaska Natives
- Anesthesiology
- Anticoagulation
- Art and Images in Psychiatry
- Artificial Intelligence
- Assisted Reproduction
- Bleeding and Transfusion
- Caring for the Critically Ill Patient
- Challenges in Clinical Electrocardiography
- Climate and Health
- Climate Change
- Clinical Challenge
- Clinical Decision Support
- Clinical Implications of Basic Neuroscience
- Clinical Pharmacy and Pharmacology
- Complementary and Alternative Medicine
- Consensus Statements
- Coronavirus (COVID-19)
- Critical Care Medicine
- Cultural Competency
- Dental Medicine
- Dermatology
- Diabetes and Endocrinology
- Diagnostic Test Interpretation
- Drug Development
- Electronic Health Records
- Emergency Medicine
- End of Life, Hospice, Palliative Care
- Environmental Health
- Equity, Diversity, and Inclusion
- Facial Plastic Surgery
- Gastroenterology and Hepatology
- Genetics and Genomics
- Genomics and Precision Health
- Global Health
- Guide to Statistics and Methods
- Hair Disorders
- Health Care Delivery Models
- Health Care Economics, Insurance, Payment
- Health Care Quality
- Health Care Reform
- Health Care Safety
- Health Care Workforce
- Health Disparities
- Health Inequities
- Health Policy
- Health Systems Science
- History of Medicine
- Hypertension
- Images in Neurology
- Implementation Science
- Infectious Diseases
- Innovations in Health Care Delivery
- JAMA Infographic
- Law and Medicine
- Leading Change
- Less is More
- LGBTQIA Medicine
- Lifestyle Behaviors
- Medical Coding
- Medical Devices and Equipment
- Medical Education
- Medical Education and Training
- Medical Journals and Publishing
- Mobile Health and Telemedicine
- Narrative Medicine
- Neuroscience and Psychiatry
- Notable Notes
- Nutrition, Obesity, Exercise
- Obstetrics and Gynecology
- Occupational Health
- Ophthalmology
- Orthopedics
- Otolaryngology
- Pain Medicine
- Palliative Care
- Pathology and Laboratory Medicine
- Patient Care
- Patient Information
- Performance Improvement
- Performance Measures
- Perioperative Care and Consultation
- Pharmacoeconomics
- Pharmacoepidemiology
- Pharmacogenetics
- Pharmacy and Clinical Pharmacology
- Physical Medicine and Rehabilitation
- Physical Therapy
- Physician Leadership
- Population Health
- Primary Care
- Professional Well-being
- Professionalism
- Psychiatry and Behavioral Health
- Public Health
- Pulmonary Medicine
- Regulatory Agencies
- Reproductive Health
- Research, Methods, Statistics
- Resuscitation
- Rheumatology
- Risk Management
- Scientific Discovery and the Future of Medicine
- Shared Decision Making and Communication
- Sleep Medicine
- Sports Medicine
- Stem Cell Transplantation
- Substance Use and Addiction Medicine
- Surgical Innovation
- Surgical Pearls
- Teachable Moment
- Technology and Finance
- The Art of JAMA
- The Arts and Medicine
- The Rational Clinical Examination
- Tobacco and e-Cigarettes
- Translational Medicine
- Trauma and Injury
- Treatment Adherence
- Ultrasonography
- Users' Guide to the Medical Literature
- Vaccination
- Venous Thromboembolism
- Veterans Health
- Women's Health
- Workflow and Process
- Wound Care, Infection, Healing
Get the latest research based on your areas of interest.
Others also liked.
- Download PDF
- X Facebook More LinkedIn
Chaarani B , Ortigara J , Yuan D , Loso H , Potter A , Garavan HP. Association of Video Gaming With Cognitive Performance Among Children. JAMA Netw Open. 2022;5(10):e2235721. doi:10.1001/jamanetworkopen.2022.35721
Manage citations:
© 2024
- Permissions
Association of Video Gaming With Cognitive Performance Among Children
- 1 Department of Psychiatry, University of Vermont, Burlington
- Invited Commentary Video Games—Cognitive Help or Hindrance? Kirk M. Welker, MD JAMA Network Open
- Correction Clarifications for Variables and Findings and Corrections to Figures JAMA Network Open
Question What is the association between video gaming and cognitive performance in children?
Findings As part of the national Adolescent Brain Cognitive Development study and after controlling for confounding factors, results of this cross-sectional study of 2217 children showed very small levels of enhanced cognitive performance measured on inhibitory control and working tasks in children who played video games vs those who did not, although the video gamers had significantly higher attention problems, depression, and attention-deficit/hyperactivity disorder scores compared with the those who did not play video games. Functional MRI obtained clear blood oxygen level–dependent signal differences were associated with video gaming in task-related brain regions during inhibition control and working memory.
Meaning These findings suggest that video gaming may be associated with very small cognitive performance enhancement involving response inhibition and working memory, and with alterations in underlying cortical pathways, but concerns about the association with mental health may warrant further study.
Importance Although most research has linked video gaming to subsequent increases in aggressive behavior in children after accounting for prior aggression, findings have been divided with respect to video gaming’s association with cognitive skills.
Objective To examine the association between video gaming and cognitive performance in children using data from the Adolescent Brain Cognitive Development (ABCD) study.
Design, Setting, and Participants In this cross-sectional study, cognitive performance and blood oxygen level–dependent (BOLD) signal were compared in video gamers (VGs) and non–video gamers (NVGs) during response inhibition and working memory using task-based functional magnetic resonance imaging (fMRI) in a large data set of 9- and 10-year-old children from the ABCD study. A sample from the baseline assessment of the ABCD 2.0.1 release in 2019 was largely recruited across 21 sites in the US through public, private, and charter elementary schools using a population neuroscience approach aiming to mirror demographic variation in the US population. Children with valid neuroimaging and behavioral data were included, with adjustments performed for demographic, behavioral, and psychiatric confounding factors. Some exclusions included common MRI contraindications, history of major neurologic disorders, and history of traumatic brain injury. Collected data were analyzed between October 2019 and October 2020, with additional analyses in 2023.
