

What does the scholarly research say about the effect of gender transition on transgender well-being?
We conducted a systematic literature review of all peer-reviewed articles published in English between 1991 and June 2017 that assess the effect of gender transition on transgender well-being. We identified 55 studies that consist of primary research on this topic, of which 51 (93%) found that gender transition improves the overall well-being of transgender people, while 4 (7%) report mixed or null findings. We found no studies concluding that gender transition causes overall harm. As an added resource, we separately include 17 additional studies that consist of literature reviews and practitioner guidelines.
Bottom Line
This search found a robust international consensus in the peer-reviewed literature that gender transition, including medical treatments such as hormone therapy and surgeries, improves the overall well-being of transgender individuals. The literature also indicates that greater availability of medical and social support for gender transition contributes to better quality of life for those who identify as transgender.
Below are the 8 findings of our review, and links to the 72 studies on which they are based. Click here to view our methodology . Click here for a printer-friendly one-pager of this research analysis .
Suggested Citation : What We Know Project, Cornell University, “What Does the Scholarly Research Say about the Effect of Gender Transition on Transgender Well-Being?” (online literature review), 2018.
Research Findings
1. The scholarly literature makes clear that gender transition is effective in treating gender dysphoria and can significantly improve the well-being of transgender individuals.
2. Among the positive outcomes of gender transition and related medical treatments for transgender individuals are improved quality of life, greater relationship satisfaction, higher self-esteem and confidence, and reductions in anxiety, depression, suicidality, and substance use.
3. The positive impact of gender transition on transgender well-being has grown considerably in recent years, as both surgical techniques and social support have improved.
4. Regrets following gender transition are extremely rare and have become even rarer as both surgical techniques and social support have improved. Pooling data from numerous studies demonstrates a regret rate ranging from .3 percent to 3.8 percent. Regrets are most likely to result from a lack of social support after transition or poor surgical outcomes using older techniques.
5. Factors that are predictive of success in the treatment of gender dysphoria include adequate preparation and mental health support prior to treatment, proper follow-up care from knowledgeable providers, consistent family and social support, and high-quality surgical outcomes (when surgery is involved).
6. Transgender individuals, particularly those who cannot access treatment for gender dysphoria or who encounter unsupportive social environments, are more likely than the general population to experience health challenges such as depression, anxiety, suicidality and minority stress. While gender transition can mitigate these challenges, the health and well-being of transgender people can be harmed by stigmatizing and discriminatory treatment.
7. An inherent limitation in the field of transgender health research is that it is difficult to conduct prospective studies or randomized control trials of treatments for gender dysphoria because of the individualized nature of treatment, the varying and unequal circumstances of population members, the small size of the known transgender population, and the ethical issues involved in withholding an effective treatment from those who need it.
8. Transgender outcomes research is still evolving and has been limited by the historical stigma against conducting research in this field. More research is needed to adequately characterize and address the needs of the transgender population.
Below are 51 studies that found that gender transition improves the well-being of transgender people. Click here to jump to 4 studies that contain mixed or null findings on the effect of gender transition on transgender well-being. Click here to jump to 17 studies that consist of literature reviews or guidelines that help advance knowledge about the effect of gender transition on transgender well-being.
Ainsworth and spiegel, 2010.

Ainsworth, T., & Spiegel, J. (2010). Quality of life of individuals with and without facial feminization surgery or gender reassignment surgery. Quality of Life Research , 19 (7), 1019-1024.
Objectives: To determine the self-reported quality of life of male-to-female (MTF) transgendered individuals and how this quality of life is influenced by facial feminization and gender reassignment surgery. Methods: Facial Feminization Surgery outcomes evaluation survey and the SF-36v2 quality of life survey were administered to male-to-female transgender individuals via the Internet and on paper. A total of 247 MTF participants were enrolled in the study. Results: Mental health-related quality of life was statistically diminished (P < 0.05) in transgendered women without surgical intervention compared to the general female population and transwomen who had gender reassignment surgery (GRS), facial feminization surgery (FFS), or both. There was no statistically significant difference in the mental health-related quality of life among transgendered women who had GRS, FFS, or both. Participants who had FFS scored statistically higher (P < 0.01) than those who did not in the FFS outcomes evaluation. Conclusions: Transwomen have diminished mental health-related quality of life compared with the general female population. However, surgical treatments (e.g. FFS, GRS, or both) are associated with improved mental health-related quality of life.
Bailey, Ellis, & McNeil, 2014

Bailey, L., Ellis, S. J., & McNeil, J. (2014). Suicide risk in the UK trans population and the role of gender transition in decreasing suicidal ideation and suicide attempt. The Mental Health Review , 19 (4), 209-220.
Purpose: The purpose of this paper is to present findings from the Trans Mental Health Study (McNeil et al., 2012) – the largest survey of the UK trans population to date and the first to explore trans mental health and well-being within a UK context. Findings around suicidal ideation and suicide attempt are presented and the impact of gender dysphoria, minority stress and medical delay, in particular, are highlighted. Design/methodology/approach: This represents a narrative analysis of qualitative sections of a survey that utilised both open and closed questions. The study drew on a non-random sample (n 1⁄4 889), obtained via a range of UK-based support organisations and services. Findings: The study revealed high rates of suicidal ideation (84 per cent lifetime prevalence) and attempted suicide (48 per cent lifetime prevalence) within this sample. A supportive environment for social transition and timely access to gender reassignment, for those who required it, emerged as key protective factors. Subsequently, gender dysphoria, confusion/denial about gender, fears around transitioning, gender reassignment treatment delays and refusals, and social stigma increased suicide risk within this sample. Research limitations/implications: Due to the limitations of undertaking research with this population, the research is not demographically representative. Practical implications: The study found that trans people are most at risk prior to social and/or medical transition and that, in many cases, trans people who require access to hormones and surgery can be left unsupported for dangerously long periods of time. The paper highlights the devastating impact that delaying or denying gender reassignment treatment can have and urges commissioners and practitioners to prioritise timely intervention and support. Originality/value: The first exploration of suicidal ideation and suicide attempt within the UK trans population revealing key findings pertaining to social and medical transition, crucial for policy makers, commissioners and practitioners working across gender identity services, mental health services and suicide prevention.
Bar et al., 2016

Bar, M. A., Jarus, T., Wada, M., Rechtman, L., & Noy, E. (2016). Male-to-female transitions: Implications for occupational performance, health, and life satisfaction. The Canadian Journal of Occupational Therapy , 83 (2), 72-82.
Background. People who undergo a gender transition process experience changes in different everyday occupations. These changes may impact their health and life satisfaction. Purpose. This study examined the difference in the occupational performance history scales (occupational identity, competence, and settings) between male-to-female transgender women and cisgender women and the relation of these scales to health and life satisfaction. Method. Twenty-two transgender women and 22 matched cisgender women completed a demographic questionnaire and three reliable measures in this cross-sectional study. Data were analyzed using a two-way analysis of variance and multiple linear regressions. Findings. The results indicate lower performance scores for the transgender women. In addition, occupational settings and group membership (transgender and cisgender groups) were found to be predictors of life satisfaction. Implications. The present study supports the role of occupational therapy in promoting occupational identity and competence of transgender women and giving special attention to their social and physical environment.
Bodlund and Kullgren, 1996

Bodlund, O., & Kullgren, G. (1996). Transsexualism–general outcome and prognostic factors: A five-year follow-up study of nineteen transsexuals in the process of changing sex. Archives of Sexual Behavior , 25 (3), 303-316.
Nineteen transsexuals, approved for sex reassignement, were followed-up after 5 years. Outcome was evaluated as changes in seven areas of social, psychological, and psychiatric functioning. At baseline the patients were evaluated according to axis I, II, V (DSM-III-R), SCID screen, SASB (Structural Analysis of Social Behavior), and DMT (Defense Mechanism Test). At follow-up all but 1 were treated with contrary sex hormones, 12 had completed sex reassignment surgery, and 3 females were waiting for phalloplasty. One male transsexual regretted the decision to change sex and had quit the process. Two transsexuals had still not had any surgery due to older age or ambivalence. Overall, 68% (n = 13) had improved in at least two areas of functioning. In 3 cases (16%) outcome were judged as unsatisfactory and one of those regarded sex change as a failure. Another 3 patients were mainly unchanged after 5 years. Female transsexuals had a slightly better outcome, especially concerning establishing and maintaining partnerships and improvement in socio-economic status compared to male transsexuals. Baseline factors associated with negative outcome (unchanged or worsened) were presence of a personality disorder and high number of fulfilled axis II criteria. SCID screen assessments had high prognostic power. Negative self-image, according to SASB, predicted a negative outcome, whereas DMT variables were not correlated to outcome.
Bouman et al., 2016

Bouman, W. P., Claes, L., Marshall, E., Pinner, G. T., Longworth, J., et al. (2016). Sociodemographic variables, clinical features, and the role of preassessment cross-sex hormones in older trans people. The Journal of Sexual Medicine , 13 (4), 711-719.
Introduction: As referrals to gender identity clinics have increased dramatically over the last few years, no studies focusing on older trans people seeking treatment are available. Aims: The aim of this study was to investigate the sociodemographic and clinical characteristics of older trans people attending a national service and to investigate the influence of cross-sex hormones (CHT) on psychopathology. Methods: Individuals over the age of 50 years old referred to a national gender identity clinic during a 30-month period were invited to complete a battery of questionnaires to measure psychopathology and clinical characteristics. Individuals on cross-sex hormones prior to the assessment were compared with those not on treatment for different variables measuring psychopathology. Main Outcome Measures: Sociodemographic and clinical variables and measures of depression and anxiety (Hospital Anxiety and Depression Scale), self-esteem (Rosenberg Self-Esteem Scale), victimization (Experiences of Transphobia Scale), social support (Multidimensional Scale of Perceived Social Support), interpersonal functioning (Inventory of Interpersonal Problems), and nonsuicidal self-injury (Self-Injury Questionnaire). Results: The sex ratio of trans females aged 50 years and older compared to trans males was 23.7:1. Trans males were removed for the analysis due to their small number (n = 3). Participants included 71 trans females over the age of 50, of whom the vast majority were white, employed or retired, and divorced and had children. Trans females on CHT who came out as trans and transitioned at an earlier age were significantly less anxious, reported higher levels of self-esteem, and presented with fewer socialization problems. When controlling for socialization problems, differences in levels of anxiety but not self-esteem remained. Conclusion: The use of cross-sex hormones prior to seeking treatment is widespread among older trans females and appears to be associated with psychological benefits. Existing barriers to access CHT for older trans people may need to be re-examined.
Boza and Nicholson, 2014

Boza, C., & Nicholson Perry, K. (2014). Gender-related victimization, perceived social support, and predictors of depression among transgender Australians. International Journal Of Transgenderism , 15 (1), 35-52.
This study examined mental health outcomes, gender-related victimization, perceived social support, and predictors of depression among 243 transgender Australians (n= 83 assigned female at birth, n= 160 assigned male at birth). Overall, 69% reported at least 1 instance of victimization, 59% endorsed depressive symptoms, and 44% reported a previous suicide attempt. Social support emerged as the most significant predictor of depressive symptoms (p>.05), whereby persons endorsing higher levels of overall perceived social support tended to endorse lower levels of depressive symptoms. Second to social support, persons who endorsed having had some form of gender affirmative surgery were significantly more likely to present with lower symptoms of depression. Contrary to expectations, victimization did not reach significance as an independent risk factor of depression (p=.053). The pervasiveness of victimization, depression, and attempted suicide represents a major health concern and highlights the need to facilitate culturally sensitive health care provision.
Budge et al., 2013

Budge, S. L., Katz-Wise, S. L., Tebbe, E. N., Howard, K. A. S., Schneider, C. L., et al. (2013). Transgender emotional and coping processes: Facilitative and avoidant coping throughout gender transitioning. The Counseling Psychologist , 41 (4), 601-647.
Eighteen transgender-identified individuals participated in semi-structured interviews regarding emotional and coping processes throughout their gender transition. The authors used grounded theory to conceptualize and analyze the data. There were three distinct phases through which the participants described emotional and coping experiences: (a) pretransition, (b) during the transition, and (c) posttransition. Five separate themes emerged, including descriptions of coping mechanisms, emotional hardship, lack of support, positive social support, and affirmative emotional experiences. The authors developed a model to describe the role of coping mechanisms and support experienced throughout the transition process. As participants continued through their transitions, emotional hardships lessened and they used facilitative coping mechanisms that in turn led to affirmative emotional experiences. The results of this study are indicative of the importance of guiding transgender individuals through facilitative coping experiences and providing social support throughout the transition process. Implications for counselors and for future research are discussed.
Cardoso da Silva et al., 2016

Cardoso da Silva, D., Schwarz, K., Fontanari, A.M.V., Costa, A.B., Massuda, R., et al. (2016). WHOQOL-100 Before and after sex reassignment surgery in Brazilian male-to-female transsexual individuals. Journal of Sexual Medicine , 13 (6), 988-993.
Introduction: The 100-item World Health Organization Quality of Life Assessment (WHOQOL-100) evaluates quality of life as a subjective and multidimensional construct. Currently, particularly in Brazil, there are controversies concerning quality of life after sex reassignment surgery (SRS). Aim: To assess the impact of surgical interventions on quality of life of 47 Brazilian male-to-female transsexual individuals using the WHOQOL-100. Methods: This was a prospective cohort study using the WHOQOL-100 and sociodemographic questions for individuals diagnosed with gender identity disorder according to criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. The protocol was used when a transsexual person entered the ambulatory clinic and at least 12 months after SRS. Main Outcome Measures: Initially, improvement or worsening of quality of life was assessed using 6 domains and 24 facets. Subsequently, quality of life was assessed for individuals who underwent new surgical interventions and those who did not undergo these procedures 1 year after SRS. Results: The participants showed significant improvement after SRS in domains II (psychological) and IV (social relationships) of the WHOQOL-100. In contrast, domains I (physical health) and III (level of independence) were significantly worse after SRS. Individuals who underwent additional surgery had a decrease in quality of life reflected in domains II and IV. During statistical analysis, all results were controlled for variations in demographic characteristics, without significant results. Conclusion: The WHOQOL-100 is an important instrument to evaluate the quality of life of male-to-female transsexuals during different stages of treatment. SRS promotes the improvement of psychological aspects and social relationships. However, even 1 year after SRS, male-to-female transsexuals continue to report problems in physical health and difficulty in recovering their independence.
(Due to a citation error, this study was initially listed twice.)
Castellano et al., 2015

Castellano, E., Crespi, C., Dell’Aquila, R., Rosato, C., Catalano, V., et al. (2015). Quality of life and hormones after sex reassignment surgery. Journal of Endocrinological Investigation , 38 (12), 1373-1381.
Background: Transpeople often look for sex reassignment surgery (SRS) to improve their quality of life (QoL). The hormonal therapy has many positive effects before and after SRS. There are no studies about correlation between hormonal status and QoL after SRS. Aim: To gather information on QoL, quality of sexual life and body image in transpeople at least 2 years after SRS, to compare these results with a control group and to evaluate the relations between the chosen items and hormonal status. Subjects and methods: Data from 60 transsexuals and from 60 healthy matched controls were collected. Testosterone, estradiol, LH and World Health Organization Quality of Life (WHOQOL-100) self-reported questionnaire were evaluated. Student’s t test was applied to compare transsexuals and controls. Multiple regression model was applied to evaluate WHOQOL’s chosen items and LH. Results: The QoL and the quality of body image scores in transpeople were not statistically different from the matched control groups’ ones. In the sexual life subscale, transwomen’s scores were similar to biological women’s ones, whereas transmen’s scores were statistically lower than biological men’s ones (P = 0.003). The quality of sexual life scored statistically lower in transmen than in transwomen (P = 0.048). A significant inverse relationship between LH and body image and between LH and quality of sexual life was found. Conclusions: This study highlights general satisfaction after SRS. In particular, transpeople’s QoL turns out to be similar to Italian matched controls. LH resulted inversely correlated to body image and sexual life scores.
Colizzi, Costa, & Todarello, 2014

Colizzi, M., Costa, R. & Todarello, O. (2014). Transsexual patients’ psychiatric comorbidity and positive effect of cross-sex hormonal treatment on mental health: Results from a longitudinal study. Psychoneuroendocrinology , 39 , 65-73.
The aim of the present study was to evaluate the presence of psychiatric diseases/symptoms in transsexual patients and to compare psychiatric distress related to the hormonal intervention in a one year follow-up assessment. We investigated 118 patients before starting the hormonal therapy and after about 12 months. We used the SCID-I to determine major mental disorders and functional impairment. We used the Zung Self-Rating Anxiety Scale (SAS) and the Zung Self-Rating Depression Scale (SDS) for evaluating self-reported anxiety and depression. We used the Symptom Checklist 90-R (SCL-90-R) for assessing self-reported global psychological symptoms. Seventeen patients (14%) had a DSM-IV-TR axis I psychiatric comorbidity. At enrollment the mean SAS score was above the normal range. The mean SDS and SCL-90-R scores were on the normal range except for SCL-90-R anxiety subscale. When treated, patients reported lower SAS, SDS and SCL-90-R scores, with statistically significant differences. Psychiatric distress and functional impairment were present in a significantly higher percentage of patients before starting the hormonal treatment than after 12 months (50% vs. 17% for anxiety; 42% vs. 23% for depression; 24% vs. 11% for psychological symptoms; 23% vs. 10% for functional impairment). The results revealed that the majority of transsexual patients have no psychiatric comorbidity, suggesting that transsexualism is not necessarily associated with severe comorbid psychiatric findings. The condition, however, seemed to be associated with subthreshold anxiety/depression, psychological symptoms and functional impairment. Moreover, treated patients reported less psychiatric distress. Therefore, hormonal treatment seemed to have a positive effect on transsexual patients’ mental health.
Colizzi et al., 2013

Colizzi. M., Costa, R., Pace, V., & Todarello, O. (2013). Hormonal treatment reduces psychobiological distress in gender identity disorder, independently of the attachment style. The Journal of Sexual Medicine , 10 (12), 3049–3058.
Introduction: Gender identity disorder may be a stressful situation. Hormonal treatment seemed to improve the general health as it reduces psychological and social distress. The attachment style seemed to regulate distress in insecure individuals as they are more exposed to hypothalamic–pituitary–adrenal system dysregulation and subjective stress. Aim: The objectives of the study were to evaluate the presence of psychobiological distress and insecure attachment in transsexuals and to study their stress levels with reference to the hormonal treatment and the attachment pattern. Methods: We investigated 70 transsexual patients. We measured the cortisol levels and the perceived stress before starting the hormonal therapy and after about 12 months. We studied the representation of attachment in transsexuals by a backward investigation in the relations between them and their caregivers. Main Outcome Measures: We used blood samples for assessing cortisol awakening response (CAR); we used the Perceived Stress Scale for evaluating self‐reported perceived stress and the Adult Attachment Interview to determine attachment styles. Results: At enrollment, transsexuals reported elevated CAR; their values were out of normal. They expressed higher perceived stress and more attachment insecurity, with respect to normative sample data. When treated with hormone therapy, transsexuals reported significantly lower CAR (P < 0.001), falling within the normal range for cortisol levels. Treated transsexuals showed also lower perceived stress (P < 0.001), with levels similar to normative samples. The insecure attachment styles were associated with higher CAR and perceived stress in untreated transsexuals (P < 0.01). Treated transsexuals did not expressed significant differences in CAR and perceived stress by attachment. Conclusion: Our results suggested that untreated patients suffer from a higher degree of stress and that attachment insecurity negatively impacts the stress management. Initiating the hormonal treatment seemed to have a positive effect in reducing stress levels, whatever the attachment style may be.
Colton-Meier et al., 2011

Colton-Meier, S. L., Fitzgerald, K. M., Pardo, S. T., & Babcock, J. (2011). The effects of hormonal gender affirmation treatment on mental health in female-to-male transsexuals. Journal of Gay & Lesbian Mental Health , 15 (3), 281-299.
Hormonal interventions are an often-sought option for transgender individuals seeking to medically transition to an authentic gender. Current literature stresses that the effects and associated risks of hormone regimens should be monitored and well understood by health care providers (Feldman & Bockting, 2003). However, the positive psychological effects following hormone replacement therapy as a gender affirming treatment have not been adequately researched. This study examined the relationship of hormone replacement therapy, specifically testosterone, with various mental health outcomes in an Internet sample of more than 400 self-identified female-to-male transsexuals. Results of the study indicate that female-to-male transsexuals who receive testosterone have lower levels of depression, anxiety, and stress, and higher levels of social support and health related quality of life. Testosterone use was not related to problems with drugs, alcohol, or suicidality. Overall findings provide clear evidence that HRT is associated with improved mental health outcomes in female-to-male transsexuals.
Costantino et al., 2013

Costantino, A., Cerpolini, S., Alvisi, S., Morselli, P. G., Venturoli, S., & Meriggiola, M. C. (2013). A prospective study on sexual function and mood in female-to-male transsexuals during testosterone administration and after sex reassignment surgery. Journal of Sex & Marital Therapy , 39 (4), 321-335.
Testosterone administration in female-to-male transsexual subjects aims to develop and maintain the characteristics of the desired sex. Very little data exists on its effects on sexuality of female-to-male transsexuals. The aim of this study was to evaluate sexual function and mood of female-to-male transsexuals from their first visit, throughout testosterone administration and after sex reassignment surgery. Participants were 50 female-to-male transsexual subjects who completed questionnaires assessing sexual parameters and mood. The authors measured reproductive hormones and hematological parameters. The results suggest a positive effect of testosterone treatment on sexual function and mood in female-to-male transsexual subjects.
Davis and Meier, 2014

Davis, S. A. & Meier, S. C. (2014). Effects of testosterone treatment and chest reconstruction surgery on mental health and sexuality in female-to-male transgender people. International Journal of Sexual Health , 26 (2), 113-128.
Objectives: This study examined the effects of testosterone treatment with or without chest reconstruction surgery (CRS) on mental health in female-to-male transgender people (FTMs). Methods: More than 200 FTMs completed a written survey including quantitative scales to measure symptoms of anxiety and depression, feelings of anger, and body dissatisfaction, as well as qualitative questions assessing shifts in sexuality after the initiation of testosterone. Fifty-seven percent of participants were taking testosterone and 40% had undergone CRS. Results: Cross-sectional analysis using a between-subjects multivariate analysis of variance showed that participants who were receiving testosterone endorsed fewer symptoms of anxiety and depression as well as less anger than the untreated group. Participants who had CRS in addition to testosterone reported less body dissatisfaction than both the testosterone-only or the untreated groups. Furthermore, participants who were injecting testosterone on a weekly basis showed significantly less anger compared with those injecting every other week. In qualitative reports, more than 50% of participants described increased sexual attraction to nontransgender men after taking testosterone. Conclusions: Results indicate that testosterone treatment in FTMs is associated with a positive effect on mental health on measures of depression, anxiety, and anger, while CRS appears to be more important for the alleviation of body dissatisfaction. The findings have particular relevance for counselors and health care providers serving FTM and gender-variant people considering medical gender transition.
De Cuypere et al., 2006

De Cuypere, G., Elaut, E., Heylens, G., Maele, G. V., Selvaggi, G., et al. (2006). Long-term follow-up: Psychosocial outcome of Belgian transsexuals after sex reassignment surgery. Sexologies , 15 (2), 126-133.
Background: To establish the benefit of sex reassignment surgery (SRS) for persons with a gender identity disorder, follow-up studies comprising large numbers of operated transsexuals are still needed. Aims: The authors wanted to assess how the transsexuals who had been treated by the Ghent multidisciplinary gender team since 1985, were functioning psychologically, socially and professionally after a longer period. They also explored some prognostic factors with a view to refining the procedure. Method: From 107 Dutch-speaking transsexuals who had undergone SRS between 1986 and 2001, 62 (35 male-to-females and 27 female-to-males) completed various questionnaires and were personally interviewed by researchers, who had not been involved in the subjects’ initial assessment or treatment. Results: On the GAF (DSM-IV) scale the female-to-male transsexuals scored significantly higher than the male-to-females (85.2 versus 76.2). While no difference in psychological functioning (SCL-90) was observed between the study group and a normal population, subjects with a pre-existing psychopathology were found to have retained more psychological symptoms. The subjects proclaimed an overall positive change in their family and social life. None of them showed any regrets about the SRS. A homosexual orientation, a younger age when applying for SRS, and an attractive physical appearance were positive prognostic factors. Conclusion: While sex reassignment treatment is an effective therapy for transsexuals, also in the long term, the postoperative transsexual remains a fragile person in some respects.
Dhejne et al., 2014

Dhejne, C., Öberg, K., Arver, S., & Landén, M. (2014). An analysis of all applications for sex reassignment surgery in sweden, 1960-2010: Prevalence, incidence, and regrets. Archives of Sexual Behavior , 43 (8), 1535-1545.
Incidence and prevalence of applications in Sweden for legal and surgical sex reassignment were examined over a 50-year period (1960-2010), including the legal and surgical reversal applications. A total of 767 people (289 natal females and 478 natal males) applied for legal and surgical sex reassignment. Out of these, 89 % (252 female-to-males [FM] and 429 male-to-females [MF]) received a new legal gender and underwent sex reassignment surgery (SRS). A total of 25 individuals (7 natal females and 18 natal males), equaling 3.3 %, were denied a new legal gender and SRS. The remaining withdrew their application, were on a waiting list for surgery, or were granted partial treatment. The incidence of applications was calculated and stratified over four periods between 1972 and 2010. The incidence increased significantly from 0.16 to 0.42/100,000/year (FM) and from 0.23 to 0.73/100,000/year (MF). The most pronounced increase occurred after 2000. The proportion of FM individuals 30 years or older at the time of application remained stable around 30 %. In contrast, the proportion of MF individuals 30 years or older increased from 37 % in the first decade to 60 % in the latter three decades. The point prevalence at December 2010 for individuals who applied for a new legal gender was for FM 1:13,120 and for MF 1:7,750. The FM:MF sex ratio fluctuated but was 1:1.66 for the whole study period. There were 15 (5 MF and 10 MF) regret applications corresponding to a 2.2 % regret rate for both sexes. There was a significant decline of regrets over the time period.
Eldh, Berg, & Gustafsson, 1997

Eldh, J., Berg, A., Gustafsson, M. (1997). Long-term follow up after sex reassignment surgery. Scandinavian Journal of Plastic and Reconstructive Surgery and Hand Surgery , 27 (1), 39-45.
A long-term follow up of 136 patients operated on for sex reassignment was done to evaluate the surgical outcome. Social and psychological adjustments were also investigated by a questionnaire in 90 of these 136 patients. Optimal results of the operation are essential for a successful outcome. Personal and social instability before operation, unsuitable body build, and age over 30 years at operation correlated with unsatisfactory results. Adequate family and social support is important for postoperative functioning. Sex reassignment had no influence on the person’s ability to work.
Fisher et al., 2014

Fisher, A. D., Castellini, G., Bandini, E., Casale, H., Fanni, E., et al. (2014). Cross‐sex hormonal treatment and body uneasiness in individuals with gender dysphoria. The Journal of Sexual Medicine , 11 (3), 709–719.
Introduction: Cross‐sex hormonal treatment (CHT) used for gender dysphoria (GD) could by itself affect well‐being without the use of genital surgery; however, to date, there is a paucity of studies investigating the effects of CHT alone. Aims: This study aimed to assess differences in body uneasiness and psychiatric symptoms between GD clients taking CHT and those not taking hormones (no CHT). A second aim was to assess whether length of CHT treatment and daily dose provided an explanation for levels of body uneasiness and psychiatric symptoms. Methods: A consecutive series of 125 subjects meeting the criteria for GD who not had genital reassignment surgery were considered. Main Outcome Measures: Subjects were asked to complete the Body Uneasiness Test (BUT) to explore different areas of body‐related psychopathology and the Symptom Checklist‐90 Revised (SCL‐90‐R) to measure psychological state. In addition, data on daily hormone dose and length of hormonal treatment (androgens, estrogens, and/or antiandrogens) were collected through an analysis of medical records. Results: Among the male‐to‐female (MtF) individuals, those using CHT reported less body uneasiness compared with individuals in the no‐CHT group. No significant differences were observed between CHT and no‐CHT groups in the female‐to‐male (FtM) sample. Also, no significant differences in SCL score were observed with regard to gender (MtF vs. FtM), hormone treatment (CHT vs. no‐CHT), or the interaction of these two variables. Moreover, a two‐step hierarchical regression showed that cumulative dose of estradiol (daily dose of estradiol times days of treatment) and cumulative dose of androgen blockers (daily dose of androgen blockers times days of treatment) predicted BUT score even after controlling for age, gender role, cosmetic surgery, and BMI. Conclusions: The differences observed between MtF and FtM individuals suggest that body‐related uneasiness associated with GD may be effectively diminished with the administration of CHT even without the use of genital surgery for MtF clients. A discussion is provided on the importance of controlling both length and daily dose of treatment for the most effective impact on body uneasiness.
Glynn et al., 2016

Glynn, T. R., Gamarel, K. E., Kahler, C. W., Iwamoto, M., Operario, D., & Nemoto, T. (2016). The role of gender affirmation in psychological well-being among transgender women. Psychology Of Sexual Orientation And Gender Diversity , 3 (3), 336-344.
High prevalence of psychological distress, including greater depression, lower self-esteem, and suicidal ideation, has been documented across numerous samples of transgender women and has been attributed to high rates of discrimination and violence. According to the gender affirmation framework (Sevelius, 2013), access to sources of gender-affirmative support can offset such negative psychological effects of social oppression. However, critical questions remain unanswered in regards to how and which aspects of gender affirmation are related to psychological well-being. The aims of this study were to investigate the associations among 3 discrete areas of gender affirmation (psychological, medical, and social) and participants’ reports of psychological well-being. A community sample of 573 transgender women with a history of sex work completed a 1-time self-report survey that assessed demographic characteristics, gender affirmation, and mental health outcomes. In multivariate models, we found that social, psychological, and medical gender affirmation were significant predictors of lower depression and higher self-esteem whereas no domains of affirmation were significantly associated with suicidal ideation. Findings support the need for accessible and affordable transitioning resources for transgender women to promote better quality of life among an already vulnerable population. However, transgender individuals should not be portrayed simplistically as objects of vulnerability, and research identifying mechanisms to promote wellness and thriving is necessary for future intervention development. As the gender affirmation framework posits, the personal experience of feeling affirmed as a transgender person results from individuals’ subjective perceptions of need along multiple dimensions of gender affirmation. Thus, personalized assessment of gender affirmation may be a useful component of counseling and service provision for transgender women.
Gomez-Gil et al., 2012

Gomez-Gil, E., Zubiaurre-Elorz, L., Esteva, I., Guillamon, A., Godas, T., Cruz Almaraz, M., Halperin, I., Salamero, M. (2012). Hormone-treated transsexuals report less social distress, anxiety and depression. Psychoneuroendocrinology , 37 (5), 662-670.
Introduction: The aim of the present study was to evaluate the presence of symptoms of current social distress, anxiety and depression in transsexuals. Methods: We investigated a group of 187 transsexual patients attending a gender identity unit; 120 had undergone hormonal sex-reassignment (SR) treatment and 67 had not. We used the Social Anxiety and Distress Scale (SADS) for assessing social anxiety and the Hospital Anxiety and Depression Scale (HADS) for evaluating current depression and anxiety. Results: The mean SADS and HADS scores were in the normal range except for the HAD-Anxiety subscale (HAD-A) on the non-treated transsexual group. SADS, HAD-A, and HAD-Depression (HAD-D) mean scores were significantly higher among patients who had not begun cross-sex hormonal treatment compared with patients in hormonal treatment (F = 4.362, p = .038; F = 14.589, p = .001; F = 9.523, p = .002 respectively). Similarly, current symptoms of anxiety and depression were present in a significantly higher percentage of untreated patients than in treated patients (61% vs. 33% and 31% vs. 8% respectively). Conclusions: The results suggest that most transsexual patients attending a gender identity unit reported subclinical levels of social distress, anxiety, and depression. Moreover, patients under cross-sex hormonal treatment displayed a lower prevalence of these symptoms than patients who had not initiated hormonal therapy. Although the findings do not conclusively demonstrate a direct positive effect of hormone treatment in transsexuals, initiating this treatment may be associated with better mental health of these patients.
Gomez-Gil et al., 2014

Gómez-Gil, E., Zubiaurre-Elorza, L., de Antonio, E. D., Guillamon, A., & Salamero, M. (2014). Determinants of quality of life in Spanish transsexuals attending a gender unit before genital sex reassignment surgery. Quality of Life Research , 23 (2), 669-676.
Purpose: To evaluate the self-reported perceived quality of life (QoL) in transsexuals attending a Spanish gender identity unit before genital sex reassignment surgery, and to identify possible determinants that likely contribute to their QoL. Methods: A sample of 119 male-to-female (MF) and 74 female-to-male (FM) transsexuals were included in the study. The WHOQOL-BREF scale was used to evaluate self-reported QoL. Possible determinants included age, sex, education, employment, partnership status, undergoing cross-sex hormonal therapy, receiving at least one non-genital sex reassignment surgery, and family support (assessed with the family APGAR questionnaire). Results: Mean scores of all QoL domains ranged from 55.44 to 63.51. Linear regression analyses revealed that undergoing cross-sex hormonal treatment, having family support, and having an occupation were associated with a better QoL for all transsexuals. FM transsexuals have higher social domain QoL scores than MF transsexuals. The model accounts for 20.6 % of the variance in the physical, 32.5 % in the psychological, 21.9 % in the social, and 20.1 % in the environment domains, and 22.9 % in the global QoL factor. Conclusions: Cross-sex hormonal treatment, family support, and working or studying are linked to a better self-reported QoL in transsexuals. Healthcare providers should consider these factors when planning interventions to promote the health-related QoL of transsexuals.
Gorin-Lazard et al., 2012

Gorin‐Lazard, A., Baumstarck, K., Boyer, L., Maquigneau, A., Gebleux, S., Penochet, J., Pringuey, D., Albarel, F., Morange, I., Loundou, A., Berbis, J., Auquier, P., Lançon, C. and Bonierbale, M. (2012). Is hormonal therapy associated with better quality of life in transsexuals? A cross‐sectional study. The Journal of Sexual Medicine , 9 (2), 531–541.
Introduction: Although the impact of sex reassignment surgery on the self‐reported outcomes of transsexuals has been largely described, the data available regarding the impact of hormone therapy on the daily lives of these individuals are scarce. Aims: The objectives of this study were to assess the relationship between hormonal therapy and the self‐reported quality of life (QoL) in transsexuals while taking into account the key confounding factors and to compare the QoL levels between transsexuals who have, vs. those who have not, undergone cross‐sex hormone therapy as well as between transsexuals and the general population (French age‐ and sex‐matched controls). Methods: This study incorporated a cross‐sectional design that was conducted in three psychiatric departments of public university teaching hospitals in France. The inclusion criteria were as follows: 18 years or older, diagnosis of gender identity disorder (302.85) according to the Diagnostic and Statistical Manual, fourth edition text revision (DSM‐IV TR), inclusion in a standardized sex reassignment procedure following the agreement of a multidisciplinary team, and pre‐sex reassignment surgery. Main Outcome Measure. QoL was assessed using the Short Form 36 (SF‐36). Results: The mean age of the total sample was 34.7 years, and the sex ratio was 1:1. Forty‐four (72.1%) of the participants received hormonal therapy. Hormonal therapy and depression were independent predictive factors of the SF‐36 mental composite score. Hormonal therapy was significantly associated with a higher QoL, while depression was significantly associated with a lower QoL. Transsexuals’ QoL, independently of hormonal status, did not differ from the French age‐ and sex‐matched controls except for two subscales of the SF‐36 questionnaire: role physical (lower scores in transsexuals) and general health (lower scores in controls). Conclusion: The present study suggests a positive effect of hormone therapy on transsexuals’ QoL after accounting for confounding factors. These results will be useful for healthcare providers of transgender persons but should be confirmed with larger samples using a prospective study design.
Gorin-Lazard et al., 2013

Gorin-Lazard, A., Baumstarck, K., Boyer, L., Maquigneau, A., Penochet, J. C., et al. (2013). Hormonal therapy is associated with better self-esteem, mood, and quality of life in transsexuals. Journal of Nervous and Mental Disease , 201 (11), 996–1000.
Few studies have assessed the role of cross-sex hormones on psychological outcomes during the period of hormonal therapy preceding sex reassignment surgery in transsexuals. The objective of this study was to assess the relationship between hormonal therapy, self-esteem, depression, quality of life (QoL), and global functioning. This study incorporated a cross-sectional design. The inclusion criteria were diagnosis of gender identity disorder (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision) and inclusion in a standardized sex reassignment procedure. The outcome measures were self-esteem (Social Self-Esteem Inventory), mood (Beck Depression Inventory), QoL (Subjective Quality of Life Analysis), and global functioning (Global Assessment of Functioning). Sixty-seven consecutive individuals agreed to participate. Seventy-three percent received hormonal therapy. Hormonal therapy was an independent factor in greater self-esteem, less severe depression symptoms, and greater “psychological-like” dimensions of QoL. These findings should provide pertinent information for health care providers who consider this period as a crucial part of the global sex reassignment procedure.
Hess et al., 2014

Hess, J., Neto, R. R., Panic, L., Rübben, H., & Senf, W. (2014). Satisfaction with male-to-female gender reassignment surgery: Results of a retrospective analysis. Deutsches Ärzteblatt International , 111 (47), 795–801.
Background: The frequency of gender identity disorder is hard to determine; the number of gender reassignment operations and of court proceedings in accordance with the German Law on Transsexuality almost certainly do not fully reflect the underlying reality. There have been only a few studies on patient satisfaction with male-to-female gender reassignment surgery. Methods: 254 consecutive patients who had undergone male-to-female gender reassignment surgery at Essen University Hospital’s Department of Urology retrospectively filled out a questionnaire about their subjective postoperative satisfaction. Results: 119 (46.9%) of the patients filled out and returned the questionnaires, at a mean of 5.05 years after surgery (standard deviation 1.61 years, range 1–7 years). 90.2% said their expectations for life as a woman were fulfilled postoperatively. 85.4% saw themselves as women. 61.2% were satisfied, and 26.2% very satisfied, with their outward appearance as a woman; 37.6% were satisfied, and 34.4% very satisfied, with the functional outcome. 65.7% said they were satisfied with their life as it is now. Conclusion: The very high rates of subjective satisfaction and the surgical outcomes indicate that gender reassignment surgery is beneficial. These findings must be interpreted with caution, however, because fewer than half of the questionnaires were returned.
Heylens et al., 2014

Heylens, G., Verroken, C., De Cock, S., T’Sjoen, G., & De Cuypere, G. (2014). Effects of different steps in gender reassignment therapy on psychopathology: a prospective study of persons with a gender identity disorder. The Journal of Sexual Medicine , 11 (1), 119–126.
Introduction: At the start of gender reassignment therapy, persons with a gender identity disorder (GID) may deal with various forms of psychopathology. Until now, a limited number of publications focus on the effect of the different phases of treatment on this comorbidity and other psychosocial factors. Aims: The aim of this study was to investigate how gender reassignment therapy affects psychopathology and other psychosocial factors. Methods: This is a prospective study that assessed 57 individuals with GID by using the Symptom Checklist‐90 (SCL‐90) at three different points of time: at presentation, after the start of hormonal treatment, and after sex reassignment surgery (SRS). Questionnaires on psychosocial variables were used to evaluate the evolution between the presentation and the postoperative period. The data were statistically analyzed by using SPSS 19.0, with significance levels set at P < 0.05. Main Outcome Measures: The psychopathological parameters include overall psychoneurotic distress, anxiety, agoraphobia, depression, somatization, paranoid ideation/psychoticism, interpersonal sensitivity, hostility, and sleeping problems. The psychosocial parameters consist of relationship, living situation, employment, sexual contacts, social contacts, substance abuse, and suicide attempt. Results: A difference in SCL‐90 overall psychoneurotic distress was observed at the different points of assessments (P = 0.003), with the most prominent decrease occurring after the initiation of hormone therapy (P < 0.001). Significant decreases were found in the subscales such as anxiety, depression, interpersonal sensitivity, and hostility. Furthermore, the SCL‐90 scores resembled those of a general population after hormone therapy was initiated. Analysis of the psychosocial variables showed no significant differences between pre‐ and postoperative assessments. Conclusions: A marked reduction in psychopathology occurs during the process of sex reassignment therapy, especially after the initiation of hormone therapy.
Imbimbo et al., 2009

Imbimbo, C., Verze, P., Palmieri, A., Longo, N., Fusco, F., Arcaniolo, D., & Mirone, V. (2009). A report from a single institute’s 14-year experience in treatment of male-to-female transsexuals. The Journal of Sexual Medicine , 6 (10), 2736–2745.
Introduction: Gender identity disorder or transsexualism is a complex clinical condition, and prevailing social context strongly impacts the form of its manifestations. Sex reassignment surgery (SRS) is the crucial step of a long and complex therapeutic process starting with preliminary psychiatric evaluation and culminating in definitive gender identity conversion. Aim: The aim of our study is to arrive at a clinical and psychosocial profile of male-to-female transsexuals in Italy through analysis of their personal and clinical experience and evaluation of their postsurgical satisfaction levels SRS. Methods: From January 1992 to September 2006, 163 male patients who had undergone gender-transforming surgery at our institution were requested to complete a patient satisfaction questionnaire. Main Outcome Measures: The questionnaire consisted of 38 questions covering nine main topics: general data, employment status, family status, personal relationships, social and cultural aspects, presurgical preparation, surgical procedure, and postsurgical sex life and overall satisfaction. Results: Average age was 31 years old. Seventy-two percent had a high educational level, and 63% were steadily employed. Half of the patients had contemplated suicide at some time in their lives before surgery and 4% had actually attempted suicide. Family and colleague emotional support levels were satisfactory. All patients had been adequately informed of surgical procedure beforehand. Eighty-nine percent engaged in postsurgical sexual activities. Seventy-five percent had a more satisfactory sex life after SRS, with main complications being pain during intercourse and lack of lubrication. Seventy-eight percent were satisfied with their neovagina’s esthetic appearance, whereas only 56% were satisfied with depth. Almost all of the patients were satisfied with their new sexual status and expressed no regrets. Conclusions: Our patients’ high level of satisfaction was due to a combination of a well-conducted preoperative preparation program, competent surgical skills, and consistent postoperative follow-up.
Johansson et al., 2010

Johansson, A., Sundbom, E., Höjerback, T., & Bodlund, O. (2010). A five-year follow-up study of Swedish adults with gender identity disorder. Archives of Sexual Behavior , 39 (6), 1429-1437.
This follow-up study evaluated the outcome of sex reassignment as viewed by both clinicians and patients, with an additional focus on the outcome based on sex and subgroups. Of a total of 60 patients approved for sex reassignment, 42 (25 male-to-female [MF] and 17 female-to-male [FM]) transsexuals completed a follow-up assessment after 5 or more years in the process or 2 or more years after completed sex reassignment surgery. Twenty-six (62%) patients had an early onset and 16 (38%) patients had a late onset; 29 (69%) patients had a homosexual sexual orientation and 13 (31%) patients had a non-homosexual sexual orientation (relative to biological sex). At index and follow-up, a semi-structured interview was conducted. At follow-up, 32 patients had completed sex reassignment surgery, five were still in process, and five—following their own decision—had abstained from genital surgery. No one regretted their reassignment. The clinicians rated the global outcome as favorable in 62% of the cases, compared to 95% according to the patients themselves, with no differences between the subgroups. Based on the follow-up interview, more than 90% were stable or improved as regards work situation, partner relations, and sex life, but 5–15% were dissatisfied with the hormonal treatment, results of surgery, total sex reassignment procedure, or their present general health. Most outcome measures were rated positive and substantially equal for MF and FM. Late-onset transsexuals differed from those with early onset in some respects: these were mainly MF (88 vs. 42%), older when applying for sex reassignment (42 vs. 28 years), and non-homosexually oriented (56 vs. 15%). In conclusion, almost all patients were satisfied with the sex reassignment; 86% were assessed by clinicians at follow-up as stable or improved in global functioning.
Keo-Meier et al., 2015

Keo-Meier, C. L., Herman, L. I., Reisner, S. L., Pardo, S. T., Sharp, C., & Babcock, J. C. (2015). Testosterone treatment and MMPI-2 improvement in transgender men: A prospective controlled study. Journal of Consulting and Clinical Psychology, 83 , 143-156.
Objective: Most transgender men desire to receive testosterone treatment in order to masculinize their bodies. In this study, we aimed to investigate the short-term effects of testosterone treatment on psychological functioning in transgender men. This is the 1st controlled prospective follow-up study to examine such effects. Method: We examined a sample of transgender men (n = 48) and nontransgender male (n = 53) and female (n = 62) matched controls (mean age = 26.6 years; 74% White). We asked participants to complete the Minnesota Multiphasic Personality Inventory (2nd ed., or MMPI–2; Butcher, Graham, Tellegen, Dahlstrom, & Kaemmer, 2001) to assess psychological functioning at baseline and at the acute posttreatment follow-up (3 months after testosterone initiation). Regression models tested (a) Gender × Time interaction effects comparing divergent mean response profiles across measurements by gender identity; (b) changes in psychological functioning scores for acute postintervention measurements, adjusting for baseline measures, comparing transgender men with their matched nontransgender male and female controls and adjusting for baseline scores; and (c) changes in meeting clinical psychopathological thresholds. Results: Statistically significant changes in MMPI–2 scale scores were found at 3-month follow-up after initiating testosterone treatment relative to baseline for transgender men compared with female controls (female template): reductions in Hypochondria (p < .05), Depression (p < .05), Hysteria (p < .05), and Paranoia (p < .01); and increases in Masculinity–Femininity scores (p < .01). Gender × Time interaction effects were found for Hysteria (p < .05) and Paranoia (p < .01) relative to female controls (female template) and for Hypochondria (p < .05), Depression (p < .01), Hysteria (p < .01), Psychopathic Deviate (p < .05), Paranoia (p < .01), Psychasthenia (p < .01), and Schizophrenia (p < .01) compared with male controls (male template). In addition, the proportion of transgender men presenting with co-occurring psychopathology significantly decreased from baseline compared with 3-month follow-up relative to controls (p < .05). Conclusions: Findings suggest that testosterone treatment resulted in increased levels of psychological functioning on multiple domains in transgender men relative to nontransgender controls. These findings differed in comparisons of transgender men with female controls using the female template and with male controls using the male template. No iatrogenic effects of testosterone were found. These findings suggest a direct positive effect of 3 months of testosterone treatment on psychological functioning in transgender men.
Kraemer et al., 2008

Kraemer, B., Delsignore, A., Schnyder, U., & Hepp, U. (2008). Body image and transsexualism. Psychopathology , 41 (2), 96-100.
Background: To achieve a detailed view of the body image of transsexual patients, an assessment of perception, attitudes and experiences about one’s own body is necessary. To date, research on the body image of transsexual patients has mostly covered body dissatisfaction with respect to body perception. Sampling and Methods: We investigated 23 preoperative (16 male-to-female and 7 female-to-male transsexual patients) and 22 postoperative (14 male-to-female and 8 female-to-male) transsexual patients using a validated psychological measure for body image variables. Results: We found that preoperative transsexual patients were insecure and felt unattractive because of concerns about their body image. However, postoperative transsexual patients scored high on attractiveness and self-confidence. Furthermore, postoperative transsexual patients showed low scores for insecurity and concerns about their body. Conclusions: Our results indicate an improvement of body image concerns for transsexual patients following standards of care for gender identity disorder. Follow-up studies are recommended to confirm the assumed positive outcome of standards of care on body image.
Landen et al., 1998

Landén, M., Wålinder, J., Hambert, G., & Lundström, B. (1998). Factors predictive of regret in sex reassignment. Acta Psychiatrica Scandinavica , 97 (4), 284-289.
The objective of this study was to evaluate the features and calculate the frequency of sex-reassigned subjects who had applied for reversal to their biological sex, and to compare these with non-regretful subjects. An inception cohort was retrospectively identified consisting of all subjects with gender identity disorder who were approved for sex reassignment in Sweden during the period 1972-1992. The period of time that elapsed between the application and this evaluation ranged from 4 to 24 years. The total cohort consisted of 218 subjects. The results showed that 3.8% of the patients who were sex reassigned during 1972-1992 regretted the measures taken. The cohort was subdivided according to the presence or absence of regret of sex reassignment, and the two groups were compared. The results of logistic regression analysis indicated that two factors predicted regret of sex reassignment, namely lack of support from the patient’s family, and the patient belonging to the non-core group of transsexuals. In conclusion, the results show that the outcome of sex reassignment has improved over the years. However, the identified risk factors indicate the need for substantial efforts to support the families and close friends of candidates for sex reassignment.
Lawrence, 2003