Exposures Participants completed a self-reported screen time survey, including an item asking children to report the time specifically spent on video gaming. All fMRI tasks were performed by all participants.
Main Outcomes and Measures Cognitive performance, assessed with stop signal tasks (SST) and n-back tasks; and BOLD signal on fMRI during the tasks. Mental health symptoms were evaluated using the Child Behavior Checklist and included raw scores of behavioral (anxiety, depression, somatic, social, attention, rule breaking, and aggression concerns) and psychiatric categories ( Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition , diagnoses of depression, anxiety, somaticism, attention-deficit/hyperactivity disorder, oppositional-defiant disorder, and conduct disorder).
Results A total of 2217 children (mean [SD] age, 119 [7.6] months; 9.91 [0.62] years; 1399 [63.1%] female) participated in this study. The final sample used in the stop signal task analyses consisted of 1128 NVGs (0 gaming hours per week) and 679 VGs who played at least 21 hours per week. The final sample used in the n-back analyses consisted of 1278 NVGs who had never played video games (0 hours per week of gaming) and 800 VGs who played at least 21 hours per week. The NVG vs VG groups did not differ on age but did differ on sex, race and ethnicity, combined parental income, body mass index, and IQ. There were no differences in body mass index and IQ after adjusting for sociodemographic variables. The Child Behavior Checklist behavioral and mental health scores were higher in VGs, with attention problems, depression, and attention-deficit/hyperactivity disorder scores significantly higher in the VGs compared with the NVGs. The VGs performed better on both fMRI tasks compared with the NVGs; the differences were statistically significant but very small. VGs had significantly faster stop signal reaction times compared with NVGs (adjusted means [SE]; 287.3 [9.8] vs 300.1 [9.6], standardized mean difference [SMD] 0.04 milliseconds; P = .018) and correct go reaction times (adjusted means [SE], 514 [2.9] vs 552 [2.2] milliseconds; SMD 0.05; P = .002). Following a similar pattern, 0-back D' measures of the n-back task were significantly higher in VGs compared with NVGs (adjusted means [SE], 2.33 [0.03] vs 2.18 [0.03]; SMD, 0.15; P < .001). Similarly, adjusted means (SE) 2-back D′ scores were significantly higher in VGs relative to NVGs (1.87 [0.03] vs 1.72 [0.02]; SMD 0.15; P < .002), and reaction times for correct responses during the 2-back conditions were faster in VGs relative to NVGs (adjusted means [SE]; 1025 [4.8] vs 1069 [3.7] milliseconds; P < .002). Nonparametric analyses of fMRI data demonstrated a greater BOLD signal in VGs in the precuneus during inhibitory control. During working memory, a smaller BOLD signal was observed in VGs in parts of the occipital cortex and calcarine sulcus and a larger BOLD signal in the cingulate, middle, and frontal gyri and the precuneus.
Conclusions and Relevance In this study, compared with NVGs, VGs were found to exhibit faster reaction times in measures of cognitive performance involving response inhibition and working memory and differences in fMRI BOLD signals in key regions of the cortex responsible for visual, attention, and memory processing. The very small differences in reaction times lack clinical relevance but were consistent with a potential association between videogaming and cognitive performance that involve response inhibition and working memory and the underlying cortical pathways. Concerns about the association with mental health symptoms may warrant further study.
Ask any parent how they feel about their child’s videogaming and you will almost certainly hear concerns about hours spent in a virtual world and the possibility of adverse effects on cognition, mental health, and behavior. A contributing factor to these concerns is the growth of video gaming within the last 20 years. In tandem, the demographic makeup of gamers has also been rapidly changing. In children aged 2 to 17 years, a large 2022 survey in the US showed that 71% play video games, an increase of 4 percentage points since 2018. 1 Given the substantial brain development that occurs during childhood and adolescence, these trends have led researchers to investigate associations between gaming and cognition and mental health. Most psychological and behavioral studies 2 suggest detrimental associations of video gaming, linking it to subsequent increases in depression, violence, and aggressive behavior in children after accounting for prior aggression. However, researchers have been divided with respect to whether playing video games is associated with cognitive skills and brain function. In contrast to the negative associations with mental health, video gaming has been proposed to enhance cognitive flexibility by providing skills that can be transferred to various cognitive tasks relevant for everyday life. One formulation for this broad transfer is that video gaming shares a number of perceptual and attentional demands (such as multiple object tracking, rapid attentional switches, and peripheral vision) with common cognitive tasks and can enhance reaction time (RT), creativity, problem solving, and logic. 3 , 4
In a previous review investigating video gaming and cognitive tasks, 3 gaming was found to be associated with attentional benefits, including improvements in bottom-up and top-down attention, optimization of attentional resources, integration between attentional and sensorimotor areas, and improvements in selective and peripheral visual attention. Video gamers (VGs) may also benefit from an enhanced visuospatial working memory capacity according to Boot et al, 5 who found that VGs outperformed non-VGs (NVGs) on various visuospatial working memory tasks, such as multiple object tracking, mental rotation, and change detection. Working memory improvements were similarly found after video game training in experimental vs control group research designs. 5 - 7 This finding is consistent with other studies suggesting that even short video game training paradigms can enhance cognitive control–related functions for long durations, such as reading abilities in dyslexic children 8 and, more particularly, working memory. 3
Task-based functional magnetic resonance imaging (fMRI) studies 4 , 9 - 11 have compared brain activity between VGs and NVGs. When presented with a complex visuomotor task, Granek et al 4 found that VGs exhibited more blood oxygen level–dependent (BOLD) activity in the prefrontal cortex but less overall brain activity compared with NVGs. In 1 study using an fMRI attentional letter detection task, Richlan et al 9 found no significant behavioral performance differences between 14 VGs and 14 NVGs, but VGs showed more brain activation in multiple frontoparietal regions and different activation patterns, suggesting that VGs may recruit different regions of the brain to perform attentional tasks. In the same study, 9 no differences between the 2 groups were observed during a working memory visuospatial task in overall performance (in accuracy or RT) or in brain activation. In a more recent study, Trisolini and colleagues 10 investigated sustained performance between VGs and NVGs in 2 attentional tasks. The results indicated that although VGs displayed significantly stronger performance at the beginning of the task, a substantial decrease in performance was observed over time. By the end of the task, NVGs performed more accurately and quicker. Moreover, in a study 11 investigating the short-term impact of different activities performed during a break before an n-back working memory test in an fMRI scan, 27 young adults who played video games during the break displayed poorer working memory task performance and less BOLD activity in the supplementary motor area compared with those who had listened to music. However, VGs showed neither performance nor BOLD differences compared with those who spent the break resting. The authors reasoned that the video-gaming demands may have fatigued specific cognitive resources that rely on the supplementary motor area and reduced the ability of VGs to focus attention on the subsequent working memory task. 11 This finding is in contrast with another study 3 that suggested that even short video game training paradigms can enhance cognitive control–related functions, particularly working memory, with the enhancement linked to activity changes in prefrontal areas, such as the dorsolateral prefrontal cortex and the orbitofrontal cortex.
In brief, although several studies have investigated the association between video gaming and cognitive behavior, the neurobiological mechanisms underlying the associations are not well understood because only a handful of neuroimaging studies have addressed this topic. In addition, findings from fMRI studies on video gaming in children and adolescents have not been replicated, which could be in part attributable to the relatively small sample sizes included in the analyses (N<80). In this study, we assess video-gaming associations with cognitive performance and brain activation during response inhibition and working memory using task-based fMRI in a large data set of 9- and 10-year-old children from the Adolescent Brain Cognitive Development (ABCD) study, 12 the largest long-term study of brain development and child health in 21 research sites across the US. We hypothesized, based on the literature, that VGs would perform better on the tasks and have altered cortical activation patterns compared with NVGs in key areas of the brain involved in inhibitory control and working memory.
This cross-sectional study used data from the baseline assessment of the ABCD study 2.0.1 release in 2019, which recruited a large sample of 9- to 10-year-old children from whom neuroimaging and behavioral data were acquired and quality controlled according to standard operating procedures for the ABCD study consortium. 5 All measurements were collected at enrollment in the ABCD study. The fMRI paradigms were preprocessed with standard automated pipelines using Analysis of Functional NeuroImages and included the stop signal task (SST) and the n-back task. Children were asked to report how many hours per week they play video games on a computer, console, smart phone, or other devices. Consent (parents) and assent (children) were obtained from all participants. The ABCD study was approved by the appropriate institutional review boards: most ABCD research sites rely on a central Institutional Review Board at the University of California, San Diego for the ethical review and approval of the research protocol, with a few sites obtaining local IRB approval.
The ABCD sample was largely recruited through public, private, and charter elementary schools. The ABCD study adopted a population neuroscience approach to recruitment 13 , 14 by using epidemiologically informed procedures to ensure demographic variation in its sample that would mirror the variation in the US population of 9- and 10-year-olds. 15 A probability sampling of schools was conducted within the defined catchment areas of the study’s nationally distributed set of 21 recruitment sites in the US. All children in each sampled school were invited to participate after classroom-based presentations, distribution of study materials, and telephone screening for eligibility. Exclusions included common MRI contraindications (such as stainless steel braces, cardiac pacemakers and defibrillators, internal pacing wires, cochlear and metallic implants, and Swan-Ganz catheters), inability to understand or speak English fluently, uncorrected vision, hearing or sensorimotor impairments, history of major neurologic disorders, gestational age less than 28 weeks, birth weight less than 1200 g, birth complications that resulted in hospitalization for more than 1 month, current diagnosis of schizophrenia, moderate or severe autism spectrum disorder, history of traumatic brain injury, or unwillingness to complete assessments. The ABCD study sample also includes 2105 monozygotic and dizygotic twins. The ABCD study’s anonymized data, including all assessment domains, are released annually to the research community. Information on how to access ABCD study data through the National Institute of Mental Health Data Archive is available on the ABCD study data-sharing webpage. 16
Participants were administered a screen time survey that asked how much time they spend engaged in different types of screen time on a typical weekday and a typical weekend day. The different screen time categories were as follows: “Watch TV shows or movies?”; “Watch videos (such as YouTube)?”; “Play video games on a computer, console, phone, or other device (Xbox, Play Station, iPad)?”; “Text on a cell phone, tablet, or computer (eg, GChat, Whatsapp, etc.)?”; “Visit social networking sites like Facebook, Twitter, Instagram, etc?”; and “Video chat (Skype, Facetime, etc)?” For each of these activities, the participants responded with how much time they spent per day doing them. They could answer none, less than 30 minutes, 30 minutes, 1 hour, 2 hours, 3 hours, or 4 hours. Answers were mostly none for the texting, social networking, and video chatting categories, as expected for this age range. For each participant, a total weekly video-gaming score was derived as the sum of (video-gaming hours per weekday × 5) + (video-gaming hours per weekend day × 2). A total weekly watching videos score was also derived for each participant. Using the video-gaming score, we defined a group of NVGs who never played video games (0 gaming hours per week) and a group of VGs who played a minimum of 3 hours per day (21 hours per week) or more. This threshold was selected because it exceeds the American Academy of Pediatrics screen time guidelines, 17 which recommends that video-gaming time be limited to 1 to 2 hours per day for older children.
The child’s age, sex, and race and ethnicity were reported by the parent at the baseline assessment. Race and ethnicity categories included Asian, Black, Hispanic, White, and other (which included American Indian, Alaska Native, Native Hawaiians, Pacific Islander, and multiple racial and ethnic categories). A trained researcher measured children’s height (to the nearest inch) and weight (to the nearest 0.1 lb). Height and weight were assessed 2 times, and means were recorded. Height and weight were converted to body mass index (BMI) scores (according to the Centers for Disease Control and Prevention BMI cutoffs 18 ). IQ scores were derived from the National Institutes of Health Toolbox cognition battery 19 as the mean of crystalized intelligence and fluid intelligence composite, age-corrected scores. The Pubertal Development Scale (PDS) 20 was used to assess the child’s pubertal stage. The PDS is a noninvasive measure that assesses current pubertal status in females and males, in which higher scores indicate further progression in puberty. Mental health symptoms were evaluated using the Child Behavior Checklist (CBCL) 21 , and included raw scores of behavioral (anxiety, depression, somatic, social, attention, rule-breaking, and aggression concerns) and psychiatric categories ( Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, diagnoses of depression, anxiety, somaticism, attention-deficit/hyperactivity disorder [ADHD], oppositional-defiant disorder, and conduct disorder).