Lawrence, A. A. (2003). Factors associated with satisfaction or regret following male-to-female sex reassignment surgery. Archives of Sexual Behavior , 32 (4), 299-315.
This study examined factors associated with satisfaction or regret following sex reassignment surgery (SRS) in 232 male-to-female transsexuals operated on between 1994 and 2000 by one surgeon using a consistent technique. Participants, all of whom were at least 1-year postoperative, completed a written questionnaire concerning their experiences and attitudes. Participants reported overwhelmingly that they were happy with their SRS results and that SRS had greatly improved the quality of their lives. None reported outright regret and only a few expressed even occasional regret. Dissatisfaction was most strongly associated with unsatisfactory physical and functional results of surgery. Most indicators of transsexual typology, such as age at surgery, previous marriage or parenthood, and sexual orientation, were not significantly associated with subjective outcomes. Compliance with minimum eligibility requirements for SRS specified by the Harry Benjamin International Gender Dysphoria Association was not associated with more favorable subjective outcomes. The physical results of SRS may be more important than preoperative factors such as transsexual typology or compliance with established treatment regimens in predicting postoperative satisfaction or regret.
Lawrence, 2006

Lawrence, A. A. (2006). Patient-reported complications and functional outcomes of male-to-female sex reassignment surgery. Archives of Sexual Behavior , 35 (6), 717-727.
This study examined preoperative preparations, complications, and physical and functional outcomes of male-to-female sex reassignment surgery (SRS), based on reports by 232 patients, all of whom underwent penile-inversion vaginoplasty and sensate clitoroplasty, performed by one surgeon using a consistent technique. Nearly all patients discontinued hormone therapy before SRS and most reported that doing so created no difficulties. Preoperative electrolysis to remove genital hair, undergone by most patients, was not associated with less serious vaginal hair problems. No patients reported rectal-vaginal fistula or deep-vein thrombosis and reports of other significant surgical complications were uncommon. One third of patients, however, reported urinary stream problems. No single complication was significantly associated with regretting SRS. Satisfaction with most physical and functional outcomes of SRS was high; participants were least satisfied with vaginal lubrication, vaginal touch sensation, and vaginal erotic sensation. Frequency of achieving orgasm after SRS was not significantly associated with most general measures of satisfaction. Later years of surgery, reflecting greater surgeon experience, were not associated with lower prevalence rates for most complications or with better ratings for most physical and functional outcomes of SRS.
Lobato et al., 2006

Lobato M. I., Koff, W. J., Manenti, C., da Fonseca Seger, D., Salvador, J., et al. (2006). Follow-up of sex reassignment surgery in transsexuals: a Brazilian cohort. Archives of Sexual Behavior, 35(6) , 711–715.
This study examined the impact of sex reassignment surgery on the satisfaction with sexual experience, partnerships, and relationship with family members in a cohort of Brazilian transsexual patients. A group of 19 patients who received sex reassignment between 2000 and 2004 (18 male- to-female, 1 female-to-male) after a two-year evaluation by a multidisciplinary team, and who agreed to participate in the study, completed a written questionnaire. Mean age at entry into the program was 31.21 ± 8.57 years and mean schooling was 9.2 ± 1.4 years. None of the patients reported regret for having undergone the surgery. Sexual experience was considered to have improved by 83.3% of the patients, and became more frequent for 64.7% of the patients. For 83.3% of the patients, sex was considered to be pleasurable with the neovagina/neopenis. In addition, 64.7% reported that initiating and maintaining a relationship had become easier. The number of patients with a partner increased from 52.6% to 73.7%. Family relationships improved in 26.3% of the cases, whereas 73.7% of the patients did not report a difference. None of the patients reported worse relationships
Manieri et al., 2014

Manieri, C., Castellano, E., Crespi, C., Di Bisceglie, C., Dell’Aquila, C., et al. (2014). Medical treatment of subjects with gender identity disorder: The experience in an Italian public health center. International Journal Of Transgenderism , 15 (2), 53-65.
Hormonal treatment is the main element during the transition program for transpeople. The aim of this paper is to describe the care and treatment of subjects, highlighting both the endocrine-metabolic effects of the hormonal therapy and the quality of life during the first year of cross-sex therapy in an Italian gender team. We studied 83 subjects (56 male-to-female [MtF], 27 female-to-male [FtM]) with hematological and hormonal evaluations every 3 months during the first year of hormonal therapy. MtF persons were treated with 17βestradiol and antiandrogens (cyproterone acetate, spironolactone, dutasteride); FtM persons were treated with transdermal or intramuscular testosterone. The WHO Quality of Life questionnaire was administered at the beginning and 1 year later. Hormonal changes paralleled phenotype modifications with wide variability. Most of both MtF and FtM subjects reported a statistically significant improvement in body image (p < 0.05). In particular, MtF subjects reported a statistically significant improvement in the quality of their sexual life and in the general quality of life (p < 0.05) 1 year after treatment initiation. Cross-sex therapy seems to be free of major risks in healthy subjects under clinical supervision during the first year. Selected subjects show an optimal adaptation to hormone-induced neuropsychological modifications and satisfaction regarding general and sexual life.
Megeri and Khoosal, 2007

Megeri, D., & Khoosal, D. (2007). Anxiety and depression in males experiencing gender dysphoria. Sexual & Relationship Therapy , 22 (1), 77-81.
Objective: The aim of the study was to compare anxiety and depression scores for the first 40 male to female people experiencing gender dysphoria attending the Leicester Gender Identity Clinic using the same sample as control pre and post gender realignment surgery. Hypothesis: There is an improvement in the scores of anxiety and depression following gender realignment surgery among people with gender dysphoria (male to female – transwomen). Results: There was no significant change in anxiety and depression scores in people with gender dysphoria (male to female) pre- and post-operatively.
Nelson, Whallett, & Mcgregor, 2009

Nelson, L., Whallett, E., & McGregor, J. (2009). Transgender patient satisfaction following reduction mammaplasty. Journal of Plastic, Reconstructive & Aesthetic Surgery , 62 (3), 331-334.
Aim: To evaluate the outcome of reduction mammaplasty in female-to-male transgender patients. Method: A 5-year retrospective review was conducted on all female-to-male transgender patients who underwent reduction mammaplasty. A postal questionnaire was devised to assess patient satisfaction, surgical outcome and psychological morbidity. Results: Seventeen patients were identified. The senior author performed bilateral reduction mammaplasties and free nipple grafts in 16 patients and one patient had a Benelli technique reduction. Complications included two haematomas, one wound infection, one wound dehiscence and three patients had hypertrophic scars. Secondary surgery was performed in seven patients and included scar revision, nipple reduction/realignment, dog-ear correction and nipple tattooing. The mean follow-up period after surgery was 10 months (range 2–23 months). Twelve postal questionnaires were completed (response rate 70%). All respondents expressed satisfaction with their result and no regret. Seven patients had nipple sensation and nine patients were satisfied with nipple position. All patients thought their scars were reasonable and felt that surgery had improved their self-confidence and social interactions. Conclusion: Reduction mammaplasty for female-to-male gender reassignment is associated with high patient satisfaction and a positive impact on the lives of these patients.
Newfield et al., 2006

Newfield, E., Hart, S., Dibble, S., & Kohler, L. (2006). Female-to-male transgender quality of life. Quality of Life Research , 15 (9), 1447-1457.
Objectives: We evaluated health-related quality of life in female-to-male (FTM) transgender individuals, using the Short-Form 36-Question Health Survey version 2 (SF-36v2). Methods: Using email, Internet bulletin boards, and postcards, we recruited individuals to an Internet site ( http://www.transurvey.org ), which contained a demographic survey and the SF36v2. We enrolled 446 FTM transgender and FTM transsexual participants, of which 384 were from the US. Results: Analysis of quality of life health concepts demonstrated statistically significant (p<0.0\) diminished quality of life among the FTM transgender participants as compared to the US male and female population, particularly in regard to mental health. FTM transgender participants who received testosterone (67%) reported statistically significant higher quality of life scores (/?<0.01) than those who had not received hormone therapy. Conclusions: FTM transgender participants reported significantly reduced mental health-related quality of life and
Padula, Heru, & Campbell, 2016

Padula, W. V., Heru, S. & Campbell, J. D. (2016). Societal implications of health insurance coverage for medically necessary services in the U.S. transgender population: A cost-effectiveness analysis. Journal of General Internal Medicine , 31 ( 4), 394-401.
Background: Recently, the Massachusetts Group Insurance Commission (GIC) prioritized research on the implications of a clause expressly prohibiting the denial of health insurance coverage for transgender-related services. These medically necessary services include primary and preventive care as well as transitional therapy. Objective: To analyze the cost-effectiveness of insurance coverage for medically necessary transgender-related services. Design: Markov model with 5- and 10-year time horizons from a U.S. societal perspective, discounted at 3 % (USD 2013). Data on outcomes were abstracted from the 2011 National Transgender Discrimination Survey (NTDS). Patients: U.S. transgender population starting before transitional therapy. Interventions: No health benefits compared to health insurance coverage for medically necessary services. This coverage can lead to hormone replacement therapy, sex reassignment surgery, or both. Main Measures: Cost per quality-adjusted life year (QALY) for successful transition or negative outcomes (e.g. HIV, depression, suicidality, drug abuse, mortality) dependent on insurance coverage or no health benefit at a willingness-to-pay threshold of $100,000/QALY. Budget impact interpreted as the U.S. per-member-per-month cost. Key Results: Compared to no health benefits for transgender patients ($23,619; 6.49 QALYs), insurance coverage for medically necessary services came at a greater cost and effectiveness ($31,816; 7.37 QALYs), with an incremental cost-effectiveness ratio (ICER) of $9314/QALY. The budget impact of this coverage is approximately $0.016 per member per month. Although the cost for transitions is $10,000–22,000 and the cost of provider coverage is $2175/year, these additional expenses hold good value for reducing the risk of negative endpoints —HIV, depression, suicidality, and drug abuse. Results were robust to uncertainty. The probabilistic sensitivity analysis showed that provider coverage was cost-effective in 85 % of simulations. Conclusions: Health insurance coverage for the U.S. transgender population is affordable and cost-effective, and has a low budget impact on U.S. society. Organizations such as the GIC should consider these results when examining policies regarding coverage exclusions.
Parola et al., 2010

Parola, N., Bonierbale, M., Lemaire, A., Aghababian, V., Michel, A., & Lançon, C. (2010). Study of quality of life for transsexuals after hormonal and surgical reassignment. Sexologies , 19 (1), 24-28.
Aim: The main objective of this work is to provide a more detailed assessment of the impact of surgical reassignment on the most important aspects of daily life for these patients. Our secondary objective was to establish the influence of various factors likely to have an impact on the quality of life (QoL), such as biological gender and the subject’s personality. Methods: A personality study was conducted using Eysenck Personality Inventory (EPI) so as to analyze two aspects of the personality (extraversion and neuroticism). Thirty-eight subjects who had undergone hormonal surgical reassignment were included in the study. Results: The results show that gender reassignment surgery improves the QoL for transsexuals in several different important areas: most are satisfied of their sexual reassignment (28/30), their social (21/30) and sexual QoL (25/30) are improved. However, there are differences between male-to-female (MtF) and female-to-male (FtM) transsexuals in terms of QoL: FtM have a better social, professional, friendly lifestyles than MtF. Finally, the results of this study did not evidence any influence by certain aspects of the personality, such as extraversion and neuroticism, on the QoL for reassigned subjects.
Pfäfflin, 1993

Pfäfflin, F. (1993). Regrets after sex reassignment surgery. Journal of Psychology & Human Sexuality , 5 (4), 69-85.
Using data draw from the follow-up literature covering the last 30 years, and the author’s clinical data on 295 men and women after SRS, an estimation of the number of patients who regretted the operations is made. Among female-to-male transsexuals after SRS, i.e., in men, no regrets were reported in the author’s sample, and in the literature they amount to less than 1%. Among male-to- female transsexuals after SRS, i.e., in women, regrets are reported in 1-1.5%. Poor differential diagnosis, failure to carry out the real-life- test, and poor surgical results seem to be the main reasons behind the regrets reported in the literature. According to three cases observed by the author in addition to personality traits the lack of proper care in treating the patients played a major role.
Pimenoff and Pfäfflin, 2011

Pimenoff, V., & Pfäfflin, F. (2011). Transsexualism: Treatment outcome of compliant and noncompliant patients. International Journal Of Transgenderism , 13 (1), 37-44.
The objective of the study was a follow-up of the treatment outcome of Finnish transsexuals who sought sex reassignment during the period 1970–2002 and a comparison of the results and duration of treatment of compliant and noncompliant patients. Fifteen male-to-female transsexuals and 17 female-to-male transsexuals who had undergone hormone and surgical treatment and legal sex reassignment in Finland completed a questionnaire on psychosocial data and on their experience with the different phases of clinical assessment and treatment. The changes in their vocational functioning and social and psychic adjustment were used as outcome indicators. The results and duration of the treatment of compliant and noncompliant patients were compared. The patients benefited significantly from treatment. The noncompliant patients achieved equally good results as the compliant ones, and did so in a shorter time. A good treatment outcome could be achieved even when the patient had told the assessing psychiatrist a falsified story of his life and sought hormone therapy, genital surgery, or legal sex reassignment on his own initiative without a recommendation from the psychiatrist. Based on these findings, it is recommended that the doctor-patient relationship be reconsidered and founded on frank cooperation.
Rakic et al., 1996

Rakic, Z., Starcevic, V., Maric, J., & Kelin, K. (1996). The outcome of sex reassignment surgery in Belgrade: 32 patients of both sexes. Archives of Sexual Behavior , 25 (5), 515-525.
Several aspects of the quality of life after sex reassignment surgery in 32 transsexuals of both sexes (22 men, 10 women) were examined. The Belgrade Team for Gender Identity Disorders designed a standardized questionnaire for this purpose. The follow-up period after operation was from 6 months to 4 years, and four aspects of the quality of life were examined: attitude towards the patients’ own body, relationships with other people, sexual activity, and occupational functioning. In most transsexuals, the quality of life was improved after surgery inasmuch as these four aspects are concerned. Only a few transsexuals were not satisfied with their life after surgery.
Rehman et al., 1999

Rehman, J., Lazer, S., Benet, A. E., Schaefer, L. C., & Melman, A. (1999). The reported sex and surgery satisfactions of 28 postoperative male-to-female transsexual patients. Archives of Sexual Behavior , 28 (1), 71-89.
From 1980 to July 1997 sixty-one male-to-female gender transformation surgeries were performed at our university center by one author (A.M.). Data were collected from patients who had surgery up to 1994 (n = 47) to obtain a minimum follow-up of 3 years; 28 patients were contacted. A mail questionnaire was supplemented by personal interviews with 11 patients and telephone interviews with remaining patients to obtain and clarify additional information. Physical and functional results of surgery were judged to be good, with few patients requiring additional corrective surgery. General satisfaction was expressed over the quality of cosmetic (normal appearing genitalia) and functional (ability to perceive orgasm) results. Follow-up showed satisfied who believed they had normal appearing genitalia and the ability to experience orgasm. Most patients were able to return to their jobs and live a more satisfactory social and personal life. One significant outcome was the importance of proper preparation of patients for surgery and especially the need for additional postoperative psychotherapy. None of the patients regretted having had surgery. However, some were, to a degree, disappointed because of difficulties experienced post operatively in adjusting satisfactorily as women both in their relationships with men and in living their lives generally as women. Findings of this study make a strong case for making a change in the Harry Benjamin Standards of Care to include a period of postoperative psychotherapy.
Rotondi et al., 2011

Rotondi, N. K., Bauer, G. R., Scanlon, K., Kaay, M., Travers, R., & Travers, A. (2011). Prevalence of and risk and protective factors for depression in female-to-male transgender Ontarians: Trans PULSE Project. Canadian Journal Of Community Mental Health , 30 (2), 135-155.
Although depression is understudied in transgender and transsexual communities, high prevalences have been reported. This paper presents original research from the Trans PULSE Project, an Ontario-wide, community-based initiative that surveyed 433 participants using respondent-driven sampling. The purpose of this analysis was to determine the prevalence of, and risk and protective factors for, depression among female-to-male (FTM) Ontarians (n = 207). We estimate that 66.4% of FTMs have symptomatology consistent with depression. In multivariable analyses, sexual satisfaction was a strong protective factor. Conversely, experiencing transphobia and being at the stage of planning but not having begun a medical transition (hormones and/or surgery) adversely affected mental health in FTMs.
Ruppin and Pfäfflin, 2015

Ruppin, U., & Pfäfflin, F. (2015). Long-term follow-up of adults with gender identity disorder. Archives of Sexual Behavior , 44 (5), 1321-1329.
The aim of this study was to re-examine individuals with gender identity disorder after as long a period of time as possible. To meet the inclusion criterion, the legal recognition of participants’ gender change via a legal name change had to date back at least 10 years. The sample comprised 71 participants (35 MtF and 36 FtM). The follow-up period was 10–24 years with a mean of 13.8 years (SD = 2.78). Instruments included a combination of qualitative and quantitative methods: Clinical interviews were conducted with the participants, and they completed a follow-up questionnaire as well as several standardized questionnaires they had already filled in when they first made contact with the clinic. Positive and desired changes were determined by all of the instruments: Participants reported high degrees of well-being and a good social integration. Very few participants were unemployed, most of them had a steady relationship, and they were also satisfied with their relationships with family and friends. Their overall evaluation of the treatment process for sex reassignment and its effectiveness in reducing gender dysphoria was positive. Regarding the results of the standardized questionnaires, participants showed significantly fewer psychological problems and interpersonal difficulties as well as a strongly increased life satisfaction at follow-up than at the time of the initial consultation. Despite these positive results, the treatment of transsexualism is far from being perfect.
Smith et al., 2005

Smith, Y. L. S., Van Goozen, S. H. M., Kuiper, A. J., & Cohen-Kettenis, P. (2005). Sex reassignment: Outcomes and predictors of treatment for adolescent and adult transsexuals. Psychological Medicine, 35 (1), 89-99.
Background: We prospectively studied outcomes of sex reassignment, potential differences between subgroups of transsexuals, and predictors of treatment course and outcome. Method: Altogether 325 consecutive adolescent and adult applicants for sex reassignment participated: 222 started hormone treatment, 103 did not; 188 completed and 34 dropped out of treatment. Only data of the 162 adults were used to evaluate treatment. Results between subgroups were compared to determine post-operative differences. Adults and adolescents were included to study predictors of treatment course and outcome. Results were statistically analysed with logistic regression and multiple linear regression analyses. Results: After treatment the group was no longer gender dysphoric. The vast majority functioned quite well psychologically, socially and sexually. Two non-homosexual male-to-female transsexuals expressed regrets. Post-operatively, female-to-male and homosexual transsexuals functioned better in many respects than male-to-female and non-homosexual transsexuals. Eligibility for treatment was largely based upon gender dysphoria, psychological stability, and physical appearance. Male-to-female transsexuals with more psychopathology and cross-gender symptoms in childhood, yet less gender dysphoria at application, were more likely to drop out prematurely. Non-homosexual applicants with much psychopathology and body dissatisfaction reported the worst post-operative outcomes. Conclusions: The results substantiate previous conclusions that sex reassignment is effective. Still, clinicians need to be alert for non-homosexual male-to-females with unfavourable psychological functioning and physical appearance and inconsistent gender dysphoria reports, as these are risk factors for dropping out and poor post-operative results. If they are considered eligible, they may require additional therapeutic guidance during or even after treatment.
van de Grift et al., 2017

van de Grift, T. C., Elaut, E., Cerwenka, S. C., Cohen-Kettenis, P. T., Cuypere, G. D., Richter-Appelt, H., & Kreukels, B. P. (2017). Effects of medical interventions on gender dysphoria and body image. Psychosomatic Medicine , 79 (7), 815-823.
Objective: The aim of this study from the European Network for the Investigation of Gender Incongruence is to investigate the status of all individuals who had applied for gender confirming interventions from 2007 to 2009, irrespective of whether they received treatment. The current article describes the study protocol, the effect of medical treatment on gender dysphoria and body image, and the predictive value of (pre)treatment factors on posttreatment outcomes. Methods: Data were collected on medical interventions, transition status, gender dysphoria (Utrecht Gender Dysphoria Scale), and body image (Body Image Scale for transsexuals). In total, 201 people participated in the study (37% of the original cohort). Results: At follow-up, 29 participants (14%) did not receive medical interventions, 36 hormones only (18%), and 136 hormones and surgery (68%). Most transwomen had undergone genital surgery, and most transmen chest surgery. Overall, the levels of gender dysphoria and body dissatisfaction were significantly lower at follow-up compared with clinical entry. Satisfaction with therapy responsive and unresponsive body characteristics both improved. High dissatisfaction at admission and lower psychological functioning at follow-up were associated with persistent body dissatisfaction. Conclusions: Hormone-based interventions and surgery were followed by improvements in body satisfaction. The level of psychological symptoms and the degree of body satisfaction at baseline were significantly associated with body satisfaction at follow-up.

van de Grift, T. C., Elaut, E., Cerwenka, S. C., Cohen-Kettenis, P. T., & Kreukels, B. P. (2017). Surgical satisfaction, quality of life, and their association after gender-affirming surgery: A follow-up study. Journal of Sex & Marital Therapy , 44 (2), 138-148.
We assessed the outcomes of gender-affirming surgery (GAS, or sex-reassignment surgery) 4 to 6 years after first clinical contact, and the associations between postoperative (dis)satisfaction and quality of life (QoL). Our multicenter, cross-sectional follow-up study involved persons diagnosed with gender dysphoria (DSM-IV-TR) who applied for medical interventions from 2007 until 2009. Of 546 eligible persons, 201 (37%) responded, of whom 136 had undergone GAS (genital, chest, facial, vocal cord and/or thyroid cartilage surgery). Main outcome measures were procedure performed, self-reported complications, and satisfaction with surgical outcomes (standardized questionnaires), QoL (Satisfaction With Life Scale, Subjective Happiness Scale, Cantril Ladder), gender dysphoria (Utrecht Gender Dysphoria Scale), and psychological symptoms (Symptom Checklist-90). Postoperative satisfaction was 94% to 100%, depending on the type of surgery performed. Eight (6%) of the participants reported dissatisfaction and/or regret, which was associated with preoperative psychological symptoms or self-reported surgical complications (OR= 6.07). Satisfied respondents’ QoL scores were similar to reference values; dissatisfied or regretful respondents’ scores were lower. Therefore, dissatisfaction after GAS may be viewed as indicator of unfavorable psychological and QoL outcomes.
Vujovic et al., 2009

Vujovic, S., Popovic, S., Sbutega-Milosevic, G., Djordjevic, M., & Gooren, L. (2009). Transsexualism in Serbia: A twenty-year follow-up study. The Journal of Sexual Medicine , 6 (4), 1018-1023.
Introduction: Gender dysphoria occurs in all societies and cultures. The prevailing social context has a strong impact on its manifestations as well as on applications by individuals with the condition for sex reassignment treatment. Aim: To describe a transsexual population seeking sex reassignment treatment in Serbia, part of former Yugoslavia. Methods: Data, collated over a period of 20 years, from subjects applying for sex reassignment to the only center in Serbia, were analyzed retrospectively. Main Outcome Measures: Age at the time of application, demographic data, family background, sex ratio, the prevalence of polycystic ovarian syndrome (PCOS) among female-to-male (FTM) transsexuals, and readiness to undergo surgical sex reassignment were tabulated. Results: Applicants for sex reassignment in Serbia are relatively young. The sex ratio is close to 1:1. They often come from single-child families. More than 10% do not wish to undergo surgical sex reassignment. The prevalence of PCOS among FTM transsexuals was higher than in the general population but considerably lower than that reported in the literature from other populations. Of those who had undergone sex reassignment, none expressed regret for their decision. Conclusions: Although transsexualism is a universal phenomenon, the relatively young age of those applying for sex reassignment and the sex ratio of 1:1 distinguish the population in Serbia from others reported in the literature.
Weigert et al., 2013

Weigert, R., Frison, E., Sessiecq, Q., Al Mutairi, K., & Casoli, V. (2013). Patient satisfaction with breasts and psychosocial, sexual, and physical well-being after breast augmentation in male-to-female transsexuals. Plastic and Reconstructive Surgery, 132 (6), 1421-1429.
Background: Satisfaction with breasts, sexual well-being, psychosocial well-being, and physical well-being are essential outcome factors following breast augmentation surgery in male-to-female transsexual patients. The aim of this study was to measure change in patient satisfaction with breasts and sexual, physical, and psychosocial well-being after breast augmentation in male-to-female transsexual patients. Methods: All consecutive male-to-female transsexual patients who underwent breast augmentation between 2008 and 2012 were asked to complete the BREAST-Q Augmentation module questionnaire before surgery, at 4 months, and later after surgery. A prospective cohort study was designed and postoperative scores were compared with baseline scores. Satisfaction with breasts and sexual, physical, and psychosocial outcomes assessment was based on the BREAST-Q. Results: Thirty-five male-to-female transsexual patients completed the questionnaires. BREAST-Q subscale median scores (satisfaction with breasts, +59 points; sexual well-being, +34 points; and psychosocial well-being, +48 points) improved significantly (p < 0.05) at 4 months postoperatively and later. No significant change was observed in physical well-being. Conclusions: In this prospective, noncomparative, cohort study, the current results suggest that the gains in breast satisfaction, psychosocial well-being, and sexual well-being after male-to-female transsexual patients undergo breast augmentation are statistically significant and clinically meaningful to the patient at 4 months after surgery and in the long term.
Weyers et al., 2009

Weyers, S., Elaut, E., De Sutter, P., Gerris, J., T’Sjoen, G., et al. (2009). Long-term assessment of the physical, mental, and sexual health among transsexual women. The Journal of Sexual Medicine , 6 (3), 752-760.
Introduction: Transsexualism is the most extreme form of gender identity disorder and most transsexuals eventually pursue sex reassignment surgery (SRS). In transsexual women, this comprises removal of the male reproductive organs, creation of a neovagina and clitoris, and often implantation of breast prostheses. Studies have shown good sexual satisfaction after transition. However, long-term follow-up data on physical, mental and sexual functioning are lacking. Aim: To gather information on physical, mental, and sexual well-being, health-promoting behavior and satisfaction with gender-related body features of transsexual women who had undergone SRS. Methods: Fifty transsexual women who had undergone SRS >or=6 months earlier were recruited. Main Outcome Measures: Self-reported physical and mental health using the Dutch version of the Short-Form-36 (SF-36) Health Survey; sexual functioning using the Dutch version of the Female Sexual Function Index (FSFI). Satisfaction with gender-related bodily features as well as with perceived female appearance; importance of sex, relationship quality, necessity and advisability of gynecological exams, as well as health concerns and feelings of regret concerning transition were scored. Results: Compared with reference populations, transsexual women scored good on physical and mental level (SF-36). Gender-related bodily features were shown to be of high value. Appreciation of their appearance as perceived by others, as well as their own satisfaction with their self-image as women obtained a good score (8 and 9, respectively). However, sexual functioning as assessed through FSFI was suboptimal when compared with biological women, especially the sublevels concerning arousal, lubrication, and pain. Superior scores concerning sexual function were obtained in those transsexual women who were in a relationship and in heterosexuals. Conclusions: Transsexual women function well on a physical, emotional, psychological and social level. With respect to sexuality, they suffer from specific difficulties, especially concerning arousal, lubrication, and pain.
Back to Top
Below are 4 studies that contain mixed or null findings on the effect of gender transition on transgender well-being. Click here to jump to the 17 studies that consist of literature reviews or guidelines that help advance knowledge about the effect of gender transition on transgender well-being . Click here to jump to the 51 studies that found that gender transition improves the well-being of transgender people .
Barrett, 1998.