The ABCD imaging protocol was designed to extend the benefits of high temporal and spatial resolution of imaging protocols of the Human Connectome Project 22 with the multiple scanner systems of participating sites. 23 High spatial and temporal resolution simultaneous multislice and multiband echo-planar imaging task-based fMRIs, with fast integrated distortion correction, were acquired to examine functional activity. For the 3-T scanners (Siemens and GE), the scanning parameters were as follows: matrix, 90 × 90; 60 slices; field of vision, 216 × 216; echo time/repetition time, 800/30 milliseconds; flip angle, 52°; and resolution, 2.4 × 2.4 × 2.4 mm. The fMRI acquisitions (2.4-mm isotropic with repetition time of 800 milliseconds) used multiband echo-planar imaging with slice acceleration factor 6. The order of fMRI tasks was randomized across participants. The fMRI preprocessing pipeline included a within-volume head motion estimation and correction and a correction for image distortions. Estimates of task-related activation strength (measured with BOLD activity levels of 10242 vertices/hemisphere) were computed at the individual participant level using a general linear model implemented in Analysis of Functional NeuroImages 3dDeconvolve, with additional nuisance regressors and motion estimates. Hemodynamic response functions were modeled in Analysis of Functional NeuroImages with 2 parameters using a γ-variate basis function plus its temporal derivative.
The SST and n-back task were selected from the ABCD imaging battery to probe inhibitory control and working memory, respectively. Participants practiced the 2 tasks before scanning to ensure they understood the instructions and were familiar with the response collection device. These 2 tasks yield robust neural activation patterns as demonstrated previously. 24 Quality control criteria included excluding participants based on poor image quality, motion, or task performance. The full details of the tasks and fMRI acquisition, preprocessing, and quality control are described in the eMethods in Supplement 1 and by Hagler et al. 22
The adaptive algorithm used in the SST allowed for calculation of the stop signal RT (SSRT; the time required to inhibit the motor response 24 ), which was used as the performance variable in analyses that assessed individual differences in response inhibition ability. The SSRT was computed by subtracting the median stop signal delay of all successful stop trials from the n th percentile go RT, where n represents the percentage of successful inhibitions (for details on the theoretical underpinnings for this estimation, see the study by Logan and Cowan 25 ). To evaluate behavioral task performance in the n-back task, D’ (calculated as the z -transformed hit rate minus the z -transformed false alarm rate) was computed for both the 2-back and 0-back conditions by calculating each participant’s hit rate (the proportion of targets for which the participant correctly indicated a match) and the false alarm rate (the proportion of nontargets for which the participant incorrectly indicated a match or did not respond). The hit and false alarm rates were then z transformed. Cognitive performance was also assessed with tasks not relying on visual-motor coordination (list sorting working memory task and Rey Auditory Verbal Learning Test), as described in the eMethods in Supplement 1 .
Participants were included if they had (1) 2 fMRI runs per task, (2) cortical vertex and subcortical voxel data available at the time of analysis, (3) hemispheric mean BOLD signal within 2 SDs of the sample mean for each task, (4) at least 200 df during the 2 scan runs, (5) mean framewise displacement less than 0.9 mm for both runs, (6) met task-specific performance criteria (described in the eMethods in Supplement 1 ), and (7) had complete information on the screen time survey and for all other variables (CBCL, age, sex, scanner serial number, puberty, race and ethnicity, and combined parental income).
Collected data were analyzed between October 2019 and October 2020, with additional analysis in 2023. Unadjusted demographic characteristics (age, sex, race and ethnicity, household income), BMI and IQ, and scanner manufacturer were compared between VGs and NVGs using 2-tailed t tests and χ 2 analyses. To compare the 2 groups on IQ, BMI, and mental health as outcome measures, we use linear mixed models, controlling for sociodemographic factors (age, sex, puberty, race and ethnicity, and household income), and including site as a random effect. Linear mixed models were also used to compare VG and NVG on the 4 task-performance measures: SSRT, correct go RT in the SST, and 0-back and 2-back D′ in the n-back. These models included age, sex, race and ethnicity, IQ, puberty, and combined parental income as adjustment variables, and site as a random effect. Based on the fits of these models, group-specific estimated marginal means (referred to as adjusted means), standard errors and standardized mean differences (SMDs) were calculated for each performance measure. Analyses were carried out in SPSS (version 28.0).
Cortical task-fMRI BOLD signal contrasts (10242 vertices/hemisphere) were compared between VGs and NVGs using vertexwise permutation analyses via the fit of a Permutation Analysis of Linear Models (PALM) general linear model. 26 Task-fMRI contrasts included correct stop vs correct go and incorrect stop vs correct go conditions of the SST, as well as 0-back vs fixation and 2-back vs fixation conditions of the n-back test. Throughout age (months), sex, scanner serial number, race and ethnicity, IQ, puberty, and combined parental income were included as adjustment variables. Furthermore, nonindependence of siblings was acknowledged using sibling status as a nested covariate in the model using PALM’s exchangeability blocks, 27 which restrict the shuffling to only occur among the observations that share the same family index (ie, number of siblings). Note, sibling status was only included in the neuroimaging analyses because the permutation design with exchangeability blocks allows for optimal modeling of nested covariates, such as sibling status and site.
Additional task measurements not relying on visuomotor coordination included a list sorting working memory task and the Rey Auditory Verbal Learning Test and are described in the eMethods in Supplement 1 .
All statistical tests were 2-sided. False discovery rate (FDR) was assessed with the Benjamini and Hochberg procedure, and corrected P values and statistical maps were considered significant at P < .05.
To investigate the potential mediating role that time spent watching videos, behavioral problems, or psychiatric disorders have in the association between video gaming with BOLD signal activation during SST and n-back tasks, we used structural equation modeling to model the association between video gaming (independent variable) and activation in the SST and n-back task (dependent variable), with video watching, behavioral problems, and psychiatric disorders scores included as covariates ( Figure 1 ). β Coefficients from the fMRI general linear model (model described in the eMethods in Supplement 1 ) were extracted using MATLAB (MathWorks) for each task and contrast from vertexes showing significant differences between NVGs and VGs in the vertexwise analyses. Mean β coefficients were computed for each contrast and included as the BOLD signal variable in the model. Total behavioral problems and psychiatric disorder scores were calculated from the CBCL 21 as the sum of the scores of all of the problem and psychiatric items, respectively. The direct effect of video gaming on BOLD signal (parameter b1) served to check whether any initial association remained significant after controlling for the covariates included in the model. This determination was accomplished by letting each covariate predict both video gaming and BOLD signal such that each covariate could have direct effects (represented as b2 and b3) as well as an indirect effect on BOLD signal via video gaming (b1 × b2) ( Figure 1 ). In this regard, video gaming could be interpreted as a mediator of the covariates’ effects. The total effect of covariates on the BOLD signal equals b1 × b2 + b3, whereas the covariate-corrected effect of video gaming on the BOLD signal equals b1. The root mean square error of approximation, comparative fit and Tucker-Lewis indices, defined as measures of the goodness-of-fit of statistical models, were also calculated for each model. The model was specified in R software, version 4.0.4 (R Foundation for Statistical Computing) using the structural equation modeling package lavaan, 28 version 0.6-7.
A total of 2217 children (mean [SD] age, 119 [7.6] months; 9.91 [0.62] years; 1399 [63.1%] females) participated in this study ( Table 1 ). The final sample used in the SST analyses consisted of 1128 NVGs who had never played video games (0 gaming hours per week) and 679 VGs who played 21 hours per week or more. The final sample used in the n-back analyses consisted of 1278 NVGs who had never played video games (0 hours per week of gaming) and 800 gamers who played 21 hours per week or more.
The NVG vs VG between-group comparisons showed that groups did not differ on age, but did differ on sex, race and ethnicity, combined parental income, and raw BMI and IQ measures ( Table 1 ). Comparison of NVGs and VGs using linear mixed models showed the adjusted means of BMI and IQ did not differ between the 2 groups ( Table 2 ). Although mental health and behavioral scores from the CBCL were consistently higher in VGs, these differences reached statistical significance for attention problems, depression, and ADHD scores (FDR P < .05) ( Figure 2 ). The t scores from the CBCL were less than 56 in both groups and thus, none of the measures in either group was high enough to reach clinical significance ( Figure 2 ).
Performance on the SST was in the anticipated range (mean [SE] SSRT, 293.7 [9.7] milliseconds; mean [SE] go RT, 538 [1.82] milliseconds), with a mean (SE) rate of correct inhibitions of 51.5% (0.001%). The distributions for D′ were as expected, with children performing better on the 0-back task (mean [SE] D′ = 2.25 [0.03] milliseconds) than the 2-back task (mean [SE] D′ = 1.8 [0.03] milliseconds; P < .001). Linear mixed models compared task performance measures between NVGs and VGs with age, sex, puberty, race and ethnicity, household income, and scanner site included as covariates. Analyses showed that videogaming was associated with small improvements in performance in the SST and n-back tasks ( Figure 2 ). In the SST, compared with NVGs, VGs had statistically significantly faster reaction times. The adjusted means (SE) times for SSRT were 287.3 (9.8) vs 300.1 (9.6) milliseconds (SMD 0.04 milliseconds; P = .02), and the adjusted means (SE) times for correct go RT were 514 (2.9) vs 552 (2.2) milliseconds (SMD, 0.5 milliseconds; P = .002). Following a similar pattern, the 0-back D' score was significantly higher in VGs relative to NVGs (adjusted means [SE], 2.33 [0.03] vs 2.18 [0.03]; P < .001) ( Table 2 ). Similarly, 2-back D′ was significantly higher in VGs relative to NVGs (adjusted means [SE], 1.87 [0.03] vs 1.72 [0.02]; P < .002). Reaction time for correct responses during the 2-back condition were significantly faster in VGs relative to NVGs (adjusted means [SE], 1025 [4.8] vs 1069 [3.7]; P < .002) ( Table 2 and Figure 2 ). Compared with NVGs, VGs, scored lower on the list sorting working memory task, and there were no differences between groups on the Rey Auditory Verbal Learning Test (see eMethods and eResults in Supplement 1 ).
Families with 2 siblings consisted of less than 5% and families with 3 siblings of less than 0.1% in both fMRI samples. In the correct stop vs correct go condition of the SST, vertexwise analyses showed significantly greater BOLD signal in VGs compared with NVGs in the bilateral precuneus ( Figure 3 ). No significant differences were observed in the incorrect stop vs correct go condition of the SST.
In the 2-back vs fixation condition of the n-back task, a significantly greater BOLD signal was observed in VGs compared with NVGs in bilateral parts of the dorsal posterior cingulate gyrus, subparietal cortex, middle and superior frontal gyri, and precuneus ( Figure 3 ). Meanwhile, a smaller BOLD signal was observed in VGs in the 2-back vs fixation condition in bilateral parts of the occipital cortex and the calcarine sulcus ( Figure 3 ). The direction, anatomical label, cluster size, and peak vertex number for each cortical region showed significant changes between VGs and NVGs ( Table 3 ). Cortical clusters showing these differences in the n-back sample also survive a Bonferroni familywise error correction at P < .05. Similar patterns of BOLD differences between VGs and NVGs were observed in male and female groups examined separately. No significant differences were observed in the 0-back vs fixation condition of the n-back task.
The two structural equation models (for the SST and n-back task) showed good fits with root mean square error of approximation less than 0.04, a comparative fit index greater than 0.9, and Tucker-Lewis Index greater than 0.9. Video watching was positively associated with video gaming for both models (estimates, 0.12 for SST and 0.14 for n-back tasks; P ≤ .001). However, video watching and total behavioral and psychiatric problems did not have significant direct (b3), indirect (b1 × b2), or total ([b2 × b1] + b3) effects on the BOLD signal in either model. Of importance, the direct effect of video gaming on the BOLD signal remained significant in both models.