Barrett J. (1998). Psychological and social function before and after phalloplasty. The International Journal of Transgenderism , 2 (1), 1-8.
There are no quantitative assessments of the benefits of phalloplasty in a female transsexual population. The study addresses this question, comparing transsexuals accepted for such surgery with transsexuals after such surgery has been performed. A population of 23 transsexuals accepted for phalloplasty was compared to a population of 40 who had undergone such surgery between six and one hundred and sixty months previously. The General Health Questionnaire (GHQ), Symptom Checklist 90 (SCL-90), Bem Sex Role Inventory and Social Role Performance Schedule (SRPS) were employed. Additionally, a questionnaire assessing satisfaction with cosmetic appearance, sexual function, relationship and urinary function was used, along with a semi-structured interview quantifying alcohol, cigarette and drug usage, and current sexual practice. There were significant differences between the populations. The post operative group showed higher depression ratings on the depression subscale of the GHQ. The masculine pre-operative Bem scores were neutral post-operatively as feminine sub-scores increased. There was improved satisfaction with genital appearance post-operatively, but satisfaction with relationships fell, although to a non-significant extent. Most other changes were in the expected direction but did not achieve significance. Transsexuals accepted for phalloplasty have very good psychological health. Tendency to further improvement is the case after phalloplasty. Depression is commoner, however, and quality of relationships declines somewhat, perhaps in consequence. Surgeons might advise partners as well as patients of realistic expectations from such surgery.
Lindqvist et al., 2017

Lindqvist, E. K., Sigurjonsson, H., Möllermark, C., Rinder, J., Farnebo, F., et al. (2017). Quality of life improves early after gender reassignment surgery in transgender women. European Journal of Plastic Surgery , 40 (3), 223-226.
Background: Few studies have examined the long-term quality of life (QoL) of individuals with gender dysphoria, or how it is affected by treatment. Our aim was to examine the QoL of transgender women undergoing gender reassignment surgery (GRS). Methods: We performed a prospective cohort study on 190 patients undergoing male-to-female GRS at Karolinska University Hospital between 2003 and 2015. We used the Swedish version of the Short Form-36 Health Survey (SF-36), which measures QoL across eight domains. The questionnaire was distributed to patients pre-operatively, as well as 1, 3, and 5 years post-operatively. The results were compared between the different measure points, as well as between the study group and the general population. Results: On most dimensions of the SF-36 questionnaire, transgender women reported a lower QoL than the general population. The scores of SF-36 showed a non-significant trend to be lower 5 years post-GRS compared to pre-operatively, a decline consistent with that of the general population. Self-perceived health compared to 1 year previously rose in the first post-operative year, after which it declined. Conclusions: To our knowledge, this is the largest prospective study to follow a group of transgender patients with regards to QoL over continuous temporal measure points. Our results show that transgender women generally have a lower QoL compared to the general population. GRS leads to an improvement in general well-being as a trend but over the long-term, QoL decreases slightly in line with that of the comparison group. Level of evidence: Level III, therapeutic study.
Simonsen et al., 2016

Simonsen, R. K., Giraldi, A., Kristensen, E., & Hald, G. M. (2016). Long-term follow-up of individuals undergoing sex reassignment surgery: Psychiatric morbidity and mortality. Nordic Journal Of Psychiatry , 70 (4), 241-247.
Background: There is a lack of long-term register-based follow-up studies of sex-reassigned individuals concerning mortality and psychiatric morbidity. Accordingly, the present study investigated both mortality and psychiatric morbidity using a sample of individuals with transsexualism which comprised 98% (n = 104) of all individuals in Denmark. Aims: (1) To investigate psychiatric morbidity before and after sex reassignment surgery (SRS) among Danish individuals who underwent SRS during the period of 1978–2010. (2) To investigate mortality among Danish individuals who underwent SRS during the period of 1978–2010.Method: Psychiatric morbidity and mortality were identified by data from the Danish Psychiatric Central Research Register and the Cause of Death Register through a retrospective register study of 104 sex-reassigned individuals. Results: Overall, 27.9% of the sample were registered with psychiatric morbidity before SRS and 22.1% after SRS (p = not significant). A total of 6.7% of the sample were registered with psychiatric morbidity both before and after SRS. Significantly more psychiatric diagnoses were found before SRS for those assigned as female at birth. Ten individuals were registered as deceased post-SRS with an average age of death of 53.5 years. Conclusions: No significant difference in psychiatric morbidity or mortality was found between male to female and female to male (FtM) save for the total number of psychiatric diagnoses where FtM held a significantly higher number of psychiatric diagnoses overall. Despite the over-representation of psychiatric diagnoses both pre- and post-SRS the study found that only a relatively limited number of individuals had received diagnoses both prior to and after SRS. This suggests that generally SRS may reduce psychological morbidity for some individuals while increasing it for others.
Udeze, 2008

Udeze, B., Abdelmawla, N., Khoosal, D., & Terry, T. (2008). Psychological functions in male-to-female transsexual people before and after surgery. Sexual & Relationship Therapy , 23 (2), 141-145.
Patients with gender dysphoria (GD) suffer from a constant feeling of psychological discomfort related to their anatomical sex. Gender reassignment surgery (GRS) attempts to release this discomfort. The aim of this study was to compare the functioning of a cohort or patients with GD before and after GRS. We hypothesized that there would be an improvement in the scores of the self-administered SCL-90R following gender reassignment surgery among male-to-female people with gender dysphoria. We studied 40 patients with a DSM-IV diagnosis of Gender Identity Disorder (GID) who attended Leicester Gender Identity Clinic. We compared their functioning as measured by Symptom Check List-90R (SCL-90R) which was administered to 40 randomly selected male-to-female patients before and within six months after GRS using the same sample as control pre-and post-surgery. There was no significant change in the different sub-scales of the SCL-90R scores in patients with male-to-female GID pre- and within six months post-surgery. The results of the study showed that GRS had no significant effect on functioning as measured by SCL-90R within six months of surgery. Our study has the advantage of reducing inter-subject variability by using the same patients as their own control. This study may be limited by the duration of reassessment post-surgery. Further studies with larger sample size and using other psychosocial scales are needed to elucidate on the effectiveness of surgical intervention on psychosocial parameters in patients with GD.
Below are 17 studies that consist of literature reviews or guidelines that help advance knowledge about the effect of gender transition on transgender well-being. Click here to jump to the 4 studies that contain mixed or null findings on the effect of gender transition on transgender well-being. Click here Click here to jump to the 51 studies that found that gender transition improves the well-being of transgender people .
American psychological, 2015.

Guidelines for psychological practice with transgender and gender nonconforming people. (2015). American Psychologist, 70 (9), 832-864.
In 2015, the American Psychological Association adopted Guidelines for Psychological Practice with Transgender and Gender Nonconforming Clients in order to describe affirmative psychological practice with transgender and gender nonconforming (TGNC) clients. There are 16 guidelines in this document that guide TGNC-affirmative psychological practice across the lifespan, from TGNC children to older adults. The Guidelines are organized into five clusters: (a) foundational knowledge and awareness; (b) stigma, discrimination, and barriers to care; (c) lifespan development; (d) assessment, therapy, and intervention; and (e) research, education, and training. In addition, the guidelines provide attention to TGNC people across a range of gender and racial/ethnic identities. The psychological practice guidelines also attend to issues of research and how psychologists may address the many social inequities TGNC people experience.
Bockting et al., 2016

Bockting, W., Coleman, E., Deutsch, M. B., Guillamon, A., Meyer, W., et al. (2016). Adult development and quality of life of transgender and gender nonconforming people. Current Opinion in Endocrinology & Diabetes and Obesity , 23 (2), 188–197.
Purpose of review: Research on the health of transgender and gender nonconforming people has been limited with most of the work focusing on transition-related care and HIV. The present review summarizes research to date on the overall development and quality of life of transgender and gender nonconforming adults, and makes recommendations for future research. Recent findings: Pervasive stigma and discrimination attached to gender nonconformity affect the health of transgender people across the lifespan, particularly when it comes to mental health and well-being. Despite the related challenges, transgender and gender nonconforming people may develop resilience over time. Social support and affirmation of gender identity play herein a critical role. Although there is a growing awareness of diversity in gender identity and expression among this population, a comprehensive understanding of biopsychosocial development beyond the gender binary and beyond transition is lacking. Summary: Greater visibility of transgender people in society has revealed the need to understand and promote their health and quality of life broadly, including but not limited to gender dysphoria and HIV. This means addressing their needs in context of their families and communities, sexual and reproductive health, and successful aging. Research is needed to better understand what factors are associated with resilience and how it can be effectively promoted.
Byne et al., 2012

Byne, W., Bradley, S.J., Coleman, E., et al. (2012). Report of the American Psychiatric Association task force on treatment of gender identity disorder. Archives of Sexual Behavior, 41 (4): 759–796.
Both the diagnosis and treatment of Gender Identity Disorder (GID) are controversial. Although linked, they are separate issues and the DSM does not evaluate treatments. The Board of Trustees (BOT) of the American Psychiatric Association (APA), therefore, formed a Task Force charged to perform a critical review of the literature on the treatment of GID at different ages, to assess the quality of evidence pertaining to treatment, and to prepare a report that included an opinion as to whether or not sufficient credible literature exists for development of treatment recommendations by the APA. The literature on treatment of gender dysphoria in individuals with disorders of sex development was also assessed. The completed report was accepted by the BOT on September 11, 2011. The quality of evidence pertaining to most aspects of treatment in all subgroups was determined to be low; however, areas of broad clinical consensus were identified and were deemed sufficient to support recommendations for treatment in all subgroups. With subjective improvement as the primary outcome measure, current evidence was judged sufficient to support recommendations for adults in the form of an evidence-based APA Practice Guideline with gaps in the empirical data supplemented by clinical consensus. The report recommends that the APA take steps beyond drafting treatment recommendations. These include issuing position statements to clarify the APA’s position regarding the medical necessity of treatments for GID, the ethical bounds of treatments of gender variant minors, and the rights of persons of any age who are gender variant, transgender or transsexual.
Carroll, 1999

Carroll, R. A. (1999). Outcomes of treatment for gender dysphoria. Journal of Sex Education and Therapy , 24 (3), 128–136.
This paper reviews the empirical research on the psychosocial outcomes of treatment for gender dysphoria. Recent research has highlighted the heterogeneity of transgendered experiences. There are four possible outcomes for patients who present with the dilemma of gender dysphoria: an unresolved outcome, acceptance of one’s given gender, engaging in a cross-gender role on a part-time basis, and making a full-time transition to the other gender role. Clinical work, but not empirical research, suggests that some individuals with gender dysphoria may come to accept their given gender role through psychological treatment. Many individuals find that it is psychologically sufficient to express the transgendered part of themselves through such activities as cross-dressing or gender blending. The large body of research on the outcome of gender reassignment surgery indicates that, for the majority of those who undergo this process, the outcome is positive. Predictors of a good outcome include good pre-reassignment psychological adjustment, family support, at least 1 year of living in the desired role, consistent use of hormones, psychological treatment, and good surgical outcomes. The outcome literature provides strong support for adherence to the Standards of Care of the Harry Benjamin International Gender Dysphoria Association. Implications to be drawn from this research include an appreciation of the diversity of transgendered experience, the need for more research on non-reassignment resolutions to gender dysphoria, and the importance of assisting the transgendered individual to identify the resolution that best suits him or her.
Cohen-Kettenis and Gooren, 1999

Cohen-Kettenis, P. T., & Gooren, L. J. G. (1999). Transsexualism: A review of etiology, diagnosis and treatment. Journal of Psychosomatic Research , 46 (4), 315-333.
Transsexualism is considered to be the extreme end of the spectrum of gender identity disorders characterized by, among other things, a pursuit of sex reassignment surgery (SRS). The origins of transsexualism are still largely unclear. A first indication of anatomic brain differences between transsexuals and nontranssexuals has been found. Also, certain parental (rearing) factors seem to be associated with transsexualism. Some contradictory findings regarding etiology, psychopathology and success of SRS seem to be related to the fact that certain subtypes of transsexuals follow different developmental routes. The observations that psychotherapy is not helpful in altering a crystallized cross-gender identity and that certain transsexuals do not show severe psychopathology has led clinicians to adopt sex reassignment as a treatment option. In many countries, transsexuals are now treated according to the Standards of Care of the Harry Benjamin International Gender Dysphoria Association, a professional organization in the field of transsexualism. Research on postoperative functioning of transsexuals does not allow for unequivocal conclusions, but there is little doubt that sex reassignment substantially alleviates the suffering of transsexuals. However, SRS is no panacea. Psychotherapy may be needed to help transsexuals in adapting to the new situation or in dealing with issues that could not be addressed before treatment.
Coleman et al., 2012

Coleman, E., Bockting, W., Botzer, M., Cohen-Kettenis, P., DeCuypere, G., et al. (2012). Standards of care for the health of transsexual, transgender, and gender-nonconforming people, version 7. International Journal of Transgenderism , 13 (4), 165-232.
The Standards of Care (SOC) for the Health of Transsexual, Transgender, and Gender Nonconforming People is a publication of the World Professional Association for Transgender Health (WPATH). The overall goal of the SOC is to provide clinical guidance for health professionals to assist transsexual, transgender, and gender nonconforming people with safe and effective pathways to achieving lasting personal comfort with their gendered selves, in order to maximize their overall health, psychological well-being, and self-fulfillment. This assistance may include primary care, gynecologic and urologic care, reproductive options, voice and communication therapy, mental health services (e.g., assessment, counseling, psychotherapy), and hormonal and surgical treatments. The SOC are based on the best available science and expert professional consensus. Because most of the research and experience in this field comes from a North American and Western European perspective, adaptations of the SOC to other parts of the world are necessary. The SOC articulate standards of care while acknowledging the role of making informed choices and the value of harm reduction approaches. In addition, this version of the SOC recognizes that treatment for gender dysphoria i.e., discomfort or distress that is caused by a discrepancy between persons gender identity and that persons sex assigned at birth (and the associated gender role and/or primary and secondary sex characteristics) has become more individualized. Some individuals who present for care will have made significant self-directed progress towards gender role changes or other resolutions regarding their gender identity or gender dysphoria. Other individuals will require more intensive services. Health professionals can use the SOC to help patients consider the full range of health services open to them, in accordance with their clinical needs and goals for gender expression.
Committee on Health Care for Underserved, 2011

Committee Opinion No. 512: Health Care for Transgender Individuals. (2011). Obstetrics & Gynecology , 118 (6), 1454–1458.
Transgender individuals face harassment, discrimination, and rejection within our society. Lack of awareness, knowledge, and sensitivity in health care communities eventually leads to inadequate access to, underutilization of, and disparities within the health care system for this population. Although the care for these patients is often managed by a specialty team, obstetrician–gynecologists should be prepared to assist or refer transgender individuals with routine treatment and screening as well as hormonal and surgical therapies. The American College of Obstetricians and Gynecologists opposes discrimination on the basis of gender identity and urges public and private health insurance plans to cover the treatment of gender identity disorder.
Costa and Colizzi, 2016

Costa, R., & Colizzi, M. (2016). The effect of cross-sex hormonal treatment on gender dysphoria individuals’ mental health: A systematic review. Neuropsychiatric Disease and Treatment , 12 , 1953-1966.
Cross-sex hormonal treatment represents a main aspect of gender dysphoria health care pathway. However, it is still debated whether this intervention translates into a better mental well-being for the individual and which mechanisms may underlie this association. Although sex reassignment surgery has been the subject of extensive investigation, few studies have specifically focused on hormonal treatment in recent years. Here, we systematically review all studies examining the effect of cross-sex hormonal treatment on mental health and well-being in gender dysphoria. Research tends to support the evidence that hormone therapy reduces symptoms of anxiety and dissociation, lowering perceived and social distress and improving quality of life and self-esteem in both male-to-female and female-to-male individuals. Instead, compared to female-to-male individuals, hormone-treated male-to-female individuals seem to benefit more in terms of a reduction in their body uneasiness and personality-related psychopathology and an amelioration of their emotional functioning. Less consistent findings support an association between hormonal treatment and other mental health-related dimensions. In particular, depression, global psychopathology, and psychosocial functioning difficulties appear to reduce only in some studies, while others do not suggest any improvement in these domains. Results from longitudinal studies support more consistently the association between hormonal treatment and improved mental health. On the contrary, a number of cross-sectional studies do not support this evidence. This review provides possible biological explanation vs psychological explanation (direct effect vs indirect effect) for the hormonal treatment-induced better mental well-being. In conclusion, this review indicates that gender dysphoria-related mental distress may benefit from hormonal treatment intervention, suggesting a transient reaction to the nonsatisfaction connected to the incongruent body image rather than a stable psychiatric comorbidity. In this perspective, timely hormonal treatment intervention represents a crucial issue in gender dysphoria individuals’ mental health-related outcome.
Dhejne et al., 2016

Dhejne, C., Van Vlerken, R., Heylens, G., & Arcelus, J. (2016). Mental health and gender dysphoria: A review of the literature. International Review Of Psychiatry , 28 (1), 44-57.
Studies investigating the prevalence of psychiatric disorders among trans individuals have identified elevated rates of psychopathology. Research has also provided conflicting psychiatric outcomes following gender-confirming medical interventions. This review identifies 38 cross-sectional and longitudinal studies describing prevalence rates of psychiatric disorders and psychiatric outcomes, pre- and post-gender-confirming medical interventions, for people with gender dysphoria. It indicates that, although the levels of psychopathology and psychiatric disorders in trans people attending services at the time of assessment are higher than in the cis population, they do improve following gender-confirming medical intervention, in many cases reaching normative values. The main Axis I psychiatric disorders were found to be depression and anxiety disorder. Other major psychiatric disorders, such as schizophrenia and bipolar disorder, were rare and were no more prevalent than in the general population. There was conflicting evidence regarding gender differences: some studies found higher psychopathology in trans women, while others found no differences between gender groups. Although many studies were methodologically weak, and included people at different stages of transition within the same cohort of patients, overall this review indicates that trans people attending transgender health-care services appear to have a higher risk of psychiatric morbidity (that improves following treatment), and thus confirms the vulnerability of this population.
Gijs and Brewaeys, 2007

Gijs, L., & Brewaeys, A. (2007). Surgical treatment of gender dysphoria in adults and adolescents: Recent developments, effectiveness, and challenges. Annual Review of Sex Research , 18 (1), 178-224.
In 1990 Green and Fleming concluded that sex reassignment surgery (SRS) is an effective treatment for transsexuality because it reduced gender dysphoria drastically. Since 1990, many new outcome studies have been published, raising the question as to whether the conclusion of Green and Fleming still holds. After describing terminological and conceptual developments related to the treatment of gender identity disorder (GID), follow-up studies, including both adults and adolescents, of the outcomes of SRS are reviewed. Special attention is paid to the effects of SRS on gender dysphoria, sexuality, and regret. Despite methodological shortcomings of many of the studies, we conclude that SRS is an effective treatment for transsexualism and the only treatment that has been evaluated empirically with large clinical case series.
Gooren, 2011

Gooren, L. J. (2011). Care of transsexual persons. New England Journal of Medicine , 364 (13), 1251–1257.
This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines, when they exist. The article ends with the author’s clinical recommendations. A healthy and successful 40-year-old man finds it increasingly difficult to live as a male. In childhood he preferred playing with girls and recalls feeling that he should have been one. Over time he has come to regard himself more and more as a female personality inhabiting a male body. After much agonizing, he has concluded that only sex reassignment can offer the peace of mind he craves. What would you advise? A healthy and successful 40-year-old man finds it increasingly difficult to live as a male. In childhood he preferred playing with girls and recalls feeling that he should have been one. Over time he has come to regard himself more and more as a female personality inhabiting a male body. After much agonizing, he has concluded that only sex reassignment can offer the peace of mind he craves. What would you advise?
Hembree et al., 2009

Hembree, W. C., Cohen-Kettenis, P., Delemarre-van de Waal, H. A., Gooren, L. J., Meyer, W., et al. (2009). Endocrine treatment of transsexual persons: An endocrine society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism, 94 (9), 3132–3154.
Objective: The aim was to formulate practice guidelines for endocrine treatment of transsexual persons. Evidence: This evidence-based guideline was developed using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system to describe the strength of recommendations and the quality of evidence, which was low or very low. Consensus Process: Committees and members of The Endocrine Society, European Society of Endocrinology, European Society for Paediatric Endocrinology, Lawson Wilkins Pediatric Endocrine Society, and World Professional Association for Transgender Health commented on preliminary drafts of these guidelines. Conclusions: Transsexual persons seeking to develop the physical characteristics of the desired gender require a safe, effective hormone regimen that will 1) suppress endogenous hormone secretion determined by the person’s genetic/biologic sex and 2) maintain sex hormone levels within the normal range for the person’s desired gender. A mental health professional (MHP) must recommend endocrine treatment and participate in ongoing care throughout the endocrine transition and decision for surgical sex reassignment. The endocrinologist must confirm the diagnostic criteria the MHP used to make these recommendations. Because a diagnosis of transsexualism in a prepubertal child cannot be made with certainty, we do not recommend endocrine treatment of prepubertal children. We recommend treating transsexual adolescents (Tanner stage 2) by suppressing puberty with GnRH analogues until age 16 years old, after which cross-sex hormones may be given. We suggest suppressing endogenous sex hormones, maintaining physiologic levels of gender-appropriate sex hormones and monitoring for known risks in adult transsexual persons. Endocrine treatment of transsexual persons should include suppression of endogenous sex hormones, physiologic levels of gender-appropriate sex hormones, and suppression of puberty in adolescents (Tanner stage 2).
Michel et al., 2002