Data were missing or partially missing on the screen time questionnaire for 11 NVG participants (0.5% of the sample). We reran our analyses on both SST and n-back task-fMRI data, as well as behavioral and mental health measures with and without those participants, and there were no differences in the adjusted means or statistical significance of our findings.
To date and to our knowledge, this is the largest study to assess the association among video gaming, cognitive performance, and brain function. The behavioral performance findings showed that VGs performed better on both the SST and n-back task compared with NVGs; however, the differences were very small and measured in fractions of milliseconds. The fMRI findings demonstrated that VGs show a greater BOLD signal in bilateral parts of the precuneus, using an SST probing inhibitory control. Moreover, results showed a smaller BOLD signal in VGs in parts of the occipital cortex and calcarine sulcus and more activation in cingulate, subparietal, middle, and frontal gyri, and the precuneus during the n-back working memory task. In line with psychological and behavioral studies 2 that suggest detrimental associations of video gaming with mental health in children, we observed significantly higher attention problems, depression, and ADHD scores in VGs compared with NVGs. The marginally higher scores in VGs in the other CBCL categories leave open the possibility that VGs may be on a trajectory to show more mental health symptoms with time and more exposure to video gaming.
The behavioral performance findings in the SST sample are in line with the behavioral findings of the studies by Chisholm et al 29 and Bavelier et al, 30 showing that VGs are less susceptible to attentional distraction and outperform NVGs on both selection-based and response-based processes, suggesting that enhanced attentional performance in VGs may be underpinned by a greater capacity to suppress or disregard irrelevant stimuli. However, these results contradict those obtained in previous studies 31 , 32 that used go/no-go tasks and those showing higher impulsivity levels to be associated with video gaming. These studies 31 , 32 adopted a different design and outcome measures, included young adult age ranges, and had small sample sizes (n < 56). The behavioral performance findings in the n-back task are also in accordance with previous studies showing enhanced visuospatial working memory performance in VGs compared with NVGs 5 , 33 and in experimental vs control groups after video game training sessions. 5 - 7 , 34 In both tasks, the significantly faster millisecond RTs in VGs compared with NVGs while simultaneously performing more accurately may reflect improved cognitive skills acquired through video gaming and not caused by impulsive responding. According to a previous EEG study, 35 earlier latencies in the visual pathways are another feature found in VGs, which may contribute to faster RTs in visual tasks after years of practice. The faster millisecond performance times on both the SST and n-back task is supported by previous studies showing that VGs outperform NVGs on a range of cognitive tasks 36 (a flanker task, an enumeration task, and 2 attentional blink tasks) and on crystallized and fluid intelligence measures assessed via the Youth National Institutes of Health Toolbox. 37 In addition, supporting our findings, research on video game training in groups of NVGs using action video games (mainly enhancing one’s attentional control) demonstrated that video game training consistently led to transferrable improvements in cognitive performance. 38
The imaging findings showing a greater BOLD signal associated with video gaming during the SST in the precuneus—a brain region involved in a variety of complex functions including attention, cue reactivity, memory, and integration of information—are consistent with previous fMRI studies 3 in children and young adolescents using response inhibition tasks showing more activation in VGs in parietal areas of the cortex, including the precuneus. More broadly, the findings agree with the evidence that VGs display enhanced overall neural recruitment in a range of attentional control areas during response inhibition tasks. 3 Of interest, in a previous study 39 investigating changes in resting state functional connectivity after video game practice in young participants using a test-retest design, the key finding was increased correlated activity during rest in the precuneus, suggesting that this area exhibits a practice effect associated with the cognitively demanding video games. 39 Advantages for VGs in various attention-demanding tasks have also been reported by Cardoso-Leite et al. 40 Moreover, in line with our findings, an electroencephalography study 41 showed that heavy-use VGs had larger event-related potential amplitudes relative to NVGs in response to numerical targets under high load conditions, suggesting that heavy-use VGs may show greater sensitivity than NVGs to task-relevant stimuli under increased load, which in turn may underpin greater BOLD changes and improved behavioral performance compared with mild-use VGs and NVGs.
Our finding of less activation in VGs in occipital areas while performing better on the n-back task is consistent with a previous fMRI study 33 that used a visuomotor task and showed less activation in occipitoparietal regions in VGs and improved visuomotor task performance; these findings suggest a reduction in visuomotor cognitive performance measures as a consequence of the video gaming practice. In addition, in line with our results, Granek et al, 4 using an increasingly complex visuomotor fMRI task, observed greater prefrontal activation in 13 VGs who played a mean (SD) of 12.8 (8.6) hours per week during the preceding 3 years compared with 13 NVGs, which the authors related to the increased online control and spatial attention required by VGs for processing complex, visually guided reaching. Similarly, Gorbet and Sergio 42 found that VGs showed less motor-related activity in the cuneus, middle occipital gyrus, and cerebellum, which they explained as an indicator that VGs have greater neural efficiency when conducting visually guided responses. In addition, previous fMRI research has found significantly greater activation related to video gaming in regions associated with working memory, including the subparietal sulcus and the precuneus. 43 , 44 In a more recent study, 45 changes in BOLD signal in the subparietal lobe, precentral gyrus, and precuneus from before to after training using a video game with a working memory component predicted changes in performance in an untrained working memory task, suggesting a practice-induced plasticity in these regions.
Although video watching is highly confounded with video gaming in our fMRI samples, our models indicate that the response inhibition and working memory effects remained significant when controlling for video watching (in addition to behavioral and psychiatric problems), suggesting that the observed BOLD alterations in the SST and n-back task are more specific to video gaming than video watching. This finding is important because it suggests that children must actively engage with a video’s content, as opposed to passively watching a video, to exhibit altered brain activation in key areas of the brain involved in cognition.