Michel, A., Ansseau, M., Legros, J., Pitchot, W., & Mormont, C. (2002). The transsexual: What about the future? European Psychiatry , 17 (6), 353-362.
Since the 1950s, sexual surgical reassignments have been frequently carried out. As this surgical therapeutic procedure is controversial, it seems important to explore the actual consequences of such an intervention and objectively evaluate its relevance. In this context, we have carried out a review of the literature. After looking at the methodological limitations of follow-up studies, the psychological, sexual, social, and professional futures of the individuals subject to a transsexual operation are presented. Finally, prognostic aspects are considered. In the literature, follow-up studies tend to show that surgical transformations have positive consequences for the subjects. In the majority of cases, transsexuals are very satisfied with their intervention and any difficulties experienced are often temporary and disappear within a year after the surgical transformation. Studies show that there is less than 1% of regrets, and a little more than 1% of suicides among operated subjects. The empirical research does not confirm the opinion that suicide is strongly associated with surgical transformation.
Murad et al., 2010

Murad, M. H., Elamin, M. B., Garcia, M. Z., Mullan, R. J., Murad, A., Erwin, P. J., & Montori, V. M. (2010). Hormonal therapy and sex reassignment: A systematic review and meta-analysis of quality of life and psychosocial outcomes. Clinical Endocrinology , 72 (2), 214-231.
Objective: To assess the prognosis of individuals with gender identity disorder (GID) receiving hormonal therapy as a part of sex reassignment in terms of quality of life and other self‐reported psychosocial outcomes. Methods: We searched electronic databases, bibliography of included studies and expert files. All study designs were included with no language restrictions. Reviewers working independently and in pairs selected studies using predetermined inclusion and exclusion criteria, extracted outcome and quality data. We used a random‐effects meta‐analysis to pool proportions and estimate the 95% confidence intervals (CIs). We estimated the proportion of between‐study heterogeneity not attributable to chance using the I2 statistic. Results: We identified 28 eligible studies. These studies enrolled 1833 participants with GID (1093 male‐to‐female, 801 female‐to‐male) who underwent sex reassignment that included hormonal therapies. All the studies were observational and most lacked controls. Pooling across studies shows that after sex reassignment, 80% of individuals with GID reported significant improvement in gender dysphoria (95% CI = 68–89%; 8 studies; I2 = 82%); 78% reported significant improvement in psychological symptoms (95% CI = 56–94%; 7 studies; I2 = 86%); 80% reported significant improvement in quality of life (95% CI = 72–88%; 16 studies; I2 = 78%); and 72% reported significant improvement in sexual function (95% CI = 60–81%; 15 studies; I2 = 78%). Conclusions: Very low quality evidence suggests that sex reassignment that includes hormonal interventions in individuals with GID likely improves gender dysphoria, psychological functioning and comorbidities, sexual function and overall quality of life.
Reisner et al., 2016

Reisner, S. L., Poteat, T., Keatley, J., Cabral, M., Mothopeng, T., et al. (2016). Global health burden and needs of transgender populations: A review. The Lancet , 388 (10042), 412-436.
Transgender people are a diverse population affected by a range of negative health indicators across high-income, middle-income, and low-income settings. Studies consistently document a high prevalence of adverse health outcomes in this population, including HIV and other sexually transmitted infections, mental health distress, and substance use and abuse. However, many other health areas remain understudied, population-based representative samples and longitudinal studies are few, and routine surveillance efforts for transgender population health are scarce. The absence of survey items with which to identify transgender respondents in general surveys often restricts the availability of data with which to estimate the magnitude of health inequities and characterise the population-level health of transgender people globally. Despite the limitations, there are sufficient data highlighting the unique biological, behavioural, social, and structural contextual factors surrounding health risks and resiliencies for transgender people. To mitigate these risks and foster resilience, a comprehensive approach is needed that includes gender affirmation as a public health framework, improved health systems and access to health care informed by high quality data, and effective partnerships with local transgender communities to ensure responsiveness of and cultural specificity in programming. Consideration of transgender health underscores the need to explicitly consider sex and gender pathways in epidemiological research and public health surveillance more broadly.
Schmidt and Levine, 2015

Schmidt, L., & Levine, R. (2015). Psychological Outcomes and Reproductive Issues Among Gender Dysphoric Individuals. Endocrinology and Metabolism Clinics of North America , 44 (4), 773-785.
Gender dysphoria is a condition in which a person experiences discrepancy between the natal anatomic sex and the gender he or she identifies with, resulting in internal distress and a desire to live as the preferred gender. There is increasing demand for treatment, which includes suppression of puberty, cross-sex hormone therapy, and sex reassignment surgery. This article reviews longitudinal outcome data evaluating psychological well-being and quality of life among transgender individuals who have undergone cross-sex hormone treatment or sex reassignment surgery. Proposed methodologies for diagnosis and initiation of treatment are discussed, and the effects of cross-sex hormones and sex reassignment surgery on future reproductive potential.
White Hughto and Reisner, 2016

White Hughto, J. M., & Reisner, S. L. (2016). A systematic review of the effects of hormone therapy on psychological functioning and quality of life in transgender individuals. Transgender Health , 1 (1), 21–31.
Objectives: To review evidence from prospective cohort studies of the relationship between hormone therapy and changes in psychological functioning and quality of life in transgender individuals accessing hormone therapy over time. Data Sources: MEDLINE, PsycINFO, and PubMed were searched for relevant studies from inception to November 2014. Reference lists of included studies were hand searched. Results: Three uncontrolled prospective cohort studies, enrolling 247 transgender adults (180 male-to-female [MTF], 67 female-to-male [FTM]) initiating hormone therapy for the treatment of gender identity disorder (prior diagnostic term for gender dysphoria), were identified. The studies measured exposure to hormone therapy and subsequent changes in mental health (e.g., depression, anxiety) and quality of life outcomes at follow-up. Two studies showed a significant improvement in psychological functioning at 3–6 months and 12 months compared with baseline after initiating hormone therapy. The third study showed improvements in quality of life outcomes 12 months after initiating hormone therapy for FTM and MTF participants; however, only MTF participants showed a statistically significant increase in general quality of life after initiating hormone therapy. Conclusions: Hormone therapy interventions to improve the mental health and quality of life in transgender people with gender dysphoria have not been evaluated in controlled trials. Low quality evidence suggests that hormone therapy may lead to improvements in psychological functioning. Prospective controlled trials are needed to investigate the effects of hormone therapy on the mental health of transgender people.
Share this:
Numbers, Facts and Trends Shaping Your World
Read our research on:
Full Topic List
Regions & Countries
- Publications
- Our Methods
- Short Reads
- Tools & Resources
Read Our Research On:

The Experiences, Challenges and Hopes of Transgender and Nonbinary U.S. Adults
Findings from pew research center focus groups, table of contents, identity and the gender journey, navigating gender day-to-day, seeking medical care for gender transitions , connections with the broader lgbtq+ community, policy and social change.
- Focus groups
- The American Trends Panel survey methodology
- Panel recruitment
- Sample design
- Questionnaire development and testing
- Data collection protocol
- Data quality checks
- Acknowledgments
Introduction
Transgender and nonbinary people have gained visibility in the U.S. in recent years as celebrities from Laverne Cox to Caitlyn Jenner to Elliot Page have spoken openly about their gender transitions. On March 30, 2022, the White House issued a proclamation recognizing Transgender Day of Visibility , the first time a U.S. president has done so.
More recently, singer and actor Janelle Monáe came out as nonbinary , while the U.S. State Department and Social Security Administration announced that Americans will be allowed to select “X” rather than “male” or “female” for their sex marker on their passport and Social Security applications.
At the same time, several states have enacted or are considering legislation that would limit the rights of transgender and nonbinary people . These include bills requiring people to use public bathrooms that correspond with the sex they were assigned at birth, prohibiting trans athletes from competing on teams that match their gender identity, and restricting the availability of health care to trans youth seeking to medically transition.
A new Pew Research Center survey finds that 1.6% of U.S. adults are transgender or nonbinary – that is, their gender is different from the sex they were assigned at birth. This includes people who describe themselves as a man, a woman or nonbinary, or who use terms such as gender fluid or agender to describe their gender. While relatively few U.S. adults are transgender, a growing share say they know someone who is (44% today vs. 37% in 2017 ). One-in-five say they know someone who doesn’t identify as a man or woman.
In order to better understand the experiences of transgender and nonbinary adults at a time when gender identity is at the center of many national debates, Pew Research Center conducted a series of focus groups with trans men, trans women and nonbinary adults on issues ranging from their gender journey, to how they navigate issues of gender in their day-to-day life, to what they see as the most pressing policy issues facing people who are trans or nonbinary. This is part of a larger study that includes a survey of the general public on their attitudes about gender identity and issues related to people who are transgender or nonbinary.
The terms transgender and trans are used interchangeably throughout this essay to refer to people whose gender is different from the sex they were assigned at birth. This includes, but is not limited to, transgender men (that is, men who were assigned female at birth) and transgender women (women who were assigned male at birth).
Nonbinary adults are defined here as those who are neither a man nor a woman or who aren’t strictly one or the other. While some nonbinary focus group participants sometimes use different terms to describe themselves, such as “gender queer,” “gender fluid” or “genderless,” all said the term “nonbinary” describes their gender in the screening questionnaire. Some, but not all, nonbinary participants also consider themselves to be transgender.
References to gender transitions relate to the process through which trans and nonbinary people express their gender as different from social expectations associated with the sex they were assigned at birth. This may include social, legal and medical transitions. The social aspect of a gender transition may include going by a new name or using different pronouns, or expressing their gender through their dress, mannerisms, gender roles or other ways. The legal aspect may include legally changing their name or changing their sex or gender designation on legal documents or identification. Medical care may include treatments such as hormone therapy, laser hair removal and/or surgery.
References to femme indicate feminine gender expression. This is often in contrast to “masc,” meaning masculine gender expression.
Cisgender is used to describe people whose gender matches the sex they were assigned at birth and who do not identify as transgender or nonbinary.
Misgendering is defined as referring to or addressing a person in ways that do not align with their gender identity, including using incorrect pronouns, titles (such as “sir” or “ma’am”), and other terms (such as “son” or “daughter”) that do not match their gender.
References to dysphoria may include feelings of distress due to the mismatch of one’s gender and sex assigned at birth, as well as a diagnosis of gender dysphoria , which is sometimes a prerequisite for access to health care and medical transitions.
The acronym LGBTQ+ refers to lesbian, gay, bisexual, transgender, queer (or, in some cases, questioning), and other sexual orientations or gender identities that are not straight or cisgender, such as intersex, asexual or pansexual.
Pew Research Center conducted this research to better understand the experiences and views of transgender and nonbinary U.S. adults. Because transgender and nonbinary people make up only about 1.6% of the adult U.S. population, this is a difficult population to reach with a probability-based, nationally representative survey. As an alternative, we conducted a series of focus groups with trans and nonbinary adults covering a variety of topics related to the trans and nonbinary experience. This allows us to go more in-depth on some of these topics than a survey would typically allow, and to share these experiences in the participants’ own words.
For this project, we conducted six online focus groups, with a total of 27 participants (four to five participants in each group), from March 8-10, 2022. Participants were recruited by targeted email outreach among a panel of adults who had previously said on a survey that they were transgender or nonbinary, as well as via connections through professional networks and LGBTQ+ organizations, followed by a screening call. Candidates were eligible if they met the technology requirements to participate in an online focus group and if they either said they consider themselves to be transgender or if they said their gender was nonbinary or another identity other than man or woman (regardless of whether or not they also said they were transgender). For more details, see the Methodology .
Participants who qualified were placed in groups as follows: one group of nonbinary adults only (with a nonbinary moderator); one group of trans women only (with a trans woman moderator); one group of trans men only (with a trans man moderator); and three groups with a mix of trans and nonbinary adults (with either a nonbinary moderator or a trans man moderator). All of the moderators had extensive experience facilitating groups, including with transgender and nonbinary participants.
The participants were a mix of ages, races/ethnicities, and were from all corners of the country. For a detailed breakdown of the participants’ demographic characteristics, see the Methodology .
The findings are not statistically representative and cannot be extrapolated to wider populations.
Some quotes have been lightly edited for clarity or to remove identifying details. In this essay, participants are identified as trans men, trans women, or nonbinary adults based on their answers to the screening questionnaire. These words don’t necessarily encompass all of the ways in which participants described their gender. Participants’ ages are grouped into the following categories: late teens; early/mid/late 20s, 30s and 40s; and 50s and 60s (those ages 50 to 69 were grouped into bigger “buckets” to better preserve their anonymity).
These focus groups were not designed to be representative of the entire population of trans and nonbinary U.S. adults, but the participants’ stories provide a glimpse into some of the experiences of people who are transgender and/or nonbinary. The groups included a total of 27 transgender and nonbinary adults from around the U.S. and ranging in age from late teens to mid-60s. Most currently live in an urban area, but about half said they grew up in a suburb. The groups included a mix of White, Black, Hispanic, Asian and multiracial American participants. See Methodology for more details.
Most focus group participants said they knew from an early age – many as young as preschool or elementary school – that there was something different about them, even if they didn’t have the words to describe what it was. Some described feeling like they didn’t fit in with other children of their sex but didn’t know exactly why. Others said they felt like they were in the wrong body.
“I remember preschool, [where] the boys were playing on one side and the girls were playing on the other, and I just had a moment where I realized what side I was supposed to be on and what side people thought I was supposed to be on. … Yeah, I always knew that I was male, since my earliest memories.” – Trans man, late 30s
“As a small child, like around kindergarten [or] first grade … I just was [fascinated] by how some people were small girls, and some people were small boys, and it was on my mind constantly. And I started to feel very uncomfortable, just existing as a young girl.” – Trans man, early 30s
“I was 9 and I was at day camp and I was changing with all the other 9-year-old girls … and I remember looking at everybody’s body around me and at my own body, and even though I was visually seeing the exact shapeless nine-year-old form, I literally thought to myself, ‘oh, maybe I was supposed to be a boy,’ even though I know I wasn’t seeing anything different. … And I remember being so unbothered by the thought, like not a panic, not like, ‘oh man, I’m so different, like everybody here I’m so different and this is terrible,’ I was like, ‘oh, maybe I was supposed to be a boy,’ and for some reason that exact quote really stuck in my memory.” – Nonbinary person, late 30s
“Since I was little, I felt as though I was a man who, when they were passing out bodies, someone made a goof and I got a female body instead of the male body that I should have had. But I was forced by society, especially at that time growing up, to just make my peace with having a female body.” – Nonbinary person, 50s
“I’ve known ever since I was little. I’m not really sure the age, but I just always knew when I put on boy clothes, I just felt so uncomfortable.” – Trans woman, late 30s
“It was probably as early as I can remember that I wasn’t like my brother or my father [and] not exactly like my girl cousins but I was something else, but I didn’t know what it was.” – Nonbinary person, 60s
Many participants were well into adulthood before they found the words to describe their gender. For those focus group participants, the path to self-discovery varied. Some described meeting someone who was transgender and relating to their experience; others described learning about people who are trans or nonbinary in college classes or by doing their own research.
“I read a Time magazine article … called ‘Homosexuality in America’ … in 1969. … Of course, we didn’t have language like we do now or people were not willing to use it … [but] it was kind of the first word that I had ever heard that resonated with me at all. So, I went to school and I took the magazine, we were doing show-and-tell, and I stood up in front of the class and said, ‘I am a homosexual.’ So that began my journey to figure this stuff out.” – Nonbinary person, 60s
“It wasn’t until maybe I was 20 or so when my friend started his transition where I was like, ‘Wow, that sounds very similar to the emotions and challenges I am going through with my own identity.’ … My whole life from a very young age I was confused, but I didn’t really put a name on it until I was about 20.” – Nonbinary person, late 20s
“I knew about drag queens, but I didn’t know what trans was until I got to college and was exposed to new things, and that was when I had a word for myself for the first time.” – Trans man, early 40s
“I thought that by figuring out that I was interested in women, identifying as lesbian, I thought [my anxiety and sadness] would dissipate in time, and that was me cracking the code. But then, when I got older, I left home for the first time. I started to meet other trans people in the world. That’s when I started to become equipped with the vocabulary. The understanding that this is a concept, and this makes sense. And that’s when I started to understand that I wasn’t cisgender.” – Trans man, early 30s
“When I took a human sexuality class in undergrad and I started learning about gender and different sexualities and things like that, I was like, ‘oh my god. I feel seen.’ So, that’s where I learned about it for the first time and started understanding how I identify.” – Nonbinary person, mid-20s
Focus group participants used a wide range of words to describe how they see their gender. For many nonbinary participants, the term “nonbinary” is more of an umbrella term, but when it comes to how they describe themselves, they tend to use words like “gender queer” or “gender fluid.” The word “queer” came up many times across different groups, often to describe anyone who is not straight or cisgender. Some trans men and women preferred just the terms “man” or “woman,” while some identified strongly with the term “transgender.” The graphic below shows just some of the words the participants used to describe their gender.
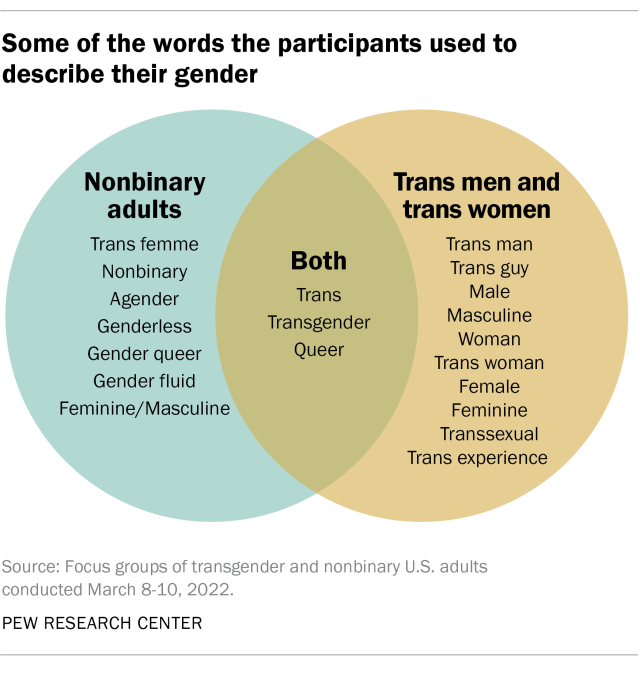
The way nonbinary people conceptualize their gender varies. Some said they feel like they’re both a man and a woman – and how much they feel like they are one or the other may change depending on the day or the circumstance. Others said they don’t feel like they are either a man or a woman, or that they don’t have a gender at all. Some, but not all, also identified with the term transgender.
“I had days where I would go out and just play with the boys and be one of the boys, and then there would be times that I would play with the girls and be one of the girls. And then I just never really knew what I was. I just knew that I would go back and forth.” – Nonbinary person, mid-20s
“Growing up with more of a masculine side or a feminine side, I just never was a fan of the labelling in terms of, ‘oh, this is a bit too masculine, you don’t wear jewelry, you don’t wear makeup, oh you’re not feminine enough.’ … I used to alternate just based on who I felt I was. So, on a certain day if I felt like wearing a dress, or a skirt versus on a different day, I felt like wearing what was considered men’s pants. … So, for me it’s always been both.” – Nonbinary person, mid-30s
“I feel like my gender is so amorphous and hard to hold and describe even. It’s been important to find words for it, to find the outlines of it, to see the shape of it, but it’s not something that I think about as who I am, because I’m more than just that.” – Nonbinary person, early 30s
“What words would I use to describe me? Genderless, if gender wasn’t a thing. … I guess if pronouns didn’t exist and you just called me [by my name]. That’s what my gender is. … And I do use nonbinary also, just because it feels easier, I guess.” – Nonbinary person, late 20s
Some participants said their gender is one of the most important parts of their identity, while others described it as one of many important parts or a small piece of how they see themselves. For some, the focus on gender can get tiring. Those who said gender isn’t a central – or at least not the most central – part of their identity mentioned race, ethnicity, religion and socioeconomic class as important aspects that shape their identity and experiences.
“It is tough because [gender] does affect every factor of your life. If you are doing medical transitioning then you have appointments, you have to pay for the appointments, you have to be working in a job that supports you to pay for those appointments. So, it is definitely integral, and it has a lot of branches. And it deals with how you act, how you relate to friends, you know, I am sure some of us can relate to having to come out multiple times in our lives. That is why sexuality and gender are very integral and I would definitely say I am proud of it. And I think being able to say that I am proud of it, and my gender, I guess is a very important part of my identity.” – Nonbinary person, late 20s
“Sometimes I get tired of thinking about my gender because I am actively [undergoing my medical transition]. So, it is a lot of things on my mind right now, constantly, and it sometimes gets very tiring. I just want to not have to think about it some days. So, I would say it’s, it’s probably in my top three [most important parts of my identity] – parent, Black, queer nonbinary.” – Nonbinary person, mid-40s
“I live in a town with a large queer and trans population and I don’t have to think about my gender most of the time other than having to come out as trans. But I’m poor and that colors everything. It’s not a chosen part of my identity but that part of my identity is a lot more influential than my gender.” – Trans man, early 40s
“My gender is very important to my identity because I feel that they go hand in hand. Now my identity is also broken down into other factors [like] character, personality and other stuff that make up the recipe for my identity. But my gender plays a big part of it. … It is important because it’s how I live my life every day. When I wake up in the morning, I do things as a woman.” – Trans woman, mid-40s
“I feel more strongly connected to my other identities outside of my gender, and I feel like parts of it’s just a more universal thing, like there’s a lot more people in my socioeconomic class and we have much more shared experiences.” – Trans man, late 30s
Some participants spoke about how their gender interacted with other aspects of their identity, such as their race, culture and religion. For some, being transgender or nonbinary can be at odds with other parts of their identity or background.
“Culturally I’m Dominican and Puerto Rican, a little bit of the macho machismo culture, in my family, and even now, if I’m going to be a man, I’ve got to be a certain type of man. So, I cannot just be who I’m meant to be or who I want myself to be, the human being that I am.” – Trans man, mid-30s
“[Judaism] is a very binary religion. There is a lot of things like for men to do and a lot of things for women to do. … So, it is hard for me now as a gender queer person, right, to connect on some levels with [my] religion … I have just now been exposed to a bunch of trans Jewish spaces online which is amazing.” – Nonbinary person, mid-40s
“Just being Indian American, I identify and love aspects of my culture and ethnicity, and I find them amazing and I identify with that, but it’s kind of separated. So, I identify with the culture, then I identify here in terms of gender and being who I am, but I kind of feel the necessity to separate the two, unfortunately.” – Nonbinary person, mid-30s
“I think it’s really me being a Black woman or a Black man that can sometimes be difficult. And also, my ethnic background too. It’s really rough for me with my family back home and things of that nature.” – Nonbinary person, mid-20s
For some, deciding how open to be about their gender identity can be a constant calculation. Some participants reported that they choose whether or not to disclose that they are trans or nonbinary in a given situation based on how safe or comfortable they feel and whether it’s necessary for other people to know. This also varies depending on whether the participant can easily pass as a cisgender man or woman (that is, they can blend in so that others assume them to be cisgender and don’t recognize that they are trans or nonbinary).
“It just depends on whether I feel like I have the energy to bring it up, or if it feels worth it to me like with doctors and stuff like that. I always bring it up with my therapists, my primary [care doctor], I feel like she would get it. I guess it does vary on the situation and my capacity level.” – Nonbinary person, late 20s
“I decide based on the person and based on the context, like if I feel comfortable enough to share that piece of myself with them, because I do have the privilege of being able to move through the world and be identified as cis[gender] if I want to. But then it is important to me – if you’re important to me, then you will know who I am and how I identify. Otherwise, if I don’t feel comfortable or safe then I might not.” – Nonbinary person, early 30s
“The expression of my gender doesn’t vary. Who I let in to know that I was formerly female – or formerly perceived as female – is kind of on a need to know basis.” – Trans man, 60s
“It’s important to me that people not see me as cis[gender], so I have to come out a lot when I’m around new people, and sometimes that’s challenging. … It’s not information that comes out in a normal conversation. You have to force it and that’s difficult sometimes.” – Trans man, early 40s
Work is one realm where many participants said they choose not to share that they are trans or nonbinary. In some cases, this is because they want to be recognized for their work rather than the fact that they are trans or nonbinary; in others, especially for nonbinary participants, they fear it will be perceived as unprofessional.
“It’s gotten a lot better recently, but I feel like when you’re nonbinary and you use they/them pronouns, it’s just seen as really unprofessional and has been for a lot of my life.” – Nonbinary person, early 30s
“Whether it’s LinkedIn or profiles [that] have been updated, I’ve noticed people’s resumes have their pronouns now. I don’t go that far because I just feel like it’s a professional environment, it’s nobody’s business.” – Nonbinary person, mid-30s
“I don’t necessarily volunteer the information just to make it public; I want to be recognized for my character, my skill set, in my work in other ways.” – Trans man, early 30s
Some focus group participants said they don’t mind answering questions about what it’s like to be trans or nonbinary but were wary of being seen as the token trans or nonbinary person in their workplace or among acquaintances. Whether or not they are comfortable answering these types of questions sometimes depends on who’s asking, why they want to know, and how personal the questions get.
“I’ve talked to [my cousin about being trans] a lot because she has a daughter, and her daughter wants to transition. So, she always will come to me asking questions.” – Trans woman, early 40s
“It is tough being considered the only resource for these topics, right? In my job, I would hate to call myself the token nonbinary, but I was the first nonbinary person that they hired and they were like, ‘Oh, my gosh, let me ask you all the questions as you are obviously the authority on the subject.’ And it is like, ‘No, that is a part of me, but there are so many other great resources.’” – Nonbinary person, late 20s
“I don’t want to be the token. I’m not going to be no spokesperson. If you have questions, I’m the first person you can ask. Absolutely. I don’t mind discussing. Ask me some of the hardest questions, because if you ask somebody else you might get you know your clock cleaned. So, ask me now … so you can be educated properly. Otherwise, I don’t believe it’s anybody’s business.” – Trans woman, early 40s
Most nonbinary participants said they use “they/them” as their pronouns, but some prefer alternatives. These alternatives include a combination of gendered and gender-neutral pronouns (like she/they) or simply preferring that others use one’s names rather than pronouns.
“If I could, I would just say my name is my pronoun, which I do in some spaces, but it just is not like a larger view. It feels like I’d rather have less labor on me in that regard, so I just say they/them.” – Nonbinary person, late 20s
“For me personally, I don’t get mad if someone calls me ‘he’ because I see what they’re looking at. They look and they see a guy. So, I don’t get upset. I know a few people who do … and they correct you. Me, I’m a little more fluid. So, that’s how it works for me.” – Nonbinary person, mid-30s
“I use they/she pronouns and I put ‘they’ first because that is what I think is most comfortable and it’s what I want to draw people’s attention to, because I’m 5 feet tall and 100 pounds so it’s not like I scream masculine at first sight, so I like putting ‘they’ first because otherwise people always default to ‘she.’ But I have ‘she’ in there, and I don’t know if I’d have ‘she’ in there if I had not had kids.” – Nonbinary person, late 30s
“Why is it so hard for people to think of me as nonbinary? I choose not to use only they/them pronouns because I do sometimes identify with ‘she.’ But I’m like, ‘Do I need to use they/them pronouns to be respected as nonbinary?’ Sometimes I feel like I should do that. But I don’t want to feel like I should do anything. I just want to be myself and have that be accepted and respected.” – Nonbinary person, early 30s
“I have a lot of patience for people, but [once someone in public used] they/them pronouns and I thanked them and they were like, ‘Yeah, I just figure I’d do it when I don’t know [someone’s] pronouns.’ And I’m like, ‘I love it, thank you.’” – Nonbinary person, early 30s
Transgender and nonbinary participants find affirmation of their gender identity and support in various places. Many cited their friends, chosen families (and, less commonly, their relatives), therapists or other health care providers, religion, or LGBTQ+ spaces as sources of support.
“I’m just not close with my family [of origin], but I have a huge chosen family that I love and that fully respects my identity.” – Nonbinary person, early 30s
“Before the pandemic I used to go out to bars a lot; there’s a queer bar in my town and it was a really nice place just being friends with everybody who went and everybody who worked there, it felt really nice you know, and just hearing everybody use the right pronouns for me it just felt really good.” – Nonbinary person, early 30s
“I don’t necessarily go to a lot of dedicated support groups, but I found that there’s kind of a good amount of support in areas or groups or fandoms for things that have a large LGBT population within them. Like certain shows or video games, where it’s just kind of a joke that all the gay people flock to this.” – Trans woman, late teens
“Being able to practice my religion in a location with a congregation that is just completely chill about it, or so far has been completely chill about it, has been really amazing.” – Nonbinary person, late 30s
Many participants shared specific moments they said were small in the grand scheme of things but made them feel accepted and affirmed. Examples included going on dates, gestures of acceptance by a friend or social group, or simply participating in everyday activities.
“I went on a date with a really good-looking, handsome guy. And he didn’t know that I was trans. But I told him, and we kept talking and hanging out. … That’s not the first time that I felt affirmed or felt like somebody is treating me as I present myself. But … he made me feel wanted and beautiful.” – Trans woman, late 30s
“I play [on a men’s rec league] hockey [team]. … I joined the league like right when I first transitioned and I showed up and I was … nervous with locker rooms and stuff, and they just accepted me as male right away.” – Trans man, late 30s
“I ended up going into a barbershop. … The barber was very welcoming, and talked to me as if I was just a casual customer and there was something that clicked within that moment where, figuring out my gender identity, I just wanted to exist in the world to do these natural things like other boys and men would do. So, there was just something exciting about that. It wasn’t a super macho masculine moment, … he just made me feel like I blended in.” – Trans man, early 30s
Participants also talked about negative experiences, such as being misgendered, either intentionally or unintentionally. For example, some shared instances where they were treated or addressed as a gender other than the gender that they identify as, such as people referring to them as “he” when they go by “she,” or where they were deadnamed, meaning they were called by the name they had before they transitioned.
“I get misgendered on the phone a lot and that’s really annoying. And then, even after I correct them, they keep doing it, sometimes on purpose and sometimes I think they’re just reading a script or something.” – Trans man, late 30s
“The times that I have been out, presenting femme, there is this very subconscious misgendering that people do and it can be very frustrating. [Once, at a restaurant,] I was dressed in makeup and nails and shoes and everything and still everyone was like, ‘Sir, what would you like?’ … Those little things – those microaggressions – they can really eat away at people.” – Nonbinary person, mid-40s
“People not calling me by the right name. My family is a big problem, they just won’t call me by my name, you know? Except for my nephew, who is of the Millennial generation, so at least he gets it.” – Nonbinary person, 60s
“I’m constantly misgendered when I go out places. I accept this – because of the way I look, people are going to perceive me as a woman and it doesn’t cause me huge dysphoria or anything, it’s just nice that the company that I keep does use the right pronouns.” – Nonbinary person, early 30s
Some participants also shared stories of discrimination, bias, humiliation, and even violence. These experiences ranged from employment discrimination to being outed (that is, someone else disclosing the fact that they are transgender or nonbinary without their permission) without their permission to physical attacks.
“I was on a date with this girl and I had to use the bathroom … and the janitor … wouldn’t let me use the men’s room, and he kept refusing to let me use the men’s room, so essentially, I ended up having to use the same bathroom as my date.” – Trans man, late 30s
“I’ve been denied employment due to my gender identity. I walked into a supermarket looking for jobs. … And they flat out didn’t let me apply. They didn’t even let me apply.” – Trans man, mid-30s
“[In high school,] this group of guys said, ‘[name] is gay.’ I ignored them but they literally threw me and tore my shirt from my back and pushed me to the ground and tried to strip me naked. And I had to fight for myself and use my bag to hit him in the face.” – Trans woman, late 20s
“I took a college course [after] I had my name changed legally and the instructor called me out in front of the class and called me a liar and outed me.” – Trans man, late 30s
Many, but not all, participants said they have received medical care , such as surgery or hormone therapy, as part of their gender transition. For those who haven’t undergone a medical transition, the reasons ranged from financial barriers to being nervous about medical procedures in general to simply not feeling that it was the right thing for them.
“For me to really to live my truth and live my identity, I had to have the surgery, which is why I went through it. It doesn’t mean [that others] have to, or that it will make you more or less of a woman because you have it. But for me to be comfortable, … that was a big part of it. And so, that’s why I felt I had to get it.” – Trans woman, early 40s
“I’m older and it’s an operation. … I’m just kind of scared, I guess. I’ve never had an operation. I mean, like any kind of operation. I’ve never been to the hospital or anything like that. So, it [is] just kind of scary. But I mean, I want to. I think about all the time. I guess have got to get the courage up to do it.” – Trans woman, early 40s
“I’ve decided that the dysphoria of a second puberty … would just be too much for me and I’m gender fluid enough where I’m happy, I guess.” – Nonbinary person, early 30s
“I’m too old to change anything, I mean I am what I am. [laughs]” – Nonbinary person, 60s
Many focus group participants who have sought medical treatment for their gender transition faced barriers, although some had positive experiences. For those who said there were barriers, the cost and the struggle to find sympathetic doctors were often cited as challenges.
“I was flat out turned down by the primary care physician who had to give the go-ahead to give me a referral to an endocrinologist; I was just shut down. That was it, end of story.” – Nonbinary person, 50s
“I have not had surgery, because I can’t access surgery. So unless I get breast cancer and have a double mastectomy, surgery is just not going to happen … because my health insurance wouldn’t cover something like that. … It would be an out-of-pocket plastic surgery expense and I can’t afford that at this time.” – Nonbinary person, 50s
“Why do I need the permission of a therapist to say, ‘This person’s identity is valid,’ before I can get the health care that I need to be me, that is vital for myself and for my way of life?” – Nonbinary person, mid-40s
“[My doctor] is basically the first person that actually embraced me and made me accept [who I am].” – Trans woman, late 20s
Many people who transitioned in previous decades described how access has gotten much easier in recent years. Some described relying on underground networks to learn which doctors would help them obtain medical care or where to obtain hormones illegally.
“It was hard financially because I started so long ago, just didn’t have access like that. Sometimes you have to try to go to Mexico or learn about someone in Mexico that was a pharmacist, I can remember that. That was a big thing, going through the border to Mexico, that was wild. So, it was just hard financially because they would charge so much for testosterone. And there was the whole bodybuilding community. If you were transitioning, you went to bodybuilders, and they would charge you five times what they got it [for], so it was kind of tough.” – Trans man, early 40s
“It was a lot harder to get a surgeon when I started transitioning; insurance was out of the question, there wasn’t really a national discussion around trans people and their particular medical needs. So, it was challenging having to pay everything out of pocket at a young age.” – Trans man, early 30s
“I guess it was hard for me to access hormones initially just because you had to jump through so many hoops, get letters, and then you had to find a provider that was willing to write it. And now it’s like people are getting it from their primary care doctor, which is great, but a very different experience than I had.” – Trans man, early 40s
The discussions also touched on whether the participants feel a connection with a broader lesbian, gay, bisexual, transgender, and queer (LGBTQ+) community or with other people who are LGBTQ+. Views varied, with some saying they feel an immediate connection with other people who are LGBTQ+, even with those who aren’t trans or nonbinary, and others saying they don’t necessarily feel this way.
“It’s kind of a recurring joke where you can meet another LGBT person and it is like there is an immediate understanding, and you are basically talking and giving each other emotional support, like you have been friends for 10-plus years.” – Trans woman, late teens
“I don’t think it’s automatic friendship between queer people, there’s like a kinship, but I don’t think there’s automatic friendship or anything. I think it’s just normal, like, how normal people make friends, just based on common interests.” – Nonbinary person, early 30s
“I do think of myself as part of the LGBT [community] … I use the resources that are put in place for these communities, whether that’s different health care programs, support groups, they have the community centers. … So, I do consider myself to be part of this community, and I’m able to hopefully take when needed, as well as give back.” – Trans man, mid-30s
“I feel like that’s such an important part of being a part of the [LGBTQ+] alphabet soup community, that process of constantly learning and listening to each other and … growing and developing language together … I love that aspect of creating who we are together, learning and unlearning together, and I feel like that’s a part of at least the queer community spaces that I want to be in. That’s something that’s core to me.” – Nonbinary person, early 30s
“I identify as queer. I feel like I’m a part of the LGBT community. That’s more of a part of my identity than being trans. … Before I came out as trans, I identified as a lesbian. That was also a big part of my identity. So, that may be too why I feel like I’m more part of the LGB community.” – Trans man, early 40s
While many trans and nonbinary participants said they felt accepted by others in the LGBTQ+ community, some participants described their gender identity as a barrier to full acceptance. There was a sense among some participants that cisgender people who are lesbian, gay or bisexual don’t always accept people who are transgender or nonbinary.
“I would really like to be included in the [LGBTQ+] community. But I have seen some people try to separate the T from LGB … I’ve run into a few situations throughout my time navigating the [LGBTQ+] community where I’ve been perceived – and I just want to say that there’s nothing wrong with this – I’ve been perceived as like a more feminine or gay man in a social setting, even though I’m heterosexual. … But the minute that that person found out that I wasn’t a gay man … and that I was actually a transgender person, they became cold and just distancing themselves. And I’ve been in a lot of those types of circumstances where there’s that divide between the rest of the community.” – Trans man, early 30s
“There are some lesbians who see trans men as being traitors to womanhood. Those are not people that I really identify with or want to be close to.” – Trans man, early 40s
“It’s only in the past maybe dozen or so years, that an identity like gender fluid or gender queer was acceptable even within the LGBTQ+ community. … I tried to go to certain LGBTQ+ events as a trans man and, you know, I was not allowed in because I looked too female. The gay men would not allow me to participate.” – Nonbinary person, 50s
“Technically based on the letters [in the acronym LGBTQ+] I am part of that community, but I’ve felt discrimination, it’s very heavily exclusive to people who are either gay or lesbian and I think that’s true … for queer or bisexual or asexual, intersex … anybody who’s not like exclusively hardcore gay or lesbian. It’s very exclusive, like excluding to those people. … I feel like the BTQ is a separate group of people…. So, I identify with the second half of the letters as a separate subset.” – Trans man, late 30s
When asked to name the most important policy or political issues facing transgender and nonbinary people in the United States today, many participants named basic needs such as housing, employment, and health care. Others cited recent legislation or policies related to people who are transgender that have made national news.
“Housing is a huge issue. Health care might be good in New York, it might be good in California, but … it’s not a national equality for trans folks. Health care is not equal across the states. Housing is not equal across the states. So, I think that the issues right now that we’re all facing is health care and housing. That’s the top, the most important things.” – Trans woman, early 40s
“Definitely education. I think that’s very important … Whether you identify as trans or not as a young child, it’s good to understand and know the different things under the umbrella, the queer umbrella. And it is also just a respect thing. And also, the violence that happens against trans and nonbinary people. I feel like educating them very young, that kind of helps – well, it is going to help because once you understand what’s going on and you see somebody that doesn’t identify the same as you, you’ll have that respect, or you’ll have that understanding and you’re less likely to be very violent towards them.” – Nonbinary person, mid-20s
“Employment is a big one. And I know that some areas, more metropolitan progressive-leaning areas, are really on top of this, but they’re trans people everywhere that are still being discriminated against. I think it’s a personal thing for me that goes back to my military service, but still, it’s just unfortunate. It’s an unfortunate reality.” – Trans man, early 30s
“I think just the strong intersectionality of trans people with mental health issues, or even physical health issues. … So in that way, accessing good health care or having good mental health.” – Trans man, late 30s
“I honestly think that the situation in Texas is the most pressing political and policy situation because it is a direct attack on the trans community. … And it is so insidious because it doesn’t just target bathrooms. This is saying that if you provide medical care to trans youth it is tantamount to child abuse. And it is so enraging because it is a known proven fact that access to gender affirming medical care saves lives. It saves the lives of trans youth. And trans youth have the highest suicide rate in the country.” – Nonbinary person, mid-40s
Participants had different takes on what gets in the way of progress on issues facing transgender and nonbinary people. Some pointed to the lack of knowledge surrounding the history of these issues or not knowing someone who is transgender or nonbinary. Others mentioned misconceptions people might have about transgender and nonbinary people that influence their political and policy perspectives.
“People who don’t know trans people, honestly … that’s the only barrier I can understand because people fear what they don’t know and then react to it a lot of the time.” – Nonbinary person, early 30s
“Sometimes even if they know someone, they still don’t consider them to be a human being, they are an ‘other,’ they are an ‘it,’ they are a ‘not like me,’ ‘not like my family,’ person and so they are put into a place socially where they can be treated badly.” – Nonbinary person, 50s
“Just the ignorance and misinformation and this quick fake social media fodder, where it encourages people who should not be part of the conversation to spread things that are not true.” – Trans man, late 30s
“Also, the political issues that face nonbinary people, it’s that people think nonbinary is some made-up thing to feel cool. It’s not to feel cool. And if someone does do it to feel cool, maybe they’re just doing that because they don’t feel comfortable within themselves.” – Nonbinary person, mid-30s
“There’s so much fear around it, and misunderstanding, and people thinking that if you’re talking to kids about gender and sexuality, that it’s sexual. And it’s like, we really need to break down that our bodies are not inherently sexual. We need to be able to talk with students and children about their bodies so that they can then feel empowered to understand themselves, advocate for themselves.” – Nonbinary person, early 30s
When asked what makes them hopeful for the future for trans and nonbinary people, some participants pointed to the way things in society have already changed and progress that has been made. For example, some mentioned greater representation and visibility of transgender and nonbinary people in entertainment and other industries, while others focused on changing societal views as things that give them hope for the future.
“I am hopeful about the future because I see so many of us coming out and being visible and representing and showing folks that we are not to stereotype.” – Trans woman, early 40s
“Also, even though celebrity is annoying, it’s still cool when people like Willow [Smith] or Billie Eilish or all these popstars that the kids really love are like, ‘I’m nonbinary, I’m queer,’ like a lot more progressive. … Even just more visibility in TV shows and movies, the more and more that happens the more it’s like, ‘Oh yeah, we are really here, you can’t not see us.’” – Nonbinary person, late 20s
“We shouldn’t have to look to the entertainment industry for role models, we shouldn’t have to, we should be able to look to our leaders, our political leaders, but I think, that’s what gives me hope. Soon, it’s going to become a nonissue, maybe in my lifetime.” – Trans man, 60s
“I have gotten a little bit into stand-up comedy in the last few weeks, and it is like the jokes that people made ten years ago are resurfacing online and people are enraged about it. They are saying like, ‘Oh, this is totally inappropriate.’ But that comes with the recognition that things have changed, and language has changed, and people are becoming more intolerant of allowing these things to occur. So that is why I am hopeful, is being able to see that progression and hopeful continued improvement on that front.” – Nonbinary person, late 20s
“I think because of the shift of what’s happening, how everything has become so normal, and people are being more open, and within the umbrella of queerness so many different things are happening, I think as we get more comfortable and we progress as a society, it’s just going to be better. So, people don’t have to hide who they are. So, that gives me hope.” – Nonbinary person, mid-20s
For many, young people are a source of hope. Several participants talked about younger generations being more accepting of those who are transgender or nonbinary and also being more accepted by their families if they themselves are trans or nonbinary.
“And then the other portion that gives me hope are the kids, because I work now with so many kids who are coming out as trans earlier and their families are embracing them and everything. … So I really am trusting in the young generation.” – Nonbinary person, 60s
“I mean kids don’t judge you the same way as adults do about gender, and they’re so expansive and have so much creativity. … So it’s just the kids, Gen Z, and it just makes me feel really, really hopeful.” – Nonbinary person, early 30s
“The youth, the youth. They understand almost intrinsically so much more about these things than I feel like my generation did. They give me so much hope for the future.” – Nonbinary person, early 30s
“I think future generations, just seeing this growing amount of support that they have, that it’s just going to keep improving … there’s an increase in visibility but there’s also an increase in support … like resources for parents where they can see that they don’t have to punish their kids. Their kids can grow up feeling like, ‘This is okay to be this way.’ And I feel like that’s not something that can be stopped.” – Trans man, late 30s
Additional materials
- Methodology
Lead photo: (Angela Weiss/AFP via Getty Images)
1615 L St. NW, Suite 800 Washington, DC 20036 USA (+1) 202-419-4300 | Main (+1) 202-857-8562 | Fax (+1) 202-419-4372 | Media Inquiries
Research Topics
- Email Newsletters
ABOUT PEW RESEARCH CENTER Pew Research Center is a nonpartisan fact tank that informs the public about the issues, attitudes and trends shaping the world. It conducts public opinion polling, demographic research, media content analysis and other empirical social science research. Pew Research Center does not take policy positions. It is a subsidiary of The Pew Charitable Trusts .
© 2024 Pew Research Center
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- 10 June 2024
Beyond the trans/cis binary: introducing new terms will enrich gender research
- Florence Ashley 0 ,
- Shari Brightly-Brown 1 &
- G. Nic Rider 2
Florence Ashley (they/them) is an assistant professor at the Faculty of Law, University of Alberta and in the John Dossetor Health Ethics Centre, University of Alberta, Edmonton, Canada.
You can also search for this author in PubMed Google Scholar
Shari Brightly-Brown (they/them) is a postdoctoral fellow at the Institute for Sexual and Gender Health and in the National Center for Gender Health, University of Minnesota Medical School in Minneapolis.
G. Nic Rider (they/them) is an assistant professor at the Institute for Sexual and Gender Health and director of the National Center for Gender Health, University of Minnesota Medical School in Minneapolis.
Illustration: Sophi Gullbrants
You have full access to this article via your institution.
“Are you transgender?” Participating in a study for their public-health class, neither Alex nor Luna knew how to answer. Alex uses they/them pronouns and identifies as agender. They are also among a growing number of young people who have been raised in a gender-neutral manner: their parents did not refer to them as a boy or a girl until they were old enough to choose for themselves. Whatever genitals Alex was born with is not common knowledge. If you are agender and were never assigned a gender, does that make you transgender?
As for Luna, today she identifies as a woman, which aligns with the gender she was assigned at birth. But this is a recent development: Luna identified as a boy for as long as she can remember and, after coming out as trans, lived openly as one throughout her childhood and adolescence. As a woman who has detransitioned, she often feels that she has more in common with transgender women than with cisgender ones, whose gender identity corresponds to the gender they were assigned at birth. Although Luna doesn’t call herself transgender, she fears that answering ‘no’ to the study’s question means that her gender trajectory and experiences will be erased.
Collection: Sex and gender in science
The difficulties Alex and Luna experienced might seem unusual. But many individuals find themselves unmoored from binary terms such as male and female, or cis and trans 1 . In the United States, an estimated 9.2% of secondary-school students don’t wholly identify with the gender they were assigned at birth 2 , yet only 1.8% anonymously answer ‘yes’ when asked whether they are transgender 3 . These identities are not trivial. How people identify shapes not only their experiences of marginalization, but also their bodies — be it by influencing their smoking habits, whether they exercise, what they eat or whether they undergo hormone therapy or transition-related surgeries.
Human experiences are inevitably richer than the categories we carve out for them. But finding the right concepts and language to describe their diversity is an essential part of the scientific endeavour. It helps researchers to capture the experiences of participants more accurately, enhances analytical clarity and contributes to people feeling included and respected. Scientists need terms that are flexible enough to capture the nuances of people’s experience, that leave space for language to evolve and that are nonetheless pragmatic enough to be used in research.
Encompassing diversity
The term ‘gender modality’ could enable researchers to broaden their horizons.
A person’s gender identity is their sense of gender at any given time. By contrast, gender modality refers to how a person’s gender identity relates to the gender they were assigned at birth (see go.nature.com/3x34784 ). It is a mode or way of being one’s gender.
The best-known gender modalities are ‘cisgender’ and ‘transgender’, but the term allows for other possibilities, such as ‘agender’, which includes those who do not identify with any gender, and ‘detrans’ or ‘retrans’ for people who have ceased, shifted or reversed their gender transition. The term also makes space for gender modalities specific to intersex individuals, gender-questioning people, people with dissociative identity disorder and people with culture-specific identities (see ‘Many ways of being’). Gender modality serves a similar purpose to sexual orientation, which describes a facet of human existence and makes space for orientations beyond gay and straight.
Many ways of being
‘Gender modality’ refers to how a person’s gender identity relates to the gender they were assigned at birth, and includes options other than cisgender and transgender. This is not an exhaustive list.
Agender: people who do not identify with any gender.
Cisgender: people whose gender identity corresponds to the gender they were assigned at birth.
Closeted trans people: individuals whose gender identity does not correspond to the gender they were assigned at birth, but who do not share their gender identity publicly.
Culture-specific identities: individuals can have identities, such as Two-Spirit identities in North American Indigenous communities and hijra on the Indian subcontinent, that might not align with Western concepts of gender and sexuality. People with these identities might not consider themselves cis or trans because of the Western philosophies that underpin these terms.
Detrans/retrans: People who have ceased, shifted or reversed their gender transition.
Gender questioning: people who are unsure of their gender identity and are in the process of working it out.
Intersex: people who were born or who endogenously developed sexual traits that differ from typical expectations of female and male bodies. Some intersex people do not consider themselves to be cis or trans.
People with dissociative identity disorder whose alters have distinct gender identities: people with this condition, also known as plural people, can have several identities, known as alters or headmates, that have distinct gender identities. These alters can have different gender modalities.
Raised in a gender-neutral manner: people who were raised without being referred to as a boy/he or girl/she until they were old enough to express their gender identity.
Transgender: people whose gender identity does not correspond to the gender they were assigned at birth.
The term gender modality was coined in 2019 by one of us (F.A.) in response to frustrations felt as a trans bioethicist and jurist with the limits of existing language (see go.nature.com/3x34784 ). The term has since been used by transgender communities, clinicians and policymakers to describe the realities of trans communities and the heterogeneity of trans experiences. It is increasingly being used in trans health research 4 – 6 and has been included in official documentation by the government agency Statistics Canada (see go.nature.com/3wvzczw ); in educational materials by the US non-profit organization Planned Parenthood (see go.nature.com/4arxzuw ); and in decisions by the Supreme Court of Canada.
In our view, researchers can use gender modality to improve their work in three important ways.
First, scientists can expand the gamut of gender modalities included in questionnaires given to participants, to capture a broader range of experiences than those represented by the binary of cis and trans. Formulating new categories, adapted to the study design, will enhance the validity of the research 7 , 8 . It could also improve response rates and reduce the likelihood of people dropping out.

We need more-nuanced approaches to exploring sex and gender in research
Researchers who exclude possibilities beyond cis and trans typically rely on several tacit assumptions about bodies and social experiences. For instance, they might assume that participants whose gender identity corresponds to their gender assigned at birth are cisgender men and women — which would be incorrect for people, like Alex, who were raised in a wholly gender-neutral manner. Or they could assume that a person’s gender identity hasn’t changed across their lifespan and that they can infer certain facts about the participant’s body or medical history from their response — which would be incorrect for those, like Luna, who have detransitioned.
Other false assumptions could include the idea that every culture understands gender in a similar manner, that gender assigned at birth straightforwardly reflects anatomy at birth, that everyone has only one gender identity and that everyone can identify and communicate their gender identity.

This is not to say that every study should include every possible gender modality. The guiding principles are feasibility, necessity and respect. Sometimes, there are too few participants in a subgroup for researchers to analyse them separately. Moreover, some gender modalities could be irrelevant to the study question. For instance, it might not be necessary to include a detrans gender modality in a study if researchers are specifically interested in health outcomes among trans people. The point is to avoid uncritically assuming that the cis/trans binary suffices. It might, or it might not.
Capturing the human experience
The second way in which researchers can use gender modality to improve their work is by using it to refine how they phrase questions or discuss results.
By reflecting on gender modality, researchers can better ensure that participants feel respected, and can avoid assigning gender modalities that conflict with participants’ identities. Recognizing gender modalities beyond cis and trans is a matter of justice 9 . In some studies, offering write-in opportunities can help participants to feel respected despite the nuances of their experiences not being captured. But it could be as simple as using ‘gender modality’ instead of ‘gender identity’ or ‘transgender status’ in a table heading, because the last two terms can be seen as inaccurate or marginalizing.
Unlike terms such as transgender status, gender modality places cis, trans and other gender-expansive people on an equal footing. It reflects a universalizing conception of gender diversity 10 , in which everyone has a gender modality and being trans, detrans or cis comprises just some of the options in the vast expanse of human experience. This is important, given the long history of trans and gender non-conforming people being treated as deviant or abnormal.
Finally, researchers can use gender modality to think more meticulously about what it is that they are really trying to capture in their study.

Male–female comparisons are powerful in biomedical research — don’t abandon them
Linguistic gaps abound when it comes to our ability to describe trans people’s experiences. For instance, discrimination against trans people is often described as discrimination on the basis of gender identity. Although this shorthand might be workable, it is not entirely accurate. If a trans woman is fired for being trans, should we say that her gender identity was targeted when she has the same gender identity as cis women? Although her gender identity was part of the equation, it would be more accurate to say that she was discriminated against on the basis of her gender modality 11 . Gender modality, not gender identity, is what distinguishes trans women from cis women.
Gender modality can help researchers to describe participant experiences with improved accuracy by shaping how they phrase their study questions or frame the discussion section of their papers. For example, asking whether participants experienced discrimination because of their gender identity can cause confusion, which could be dispelled by asking whether they experienced discrimination because they are trans, detrans or another gender modality. Used thoughtfully, gender modality is a means of achieving improved clarity, accuracy and understanding. A researcher’s first question should always be: ‘What am I really trying to work out?’
Fluid and flexible language
Gender modality is not a panacea. Rather, it is one piece in the toolbox of those who engage in research involving human participants, whether in the medical, biological or social sciences. Its power lies in what people make of it. Our hope is that researchers and others will play with it, stretching it and exploring its full potential. Rather than foreclosing the evolution of language, gender modality welcomes it.
Not everyone is male or female. Not everyone is cis or trans. The sooner we make space for these truths, the better. And inviting scientists to adopt the concept of gender modality will hopefully foster research that better reflects the intricacies and nuances of our increasingly gender-expansive world.
The first step in science should never be to assume that something is correct. It should be to engage with the world in front of us — in all its magnificent complexity. Researching gender should begin with critically engaging with current language and concepts. Thoughtfulness, flexibility, curiosity and empathy are what science needs.
Nature 630 , 293-295 (2024)
doi: https://doi.org/10.1038/d41586-024-01719-9
Beischel, W. J., Schudson, Z. C., Hoskin, R. A. & van Anders, S. M. Psychol. Sex. Orientat. Gend. Divers. 10 , 355–372 (2023).
Article Google Scholar
Kidd, K. M. et al. Pediatrics 147 , e2020049823 (2021).
Article PubMed Google Scholar
Johns, M. M. et al. Morb. Mortal. Wkly Rep. 68 , 67–71 (2019).
Rioux, C. et al. J. Epidemiol. Commun. Health 76 , 764–768 (2022).
Hayes, L. et al. Am. J. Public Health 113 , 1153–1156 (2023).
Streed, C. G. Jr et al. Circulation 144 , e136–e148 (2021).
Adams, N. et al. Transgend. Health 2 , 165–175 (2017).
Marshall, Z., Kaposy, C., Brunger, F. & Welch, V. Bull. Appl. Transgend. Stud. 1 , 187–210 (2022).
Beauchamp, T. L. & Childress, J. F. Principles of Biomedical Ethics 8th edn (Oxford Univ. Press, 2019).
Google Scholar
Sedgwick, E. K. Epistemology of the Close t (Univ. California Press, 2008).
Katri, I. Univ . PA J. Law Soc. Change 20 , 51–79 (2017).
Download references
Competing Interests
The authors declare no competing interests.
Related Articles

Let’s talk about (biological) sex
- Public health

How Rwandan paediatrician Agnes Binagwaho fights racial stereotypes in global health
Career Q&A 02 JUL 24

Climate change is worsening the housing crisis — we must tackle the two together
World View 02 JUL 24

The science of protests: how to shape public opinion and swing votes
News Feature 26 JUN 24
Streamlined collaboration can boost CRISPR gene therapies for rare diseases
Correspondence 02 JUL 24

Combined COVID-flu vaccines are coming: Moderna jab clears major test
News 28 JUN 24

‘Vindicated’: Embattled misinformation researchers celebrate key US Supreme Court decision
News 26 JUN 24
Postdoctoral / Research Scientist / Research Assistant positions in Molecular Immunology
Postdoctoral / Research Scientist / Research Assistant positions in Molecular Immunology / Cancer Immunology
Dallas, Texas (US)
The University of Texas Southwestern Medical Center (UT Southwestern Medical Center)
Alzheimer's Disease (AD) Researcher/Associate Researcher
Xiaoliang Sunney XIE’s Group is recruiting researchers specializing in Alzheimer's disease (AD).
Beijing, China
Changping Laboratory
Osaka University Immunology Frontier Research Center Postdoctoral Researcher
IFReC, Osaka University in Japan offers Advanced Postdoc Positions for Immunology, Cell Biology, Bioinformatics and Bioimaging.
Suita Campus, Osaka University in Osaka, Japan
Immunology Frontier Research Center, Osaka University
PostDoc Researcher, Magnetic Recording Materials Group, National Institute for Materials Science
Starting date would be after January 2025, but it is negotiable.
Tsukuba, Japan (JP)
National Institute for Materials Science
Tenure-Track/Tenured Faculty Positions
Tenure-Track/Tenured Faculty Positions in the fields of energy and resources.
Suzhou, Jiangsu, China
School of Sustainable Energy and Resources at Nanjing University
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Help Us Stay Paywall-Free
Democracy depends on the free exchange of ideas. Help sustain it with a tax-deductible donation today.

Image: Ted Eytan
How Do Gender Transitions Happen?
It’s a much better question than the obsession with asking why .
Jules Joanne Gleeson
- June 4, 2021
This year has been a time of trial for trans people worldwide: in the United States, some improvements at the federal level in 2020 were then countered at the state level, with thirty-three state governments advancing over a hundred “model bills” denying trans people (and especially transgender children and youth) access to health care and supportive schooling environments. Last month in Germany and Spain , moves toward self-identification were defeated after cowardly abstentions from the local social democratic parties. In Britain similar efforts to reform the convoluted Gender Recognition Act were defeated in 2018, and this year transphobic feminists funded by the U.S. Christian right have lodged one lawsuit after another in an attempt to roll back trans rights. And in Hungary Viktor Orbán seized COVID-19 as an opportunity to effectively outlaw trans people from having any claim to their lived gender.
In this context, it’s urgent to not only respond to these setbacks and offensives against trans people, but offer our own understanding of what gender transition amounts to. Transgender liberation will not be a purely defensive process, but must build consciously on the existing breakthroughs achieved (often out of sight) by transgender movements. This essay approaches this by proposing that we counter unhelpful and harmful questions about gender transition by instead reframing these inquires as a question of how transitions become possible.
Doing so allows us to set aside both if and why questions of transition. Focusing on how transitions unfold is a concern distinct from what Julia Serano has termed the “etiological” fixation of writing on trans issues: the fascination around why it is certain people become transgender. (This speculation is one cis thinkers seem to be especially prone to.) On the ubiquitous why questions so often asked of trans people, Serano writes:
Eventually, I realized that it is a pointless question—the fact is that I am transsexual and I exist, and there is no legitimate reason why I should feel inferior to a cissexual [i.e., a nontranssexual] because of that. Once I accepted my own transsexuality, then it became obvious to me that the question ‘Why do transsexuals exist?’ is not a matter of pure curiosity, but rather an act of non-acceptance, as it invariably occurs in the absence of asking the reciprocal question: ‘Why do cissexuals exist?’ The unceasing search to uncover the cause of transsexuality is designed to keep transsexual gender identities in a perpetually questionable state, thereby ensuring that cissexual gender identities continue to be unquestionable.
This “etiological imperative” is often pushed onto trans writers, burdening us with an expectation that we account for why it is we deviated from the cisgender norm, preferably garnished with vivid childhood memories, and the all-important moment of dramatic revelation.
Another line of inquiry is whether transitions can be considered legitimate at all, with an increasingly vocal minority of Anglophone feminist philosophy attempting to undermine the case that trans people (and for various reasons, trans women in particular) ever have a valid claim to our gender. Trans lesbians in particular have faced the charge that their coupling of trans status and sapphic sexuality is harmful, “erasing” cisgender lesbians. Let us set aside these questions for something more interesting.
I take it as a given that transition between genders is, indeed, possible. But this does not mean that there is only one vision of how transition occurs. Referencing mostly the writings of other trans people, I will distinguish between two commonplace understandings of how transitions unfold. The first centers transitions as the consequence of trans people overcoming an array of hurdles on a personal level. The second centers the work of trans communities in the realization of our genders, and our quite particular pursuit of human flourishing.
These two conceptions are not rivals, nor strictly speaking opposing views. I suspect that most trans people have alternated between dependence on one or the other—perhaps daily, and certainly across the course of transition. Both have their uses for trans people, both as individuals and as a group, passing through the world. With that said, these views can be distinguished as follows.
In the first, transition constitutes purposefully varying “the encounter” between the individual and society’s gendered expectations. This view identifies “determining” qualities, which taken as a whole amount to an “overdetermination”: a certain number of “tells” might make one perceived as a woman, or a man, or as something unclearly in-between. Trans people struggle with mastering the way they in particular will be perceived, and mastery over this moment of encounter (the aleatory exchange) through exercises, affectations, and physical changes is the focus of transitioning.
The second view of transition focuses on trans communities and how they perform the central work of reciprocal recognition. This view frames identities as arising out of formative relationships and processes within those bonds. These loose collectives provide a context or space for the articulation of new language, lifestyle developments, and culture. This view foregrounds the circles that trans identities have tended to arise out of, and which offer support and resources, as only this kind of affinity-based grouping can.
View 1: Transition as mastery over the encounter
The first view of transition is an analytic one: it considers gender recognition to be a process that unfolds socially, and which trans people are tasked with doing their best to take command of using hormones, surgeries, training in posture or speech, their wardrobes, and formal changes to identity documents. It focuses on the evaluative moments trans people go through in considering themselves and preparing themselves, and in their encounters with the broader world.
To provide a simple example: nail polish alone might not do the job in getting a transitioning woman seen as she wishes to be, but nail polish together with long hair, a certain posture, five sessions of laser hair removal, and six months of hormone replacement therapy (HRT) might very well. Transition consists of amassing a medley of decisive features which inform the public at large of how you expect to be read.
This approach to transition is exemplified by the focus on “passing”: the ideal state for many trans people, and the focus of a considerable amount of energy, is passing through the world being mistaken for their cisgender target gender. The focus of those pursuing “passing” is both their own form (body, attire, voice, mannerism, word choice), but also interactions with an observer (assumed usually to be cis, and perhaps relatively uninformed on gender affairs). Perfecting this art requires not only a purely self-directed transformation, but a new orientation to the cis majority: would-be passers usually speak of the importance of “blending” (appearing among a group of cisgender people of one’s target gender, without any apparent mismatch). One ideal endpoint sought by some who pass is “deep stealth”: transgender people who’ve reached this lofty goal have only a select few friends, lovers, and physicians they have disclosed their transition to. (In most cases of adult transition this would, of course, require some form of radical relocation.)
Passing has been problematized many times by some critically minded trans people, who are prone to opposing it on political grounds as assimilationist: a transition calculated to cause no disruption to the prevailing cisgender order. Yet passing remains a commonplace concern both for those transitioning and for those considering it. For as long as the threat of violence remains suspended over those who are visibly transgender, passing (on an at least an everyday level) will remain a conscious priority for many.
Most recently, this perspective of transition-as-modified-encounter was expressed very clearly in a chain of tweets by Natalie Wynn, best known for her YouTube channel ContraPoints. Accounting for, and tacitly justifying, her desire for facial feminization surgery, Wynn introduces her transition in the following terms:
What I really want is not for people to call me a woman because they pity me, sympathize with me, or respect me. It’s better than them calling me a man, but only as a last resort. Really, I want them to call me a woman because it feels natural to do so, because I just seem like a woman to them. This is not something I can just demand, so a lot of the burden is on me. I have to change my appearance, my voice, my mannerisms not with the aim of becoming a woman in some metaphysical sense (a nonsensical idea) but of becoming a woman socially by appearing & interacting ‘like a woman’ with other people. But subjective isn’t the same as unpredictable. There is a lot of intersubjective agreement about what sorts of things make a person seem manly or womanly. And the point of transitioning is largely to present female to that collective perception.
In this view, transition appears as a reconciliatory move, a burden which for the most part lands on Wynn’s shoulders. Shifting not only how one is addressed by one’s friends and confidants, but also how one is intuitively understood by a passerby, postman, or ticket collector; the burden of transition is at once an intimate one and yet involves the entirety of society, as its “other” or onlooker: those undergoing transition must prepare themselves for encounters with strangers, through whatever changes are required to get them to “read” correctly. However, Wynn’s account is not altogether downbeat:
A year ago very few people thought of me as a woman. Now a majority of people probably do. My goal is to push that trend as far as I can, look back on my progress and one day say, ‘You know what? Good enough’. Hair, makeup, surgery, voice training, mannerisms—each of these is only a small part of a general effort to change how I’m perceived, how I’m treated by others, how I interact with others. It’s the net effect of these things—my acquired social position as a woman—that makes it philosophically sound to call me a woman. The minutiae of how I achieve that end are not particularly relevant. . . . The goal of my transition is merely to conform *enough* to elicit that mysterious ‘seems like a woman’ perception.
This view of transition as a gathering together of a medley of determining features can prove especially compelling to those still in the early stages of embarking on transition (or contemplating such a move, a process that can stretch out for years, or even decades).
While Wynn (as a self-described “Wittgenstein gal”) was doing her best to avoid taking a metaphysical stance in making this case, this account is highly reminiscent of the emphasis on “the encounter” developed throughout French philosopher Louis Althusser’s career. Later terming this position “aleatory materialism,” Althusser presented human interactions as drawing subjects into being through encounters, as they confronted institutions which demanded them to identify themselves. The “collective perception” described by Wynn follows this line in its rejection of any underlying truth: she wishes to be taken as a woman and (in her words) being read as such is the only philosophically sound basis for her being considered one.
Much the same approach to discerning womanhood appears in C. J. Hale’s classic response to Monique Wittig: “Are Lesbians Women?” Taking Wittig’s provocation (that lesbians are not) quite seriously, Hale draws from a rich selection of social science research to identify the features most probable to cause someone to be identified as a woman. In this form of account, being apprehended as a given gender is an apprehension triggered by a medley of cultural markers, each of which determine the evaluation given by those who encounter the person in question.
Gendered traits can cause a considerable degree of anxiety during the transition process (just as cisgendered men might worry that wearing too much pink attire makes them seem “unmanly,” or a cis woman could be concerned that a short haircut would leave her face appearing “mannish”). However, in most cases trans people will encounter immutable features they are unlikely to be able to do much to alter (the hip bones of trans men who transition post-puberty and the ribcages of trans women are two examples). Between these fixed and immutable features, much attention and energy can be expended on weighing up one’s prospects of encountering the outside world as one would desire. In a short film made by Wynn entitled “Gender Dysphoria” (since removed from public view), she conveys the tortured internal dialogue confronting many who are considering the process of transition, a process of self-examination that at its worst can leave trans people trapped in their homes for extended periods of time.
Taking up this outlook, many trans people have grown near obsessively astute in noticing, and itemizing, gendered features of everyday presentation. Few of society’s arbitrary sexed associations or gender expectations today escape the discerning eye of anxious transsexuals. The contents of many “how to” guides are intended to exactly instruct putative transitioners, with their more seasoned authors revealing the tricks and tips they have accumulated to achieve the desired outcome of passing through the world seamlessly.
This perspective is notable for matching very closely to the perspective of the state: for instance, to satisfy the British Passport Office that your gender change is permanent enough for a corrected “sex” entry, one currently needs the following: an assessment by a relevantly qualified medical professional, a letter from an employer or local authority confirming that your new identity is in use with them, and a completed deed poll. In certain U.S. states, further measures, such as taking out an advert in a local newspaper announcing the transitioner’s name change, are required. This reliance on a checklist demands that those wishing to update their official bureaucratic records approach transition as a series of successive tasks, at least at the level of paperwork. In many cases, compliance with this occurs on an obviously bad-faith basis: trans people passing through gender identity clinics often wear to their appointments more overtly gender-coded clothes than they would on a day-to-day basis, and provide an account of their daily lives and gender histories which they know to match the preferred model of “transsexuality,” in order to ensure access to hormones. Given the many indignities and second-guessing games required of trans people by the state, and medical profession, it seems inevitable that many adopt much the same view for surveying their basic lived experiences.
“Transition as preparations for an encounter with the world” is ultimately both most useful and least theoretically satisfying for its steadfast focus on the individual, and those around them. The greatest risk of this line of thinking is reducing transition to simply one process which takes place in an overall condition of atomism. Social influence only emerges analytically as a block or constraint on easy transition requiring individualized responses. Recognizing the much broader role social relations play requires a different theoretical approach. This brings us to another view of transition, one which centers the role trans communities play in cultivating the very transitioning subjectivity that this first perspective takes not as socially engendered, but as a given.
View 2: Transition as founded in community action
When turning to trans communities, I should first clarify that what I have in mind is not any one entity called “the transgender community.” The notion of a unified community is one mostly appealing to career politicians, who are fond of imagining they might be able to interact with an entire tier of potential voters by taking a single representative out for lunch. In reality, trans people are prized apart and mutually alienated in much the same way as any other group: differences in class, race, ethnicity, and gender position still ensure that even a pair of trans people in the same city might be unlikely on various grounds to ever meet. (With this said, the likelihood of prolonged unemployment, and dispossession from one’s family, make the life experiences of trans people significantly more likely to converge, and severe mental health problems are pervasive among trans people of whatever demographic station.)
Communities are never to be assumed as unified, or taken for granted. Trans communities, like any other kind, always have to be actively cultivated, and sustained, across time. Communities of this kind are the product of careful development in less-than-ideal circumstances by trans people, and can never be treated as a given. For the commonality between trans people to become a true affinity, a more profound engagement is required, and in most cases these groups will consist of those with both trans status and other significant social commonalities (with an exception for clearly structured online communities such as /r/AskTransgender, which as its name suggests is intended exclusively for Q&A threads).
As such there is not, has never been, and could never be one trans community, and it’s better to think in terms of trans circles. These groupings might be founded around support groups, book clubs, club nights, youth centers, web forums, social media constellations, WhatsApp group chats, shared apartments, and community potlucks. These trans circles have become easier to establish across time, both because of mass access to advances in communication technology and a certain self-perpetuating cycle of access to potential mentors.
These circles are often not strictly exclusive to trans people: many cis people also find themselves developing an affinity with trans circles, and boundaries can often become porous in queer scenes. Such groupings of affinity can arise spontaneously, or they can be the product of purposeful development, also known as community organizing. Sometimes sites for the celebration and mutual development of trans identities can arise in unlikely places. Even otherwise hostile online outlets such as 4chan can foster distinctive nonbinary identities.
Considering transition in these terms presents a rather different view to splitting that process into gendered determinations. Whereas the focus on the “encounter” trans people must master in order to move through the world can tell us much, it’s not only interactions with strangers that form the core of self-realization for many undergoing transition. Trans people most often draw strength from interacting with other like-minded souls (often, but not exclusively, trans themselves) who are able to offer them the specific support, mentoring, and reciprocal recognition that identity formation requires.
Beyond the personal level (what trans circles offer the individuals who make them up), there is also a collective progression brought about by the shared pool of expertise and experience built up by lasting bonds between those developing a shared approach to life and developing ties of affinity. On the level of community, trans people are collectively able to build up a considerable base of shared knowledge. This is especially urgent in a context in which much of the medical profession remains wedded to pathologizing conceptualizations of trans people, and often deploys outmoded medical practices.
One indispensable service offered by trans communities to newcomers is presenting them with the fact that much of what they had considered their most freakish features are, within trans circles, so familiar as to be articles of cliché.
An example of this practical wisdom in action can be found in Imogen Binnie’s first novel, Nevada (2013). Here the protagonist, Maria, several years into her transition and soon after encountering another trans character deeply in denial, has her approach to online trans activism recounted:
There’s a thing Maria is used to doing on the internet. It came from the older practice of telling everybody who thought they might be trans that they must be absolutely certain that they were trans before they even considered buying some clothes or starting a testosterone blocker. . . . Trans women on the internet looked around and were like, well, maybe surviving for the first part of your life in the role of a cis dude is an adaptive strategy. . . . For a while they were like, ‘You must be entirely certain’. Then they were like, ‘I dunno man, it sounds like you’re probably trans, you should explore that’. Then, eventually, when Maria and the trans women of the internet couldn’t help but notice that they were 100% accurate in their message board diagnoses, they started just saying, ‘Welp, you are definitely trans’. Because even on the off chance that somebody finding a trans community to talk to about these things was not, actually, trans . . . maybe hearing somebody say, like, ‘You are trans’, would spur some useful thinking. Like, if you’re going to decide on your gender for the rest of your life based on what a couple of idiots on the internet tell you, you probably have problems beyond a false diagnosis of transsexuality.
It’s notable here that the group reaching these conclusions is “Maria and the trans women of the internet,” a collective described here as having moved through both a stage of theorization and experimentation before concluding with a best practice of encouraging potential transitioners with affirmation. Through their shared experiences and observations, those who had already embarked upon transition established a bridge between their own conditions and the conditions of those still weighing up the prospect of committing to changing their gender.
What this passage reveals is the rather pragmatic character expectations and theorizations we can expect from communities of affinity. Needless to say, the maxim, “If you’re asking whether or not you’re trans . . . you’re trans!” is a gender normative statement of its own kind. However, the relevant capacity for coercion is entirely missing: as Binnie wryly implies, “trans women on the internet” are unlikely to wield the power available to doctors at Johns Hopkins, and anyone susceptible to their advice was likely encountering uncertainty around their gender for sound reasons.
Prior to writing this novel, Binnie had spent years as a leading trans activist, with her protagonist clearly informed by her own experiences as a politically engaged New Yorker (the novel is obviously and unabashedly self-satirizing throughout). In other words, Nevada ’s success was based on many years, and innumerable conversations, distilling experiences of transgender life into a single narrative account.
In addition to the mentoring and enculturation of younger trans people by old hands, there are also direct and ongoing ways in which trans (or trans celebratory queer) circles enrich and fulfill the lives of those involved.
Communities of people with a sense of affinity for each other are able to build up their own language for describing experiences and bodies. This can ultimately allow for a thoroughgoing rewriting of terms which trans people apply to their own physical forms. Another piece by C. J. Hale focuses on the variations in sexuality, gender, and embodiment allowed for in the kink practices that were integral to pre-2000s Leatherdyke communities (many of whose participants have since transitioned to men). These predecessors of today’s queer and trans scenes provided frameworks for shifting gendered embodiment, in a way that today’s trans communities offer on a more conceptual level. In “Leatherboys and their Daddies: How to Have Sex Without Women or Men” (1997), Hale writes:
Leatherdyke genderplay enables a phenomenon sometimes called ‘retooling’ or ‘recoding’ our bodies in trans community discourse. Sexual interactions, along with public restrooms and medical settings, are some of the sites at which dominant cultural connections between genitals and gender are the tightest, so many transpeople must remap the sexualized zones of our bodies if we are to be sexually active. . . . One such phenomenon is that inanimate objects—dildoes—sometimes take on some of the phenomenological characteristics of erogenous body parts. . . . Sometimes leatherdykes resignify sexed bodily zones. Among some leatherdyke faggots, an important desideratum is to keep masculinity as seamless as possible during scenes, and gay leathermen’s masculinities often provide the paradigms of masculinity here. Thus, if the body part a leatherdyke daddy is fisting is that which a physician would unequivocally deem a ‘vagina’, it may be resignified so that its use for erotic pleasure is consistent with male masculinity. It may become a ‘hole’, ‘fuckhole’, ‘manhole’, ‘boyhole’, ‘asshole’, or ‘butthole’, and a leatherdyke boy pleading, ‘Please, Daddy, fuck my butt!’ may be asking daddy to fuck the same orifice into which a physician would insert a speculum to perform a pap smear. Of course, this resignification may prove painful if this boy’s daddy does not understand it.
While these practices were not exclusively explored by those who were later to transition, Hale makes clear that, for many involved, they provided a means of breaching the normative associations with their physical forms which had previously stifled them.
This twenty-one-year-old account of directly transformative practices, native to a particular community with its own understandings for terms suitable for those immersed in it, still speaks to the sexual practices developed by trans people today. A poem by Gabe Moses entitled “How to Make Love to a Trans Person” (2012) relates much the same process of semantic rearticulation and conceptual reimagining:
Forget the images you’ve learned to attach To words like cock and clit, Chest and breasts. Break those words open Like a paramedic cracking ribs To pump blood through a failing heart [. . .] Get rid of the old words altogether. Make up new words. Call it a click or a ditto. Call it the sound he makes When you brush your hand against it through his jeans, When you can hear his heart knocking on the back of his teeth
These pieces of writing record the processes of transformation collectively enabled by the communities of affinity which have enabled and celebrated transition. This would seem to point in quite a different direction to the process of identification and elimination of stray misleading features presented in the first view of transition. Whereas much of the attention of trans people, especially early into transition, is drawn toward the “moment of encounter,” the subjectivity robust enough to weather such a storm is provided in large part by this “underground” body of community-built resources.
The prominent role played by communities in substantiating transitions can be understood in a few ways. Julia Serano’s view of transition constituting an “intrinsic inclination” on the part of trans people would suggest that these communities serve as an underground means to achieve the expression that certain cultures have more institutionally established outlets for. By contrast, Susan Stryker’s account of identity realization in Transgender History (2008) is considerably more complex and historicist. Stryker traces how new identities arose in particular contexts, both informed by the perceptions of cisgendered physicians and challenging them at every turn.
The two views outlined above are not directly at odds, and can be thought of as two differing registers for understanding the process of transition. Neither can account fully for transition as it exists today: there are those who eschew community as far as possible, treating their transition as a solitary affair (although it seems unlikely that many would not rely at least to some extent on information gleaned from the autonomously stockpiled resources by trans communities). And there are those who report limited concern with the need to eliminate undesirable features, or affirm themselves through encounters with strangers.
But can either of these views—individual wriggling in the face of interpellation or community working up their own normative bedrock—ever be fully accepted?
While they have been my primary interest, my intention here has not been to laud the workings of communities. Organization between ourselves as peers has achieved breakthrough after breakthrough in the pre-political labors required for forming and sustaining ourselves. But keeping one another alive cannot be collapsed with revolutionary change. We have made the best of our proletarianized existence, but we have yet to escape it.
For as long as trans people operate in the face of a capitalist state, we will break in two directions: atomized struggle and the fashioning of a trans-specific mode of civil society. Trans people oscillate not only out of their atomized state but often enough back into it: many of our worst traumas are inflicted by other trans people, and many drop out of activism with an embittered set of scare quotes placed around the words “trans community.” Every petty corruption, frustrationm and normativity-enforcing eccentricity finds itself empowered by the raw necessity of communal work to avoid trans life becoming heteronymous to the whims and outdated protocols of state provision. In other words, to exist on our own terms immediately follows through into ferocious rows about exactly who “we” are.
The result is that trans communities are despised and relied upon by trans people in equal measure, and for the exact same reason. These ever-imperfect and ad hoc circles of shared interest are the best (and worst) stopgap against the total immiseration provided by the existing capitalist division of labor.
Surpassing this divide requires a new movement, which we so far have only the haziest picture of: an anti-capitalist struggle fully responsive to, and in part growing out of, the existing struggles waged to secure our basic subsistence.
Editor’s Note : This essay is an excerpt from Transgender Marxism edited by Jules Joanne Gleeson and Elle O’Rourke, available from Pluto Press.
Jules Joanne Gleeson is a writer, comedian, and historian. She is coeditor, with Elle O’Rourke, of Transgender Marxism . She has published essays in outlets including Viewpoint Magazine , Invert Journal , and VICE , and performed internationally at a wide range of communist and queer cultural events.
Boston Review is nonprofit and reader funded.
We rely on readers to keep our pages free and open to all. Help sustain a public space for collective reasoning and imagination: become a supporting reader today .
Readers Also Liked