This study has some limitations, and the findings should be interpreted with caution. The 2 groups were different in terms of sex, race and ethnicity, parental income, and mental health and behavioral scores. While the results show statistically different SSRTs (287.3 [9.8] vs 300.1 [9.6] milliseconds), these are very small differences without clear implications. In addition, video games regroup a variety of gaming categories that include action-adventure, shooters, puzzle solving, real-time strategy, simulation, and sports. These specific genres of video games may have different effects for neurocognitive development 46 because they do not all equally involve interactive (ie, multisensory and motor systems) and executive function processes. In addition, single vs multiplayer games may also have differential impacts on the brain and cognition. 46 Not including the video-gaming genre in our analyses is a limitation of the current study because the screen time survey in the ABCD database does not include additional information on the genre of video games played. Future large studies investigating the association between video gaming and cognition would benefit from including game genre as a moderating variable in analyses. Another limitation of the current study is the use of only cross-sectional study designs, which cannot provide enough evidence to resolve causality or the directionality of the associations among video gaming and other variables. For example, we cannot resolve whether mental health issues or brain function changes precede and drive video gaming or whether video gaming results in mental health symptoms or altered neuroplasticity. Future works benefiting from the longitudinal design of the ABCD study will enable researchers to move beyond association toward causation using causal approaches, such as discordant twin analyses, bayesian causal networks, and machine learning.
Overall, even with consideration of the correlational nature of these cross-sectional data, the current findings are consistent with video gaming being associated with faster performance on cognitive tests that involve response inhibition and working memory and altered BOLD signal on these tasks, although the differences in task performances were very small and measured in fractions of milliseconds. The results raise the possibility that video gaming may provide a cognitive training experience with measurable neurocognitive effects. However, the CBCL behavioral and mental health scores were higher in children who played video games for 3 or more hours a day, with attention problems, depression, and ADHD scores significantly higher in the VGs compared with the NVGs. Future ABCD data releases will allow researchers to test for longitudinal effects in which video gaming might improve response inhibition, working memory, and other cognitive functions, as previously suggested in a longitudinal intervention study 34 in which episodic and short-term memory gains were maintained during a 3-month follow-up period, as well as the association of mental health symptoms with exposure to video gaming. The longitudinal design of the ABCD study will enable within-participant testing for the correlates of accumulated video-gaming practice over the years. By using methods such as cross-lagged correlations or causal inference, researchers can assess whether video gaming is associated with subsequent mental health symptoms, behavioral issues, or neurocognitive development in adolescents.
Accepted for Publication: August 20, 2022.
Published: October 24, 2022. doi:10.1001/jamanetworkopen.2022.35721
Retraction and Replacement: This article was retracted on April 10, 2023, to fix errors in the analysis in the Key Points, Abstract, main text, Table 1 , and Figure 2 (see Supplement 2 for the retracted article with errors highlighted and Supplement 3 for the replacement article with corrections highlighted).
Correction: This article was corrected on August 8, 2023, to add clarifications to the text and Supplement 1 , report the demographic variables in Table 1 and the adjusted outcomes in Table 2 , and correct Figures 1 and 2 .
Open Access: This is an open access article distributed under the terms of the CC-BY License . © 2022 Chaarani B et al. JAMA Network Open .
Corresponding Author: Bader Chaarani, PhD, Department of Psychiatry, University of Vermont, 1 S Prospect St, Burlington, VT 05405 ( [email protected] ).
Author Contributions: Drs Chaarani and Garavan had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: Chaarani, Garavan.
Acquisition, analysis, or interpretation of data: All authors.
Drafting of the manuscript: Chaarani, Ortigara, Garavan.
Critical revision of the manuscript for important intellectual content: Chaarani, Yuan, Loso, Potter, Garavan.
Statistical analysis: Chaarani, Ortigara, Yuan, Loso, Garavan.
Obtained funding: Chaarani, Potter, Garavan.
Administrative, technical, or material support: Chaarani, Ortigara, Potter.
Supervision: Chaarani, Garavan.
Conflict of Interest Disclosures: Dr Potter reported receiving grants from the National Institutes of Health during the conduct of the study. No other disclosures were reported.
Additional Contributions: We thank Shana Adise, PhD, and Nicholas D. Allgaier, PhD (Department of Psychiatry, University of Vermont, Burlington), for conducting independent statistical analyses for the corrected article.
Additional Information: Data used in the preparation of this article were obtained from the Adolescent Brain Cognitive Development (ABCD) Study ( https://abcdstudy.org ) held in the National Institute of Mental Health Data Archive. Computations were performed on the Vermont Advanced Computing Core supported in part by award OAC-1827314 from the National Science Foundation.
- Register for email alerts with links to free full-text articles
- Access PDFs of free articles
- Manage your interests
- Save searches and receive search alerts
IMAGES
VIDEO
COMMENTS
Each year 30,000+ K-12 students in 34+ U.S. states and 14 countries participate in a variety of Future Problem Solving challenges. Each year 30,000+ K-12 students from around the world participate in a variety of Future Problem Solving real world challenges. ... 2022 Champion Junior Division (Community Projects) Our Topic Center. Real issues ...
Submit a Topic. 2016-17, 2018-19, 2019-20, 2020-21, 2021-22, 2022-23, 2023-24 2024-25, Affiliate Finals Problem, International Conference, Practice Problem, Qualifying Problem, STEM Topics, World Solutions Challenge. Visit our topic center to learn more about current and past Future Problem Solving student competition topic challenges.
Create innovative solutions and solve tough problems fast with these problem-solving techniques! Solving challenges is easier with the right methods. Create innovative solutions and solve tough problems fast with these problem-solving techniques! ... 2022 as 6:44 am. Excellent. Reply. AQ — September 19, 2022 as 4:41 pm. Certainly wonderful ...
One of the best ways to improve your problem-solving skills is to learn from experts. Consider enrolling in organizational training, shadowing a mentor, or working with a coach. 2. Practice. Practice using your new problem-solving skills by applying them to smaller problems you might encounter in your daily life.
Problem-solving is a mental process that involves discovering, analyzing, and solving problems. The ultimate goal of problem-solving is to overcome obstacles and find a solution that best resolves the issue. The best strategy for solving a problem depends largely on the unique situation. In some cases, people are better off learning everything ...
In insight problem-solving, the cognitive processes that help you solve a problem happen outside your conscious awareness. 4. Working backward. Working backward is a problem-solving approach often ...
Problem-solving skills are the most sought-after soft skill of 2022. In fact, 86% of employers look for problem-solving skills on student resumes, according to the National Association of Colleges and Employers Job Outlook 2022 survey .
Problem 13. Let be a scalene triangle. Point lies on so that bisects The line through perpendicular to intersects the line through parallel to at point Suppose and What is . Solution. Problem 14. How many ways are there to split the integers through into pairs such that in each pair, the greater number is at least times the lesser number ...
6. Solution implementation. This is what we were waiting for! All problem solving strategies have the end goal of implementing a solution and solving a problem in mind. Remember that in order for any solution to be successful, you need to help your group through all of the previous problem solving steps thoughtfully.
The comprehensive nature of the list of problem solving strategies allows individuals to use a checklist approach to problem solving. It also could facilitate training others in problem solving. ... 2022 at 9:31 am Great job! Efficient strategies and very informative. jmalouff on January 14, 2022 at 9:47 am Thanks!
2022 AMC 8 problems and solutions. THE TEST WAS HELD BETWEEN JANUARY 18, 2022 AND JANUARY 24, 2022. ... Art of Problem Solving is an ACS WASC Accredited School. aops programs. AoPS Online. Beast Academy. AoPS Academy. About. About AoPS. Our Team. Our History. Jobs. AoPS Blog. Site Info. Terms.
26 Problem-Solving Products To Help You Fix Things You Didn't Know You Could Fix Yourself In 2022. This year, your motto is "I got this." by Katy Herman. BuzzFeed Staff. 1. Salicylic acid wart ...
PROBLEM: Your beloved cast iron pan is difficult to clean. SOLUTION: Wash off the grit AND preserve the flavor with soap-less, detergent-free grit removal. You don't need to fear your seasoning being stripped off by harsh soap or cleaners. With The Ringer, all you need is warm water and you're good to go. WATCH.
The world entered 2022 with growing weariness after two years of a global pandemic that has claimed 5.61 million lives, and continuing humanitarian and climate crises, with energy-related emissions set to rise by 87 million metric tonnes (about 96 million tons), and 274 million people in need of lifesaving humanitarian assistance.. None of these issues has simple fixes.
Problem-Solving: Arizona State University. Creative Thinking: Techniques and Tools for Success: Imperial College London. Solving Problems with Creative and Critical Thinking: IBM. Computer Science: Programming with a Purpose: Princeton University. Introduction to Mathematical Thinking: Stanford University. Problem Solving, Python Programming ...
In this episode of the McKinsey Podcast, Simon London speaks with Charles Conn, CEO of venture-capital firm Oxford Sciences Innovation, and McKinsey senior partner Hugo Sarrazin about the complexities of different problem-solving strategies.. Podcast transcript. Simon London: Hello, and welcome to this episode of the McKinsey Podcast, with me, Simon London.
Similar to how collaborative problem-solving influences attitudinal tendency, attitudinal tendency impacts cognitive skill when attempting to solve a problem (Liu et al., 2020; Zhang et al., 2022 ...
26 Products That Deserve An Award For All The Problems They'll Solve In 2022. Maybe in 2022, the CDC will print wallet-sized vaccine cards but until that happens, keeps yours safe with a cute vax ...
Creative problem-solving primarily operates in the ideate phase of design thinking but can be applied to others. This is because design thinking is an iterative process that moves between the stages as ideas are generated and pursued. This is normal and encouraged, as innovation requires exploring multiple ideas.
Discover what problem-solving is, and why it's important for managers. Understand the steps of the process and learn about seven problem-solving skills. ... Accessed December 6, 2022. Keep reading. Updated on Jan 5, 2024. Written by: C. Coursera Staff. Editorial Team. Coursera's editorial team is comprised of highly experienced professional ...
2022 PPSN 2022. 10-14 September; Dortmund, Germany; Parallel Problem Solving from Nature - PPSN XVII. 85 Papers. 2 Volumes. 2020 PPSN 2020. 5-9 September; ... Parallel Problem Solving from Nature - PPSN XIII. 93 Papers. 1 Volume. 2012 PPSN 2012. 1-5 September; Taormina, Italy; Parallel Problem Solving from Nature - PPSN XII. 105 Papers. 2 ...
Many employers have responded by investing more into mental health and well-being than ever before. Across the globe, four in five HR leaders report that mental health and well-being is a top priority for their organization. 3 McKinsey Health Institute Employee Mental Health and Wellbeing Survey, 2022: n (employee) = 14,509; n (HR decision maker) = 1,389.
2022 AMC 12B problems and solutions. The test was held on Wednesday, November 16, 2022. 2022 AMC 12B Problems. 2022 AMC 12B Answer Key. Problem 1.
Summary The 35th edition of the Annie E. Casey Foundation's KIDS COUNT ® Data Book examines the unprecedented declines in student math and reading proficiency brought on by the COVID-19 pandemic's effect on education.The latest data from the National Assessment of Educational Progress reveals that between 2019 and 2022, fourth-grade reading and eighth-grade math scores plummeted, representing ...
There is debate about whether complex problems should be addressed technocratically or whether they should be politicized. While many tend to favour technocratic decision-making and evidence based policy, for others politicization of policy problems is fundamental for significant policy change. But politicization does not always lead to problem solving. Nor is it always necessary. This paper ...
Our online AMC 10 Problem Series course has been instrumental preparation for thousands of top AMC 10 scorers over the past decade. LEARN MORE AMC 10 Problems and Solutions
2022 AIME II. 2022 AIME II problems and solutions. The test was held on Wednesday, February 16, 2022. The first link will contain the full set of test problems. The rest will contain each individual problem and its solution.
A-D, Adjusted means and standard errors from linear mixed models accounting for sociodemographic factors are visualized. F, A t score of 59 or less indicates nonclinical symptoms, a t score between 60 and 64 indicates that the child is at risk for problem behaviors, and a t score of 65 or greater indicates clinical symptoms.The t score of 60 is visually represented with a dashed blue line on ...