Eroding the Regulatory State

The Death of the Gay Bar
Donate to support work like this:, sign up for our newsletter.
The best writing on ideas, politics, and culture delivered straight to your inbox.
Most Recent

For a Solidarity State
The state structures society. It can make us more prone to care for one another.

Inside Project 2025
Backed by the Heritage Foundation, the initiative seeks to undermine longstanding safeguards against abuses of executive power.

Black Planet
“There is no plot; it’s just Black people living their lives with other Black people on their own planet.”
A political and literary forum, independent and nonprofit since 1975.
Registered 501(c)(3) organization.
Get a FREE copy of Reclaiming Freedom !

Get a free copy of this recent issue—featuring Aziz Rana, Lea Ypi, Adom Getachew, and many others—when you become a member at any level.
Just enter code FREEDOM at checkout.
A special offer for July 4

Get a free copy of this recent issue—featuring Aziz Rana, Lea Ypi, Adom Getachew & others—when you become a member at any level.
Transgender Identity and the Path to Self-Acceptance
Walter Bockting , a clinical psychologist and the founding director of the Gender and Sexuality Program at Columbia University Irving Medical Center (CUIMC), explains why more young people are identifying as transgender and discusses issues surrounding care.
Tell us about the Gender and Sexuality Program. What is its mission? Who does it serve?
We launched our program in 2018 to serve people identifying as transgender or nonbinary. It now offers comprehensive mental-health services to those who are questioning their gender or sexuality or struggling to navigate life with an identity that does not conform to traditional expectations. The majority of our patients are adolescents and teenagers, some of whom are considering medical treatments to align their bodies with their gender identity. We also see adults who are considering making such changes. And sometimes parents will come in with young children who appear to identify with another gender. They want to understand what their children are going through and how best to support them.
What exactly do the terms “transgender” and “nonbinary” mean?
Transgender is an umbrella term used to describe anyone with a gender identity that differs significantly from the sex they were assigned on their birth certificate, based on their outward anatomy. This can include people whose gender is the opposite of the sex they were assigned at birth — that is, a person assigned male at birth who identifies as a girl or woman or a person assigned female at birth who identifies as a boy or man. Transgender people may undergo medical interventions to align their appearance with their gender identity, or they may choose not to do so. Nonbinary individuals, who identify as neither boy nor girl, man nor woman, are generally considered part of the transgender community too. Their identities may combine aspects of masculinity or femininity or transcend these binary categories. Research conducted by my group and others has shown that gender identity and expression exist on a spectrum. For many people they are composed of different characteristics not easily reducible to being either male or female, masculine or feminine.
Is the transgender population growing?
There’s been a significant increase in people who openly identify as transgender or nonbinary over the past decade, especially among young people. Surveys indicate that 2 to 3 percent of adolescents and teenagers and about 5 percent of young adults in the United States now identify as transgender, with half or more of these individuals considering themselves nonbinary. Among older adults, that number is less than 1 percent, which is in line with historical trends dating back to the mid-twentieth century, when the concept of gender identity as distinct from biological sex first emerged.
What explains the rise?
Of course, there are cultural forces at work. As more and more people have embraced diverse gender identities, less stigma is associated with being trans. Which isn’t to say that it’s particularly easy to come out as transgender, because gender-nonconforming people are still among the most stigmatized in society. But transgender people feel freer to be themselves now, compared to previous decades. This is especially true for young people who’ve grown up seeing transgender individuals depicted positively in the media and meeting other transgender folks in school, on the job, or through friends and family. I think that older adults who grew up when it was less socially acceptable to be transgender are more likely to have suppressed or concealed any gender-identity issues they had, which is why you see a generational divide in these statistics.
How many Americans now undergo gender-affirming surgeries?
It’s difficult to say for sure, because the US has no centralized system for collecting data on such procedures, but it’s probably on the order of ten thousand people a year, the vast majority of whom are adults. Only a few hundred adolescents undergo gender-affirming surgeries annually, although thousands of young people do receive puberty suppressants or hormones to feminize or masculinize their bodies.
Before they perform gender-affirming surgery, physicians typically require a referral from a mental-health professional who can attest that a patient has thought the decision through, and in the past obtaining such a referral was more challenging than it is today. For example, until the mid-1990s, people who sought genital surgery were often turned down if they exhibited symptoms of severe anxiety or depression, which were seen as signs of mental instability. Now we know that feeling an incongruence between one’s gender identity and sex assigned at birth can contribute to mood disorders and that it is often appropriate to provide a person gender-affirming care at the same time that you’re treating them for other mental-health conditions.
People who opt for gender-affirming surgeries typically carry a diagnosis of gender dysphoria, a condition characterized by a discomfort with one’s sex assigned at birth that is so intense that it becomes debilitating, making daily life difficult if not impossible. Many, but not all, teenagers and young adults who now identify as transgender experience gender dysphoria. And having gender dysphoria does not necessarily lead a person to seek puberty suppression, hormone therapy, surgery, or any other gender-affirming medical interventions. Gender dysphoria plays out differently for each person.
Do your patients at the Gender and Sexuality Program tend to have dysphoria?
Most of them do, yes. We see people who are in a lot of emotional pain. In addition to experiencing incongruence between their gender identity and physical sex characteristics, which is incredibly frustrating, many are also socially isolated. Before coming to us, some have never spoken to anybody at length about what they’re going through. They might also have experienced bullying, harassment, violence, and discrimination. And it’s not uncommon for them to have internalized other people’s negative attitudes about transgender people and to feel ashamed of who they are. The cumulative stress can contribute to a wide range of mental-health issues, including substance abuse, suicidal thoughts, self-harm, anxiety, and mood disorders. When we help them come up with a plan to alleviate their gender dysphoria, we often need to address these issues, too.

What does treatment typically look like?
It starts with talk therapy to facilitate self-acceptance and identity exploration. We ask patients to describe how they’d ideally like to express their gender and what, if anything, is holding them back. If they haven’t lived openly as a transgender person yet, we might suggest that they first learn about the possibilities online and then try expressing their gender identity in a safe, private setting, like in the company of supportive friends or family members. After exploring their identity and expression in this way, some people may decide that they don’t need to change their gender identity in a formal sense. They might conclude that they’re simply uncomfortable with traditional gender norms and can be happy continuing to identify as a man or woman if they bend the rules to their liking a bit. But more often than not, among the patients we see, such experiences are affirming, encouraging people to move forward and continue transitioning. Then we might help them develop a plan for coming out at school or work, which can include preparing to address changes in pronoun use, how they dress, and bathroom access. We’ll work with their families to ensure that individuals get the emotional and social support they need. And if a patient is determined to change their body, we’ll help them think through the available options. We’ll also support them after they’ve made any physical changes, because the challenges of being transgender don’t end at that point.
You’ve been counseling transgender people and studying their lives for more than three decades. In particular, you’ve researched how their identities evolve over time. What have you learned?
One insight is that most transgender people, as they get older, become less interested in trying to pass as cisgender men and women and more comfortable identifying primarily as trans men, trans women, or nonbinary individuals. It can take them years to get to this point, because many transgender people, especially when they’re young, have internalized our society’s binary conception of gender and feel compelled to adopt the stereotypical gender expressions of men or women. They may initially think, “Well, I know I’m not a girl, so I must be a boy. Now I need to look and behave exactly like one!” This isn’t surprising. It’s human nature to seek a sense of belonging by carving out rather neatly defined identities for ourselves. And realizing that your gender identity is different or ambiguous can be nerve-racking. When my colleagues and I counsel transgender people, we encourage them to unearth and face some of this anxiety. We’ve found that by accepting the complexity and uniqueness of their gender identities, and by embracing the fact that, as transgender people, their experiences will always be unique and a bit different from cisgender people’s, they’re able to feel better about themselves and ultimately find more meaning in their lives.
Shortly before coming to Columbia in 2012, you served as president of the World Professional Association for Transgender Health (WPATH). In that role, you oversaw the creation of treatment guidelines that have made it easier for nonbinary people in many countries to access appropriate gender-affirming medical care.
Yes, these guidelines, which are now followed by most medical professionals and endorsed by their associations, stipulate that people who identify as nonbinary should have access to the same high-quality care as other transgender people. This is important because, as recently as the early 2000s, people who needed to change their bodies but didn’t necessarily want to look like cisgender men or women were often turned away. Maybe they just wanted to alter their chest, tone of voice, or hair-growth patterns while forgoing other procedures. If a physician asked if they identified as a man or woman and they responded, “Neither,” they might have been told, “Well, come back when you figure it out.” Now they’re treated equally and can access gender-affirming medical interventions appropriate to their identities and needs.
You’re also credited with improving access to care for transgender people who identify as gay, lesbian, or bisexual.
Yes, when I entered this field, another common requirement for getting gender-affirming surgery was to identify as heterosexual after transitioning. Can you believe that? In other words, you couldn’t be sexually attracted to members of your own gender identity but rather only to members of the sex you were originally assigned at birth. This was rooted in a twentieth-century theory called the “inversion hypothesis,” which held that the desire to transition one’s gender was the manifestation of intense same-sex attraction — basically, an extreme form of homosexuality. So, for example, a person who was assigned male at birth and sexually attracted to other men — and who had an unusually “de-masculinized and feminized” mind — might eventually want to become a woman. Transgender people who were brave enough to disclose their same-gender attractions faced significant barriers to accessing gender-affirming medical care. And transgender men who were attracted to men weren’t even thought to exist. But in the late 1980s and early 1990s, I published a series of papers documenting that transgender men who are attracted to men do exist and are quite happy and well-adjusted. This research, together with other scholars’ observations that transgender women often identify as lesbian, helped usher in a paradigm shift, where gender identity and sexual orientation were finally understood as separate components of one’s overall identity.
Today there is fierce debate about whether it has become too easy for adolescents to access gender-affirming medical care. In the past couple of years, more than twenty states have passed laws banning anyone under the age of eighteen from receiving puberty suppressants, hormone therapies, and surgeries. What do you make of this?
I’m shocked at how thoroughly the public discussion on this issue has become politicized and inundated by misinformation. Opponents of transgender rights, who’ve now organized themselves into a powerful movement, would have Americans believe that their kids are being brainwashed into thinking they’re transgender and greenlighted for medical procedures that they don’t need and will later regret. Of course, this isn’t true. Even among youth with gender dysphoria, only those with the most pronounced symptoms access medical interventions, usually after extensive counseling and therapy. What’s really happening is that young people in nearly half the United States are being denied access to health care that they desperately need, care that nearly every major medical organization in the country has deemed safe and essential. It’s a disgrace. Honestly, it makes me so upset that it’s difficult for me to talk about it.
“I’m shocked at how thoroughly the public discussion on this issue has become politicized and inundated by misinformation.”
When you meet a young person with gender dysphoria and hear them describe what they’re going through, you don’t forget it. It’s heartbreaking. I’m talking about kids who are overwhelmed by despair related to their sex characteristics. Who take showers in the dark to avoid seeing their bodies. Who can’t focus in school because they’re so upset about going through puberty. To these kids and their families, having access to gender-affirming care can feel like a matter of life or death.
Puberty blockers are now given to transgender kids as young as ten or eleven, which critics point out is a pretty tender age to be making medical decisions whose effects could last a lifetime.
Helping kids to change their bodies raises serious questions and concerns, there’s no doubt about it. I think that everyone working in the field of transgender health right now is asking themselves: Will any of these kids come to regret this decision? Will the puberty blockers cause any unintended effects later in life? Exactly how much therapy should these kids be getting before they transition? We don’t have conclusive answers to these questions yet. The best data available comes from a clinic in Amsterdam where gender-affirming medical care was first provided to adolescents in the 1990s. I grew up and trained in the Netherlands, and I’ve conducted research with some of the people who developed that program, which has shaped my thinking. In any case, the results from patients of that clinic are so far positive, which is why health-care providers throughout Europe and the US have since started offering puberty suppression and hormone therapies to adolescents. Hundreds of Dutch people who received gender-affirming care as youngsters decades ago are still being followed by researchers. Very few say they regret transitioning or show signs of serious unintended effects. And as a group, they have lower rates of anxiety and depression than other transgender people who attain access to gender-affirming care later in life or not at all.
What are you studying now?
For the past eight years, I’ve been leading a longitudinal study following the lives of more than three hundred transgender people, who now range in age from about twenty to ninety, in New York City, San Francisco, and Atlanta. My colleagues and I are hoping to follow these participants for years to come. We want to learn what aspects of their lives are most challenging, what brings them happiness and contentment, and how they develop resilience in the face of stigma, discrimination, and the associated stress. Among our discoveries so far is that transgender people who maintain close friendships with other transgender people are happier and healthier overall, as are those who are in regular contact with their parents, siblings, or other close family members and friends.
The importance of family, I think, is particularly interesting. Other studies have shown that transgender people are often rejected by their families or subjected to such awful abuse at home that they have to cut ties. Some of our participants have experienced this too. But many others told us things like, “You know, my folks weren’t very nice to me at first and actually said some terrible things. But I was patient and left the door open, and eventually they came around and accepted me. And I’m glad I gave them a chance, for my own sake and theirs.”
That’s inspiring. Do you share those types of stories with your patients?
I do. I’m always telling my patients about the dignity, strength, and courage of other transgender people. I’ll recommend movies, TV shows, and books, and I’ll tell them anecdotes about some of the amazing patients and research participants I’ve known over the years. When they’re ready, I’ll help them connect meaningfully with other transgender people in group therapy and support meetings. And I’ll tell them, “I know that being transgender isn’t easy — but it’s also exciting, beautiful, and, yes, fabulous. And you are now among these fabulous people who, just by being themselves and holding their heads up high, are changing the world.”
This article appears in the Winter 2023-23 print edition of Columbia Magazine with the title "Beyond the Binary."
More From Health & Medicine

A Physician’s Journey into the Minds of Coma Patients
In studying people with severe brain injuries, Columbia neurologist Jan Claassen hopes to better identify those likely to regain consciousness

Legendary Child Psychiatrist Clarice Kestenbaum Looks Back — and Forward
At 95, the Columbia professor emerita of clinical psychiatry reflects on an ever-developing field

How Much Plastic Is in Bottled Water? You Probably Don’t Want to Know
Columbia researchers find sobering evidence that bottled water contains far more microplastic particles than previously estimated
Stay Connected.
Sign up for our newsletter.
General Data Protection Regulation
Columbia University Privacy Notice
Understanding transgender people, gender identity and gender expression

According to the APA Style guide, the term “transsexual” is largely outdated, but some people identify with it; this term should be used only for an individual who specifically claims it. While the term “transsexual” appears multiple times throughout this document, APA’s Committee on Sexual Orientation and Gender Diversity is undertaking a systematic review of its use along with other terms. In the meantime, please refer to the Guidelines for Psychological Practice with Transgender and Gender Nonconforming People (PDF, 472KB) for more up-to-date language regarding transgender and gender nonconforming people.
Transgender is an umbrella term for persons whose gender identity, gender expression or behavior does not conform to that typically associated with the sex to which they were assigned at birth. Gender identity refers to a person’s internal sense of being male, female or something else; gender expression refers to the way a person communicates gender identity to others through behavior, clothing, hairstyles, voice or body characteristics. “Trans” is sometimes used as shorthand for “transgender.” While transgender is generally a good term to use, not everyone whose appearance or behavior is gender-nonconforming will identify as a transgender person. The ways that transgender people are talked about in popular culture, academia and science are constantly changing, particularly as individuals’ awareness, knowledge and openness about transgender people and their experiences grow.
What is the difference between sex and gender?
Sex is assigned at birth, refers to one’s biological status as either male or female, and is associated primarily with physical attributes such as chromosomes, hormone prevalence, and external and internal anatomy. Gender refers to the socially constructed roles, behaviors, activities, and attributes that a given society considers appropriate for boys and men or girls and women. These influence the ways that people act, interact, and feel about themselves. While aspects of biological sex are similar across different cultures, aspects of gender may differ.
Various conditions that lead to atypical development of physical sex characteristics are collectively referred to as intersex conditions.
Have transgender people always existed?
Transgender persons have been documented in many indigenous, Western, and Eastern cultures and societies from antiquity until the present day. However, the meaning of gender nonconformity may vary from culture to culture.
What are some categories or types of transgender people?
Many identities fall under the transgender umbrella. The term transsexual refers to people whose gender identity is different from their assigned sex. Often, transsexual people alter or wish to alter their bodies through hormones, surgery, and other means to make their bodies as congruent as possible with their gender identities. This process of transition through medical intervention is often referred to as sex or gender reassignment, but more recently is also referred to as gender affirmation. People who were assigned female, but identify and live as male and alter or wish to alter their bodies through medical intervention to more closely resemble their gender identity are known as transsexual men or transmen (also known as female-to-male or FTM). Conversely, people who were assigned male, but identify and live as female and alter or wish to alter their bodies through medical intervention to more closely resemble their gender identity are known as transsexual women or transwomen (also known as male-to-female or MTF). Some individuals who transition from one gender to another prefer to be referred to as a man or a woman, rather than as transgender.
People who cross-dress wear clothing that is traditionally or stereotypically worn by another gender in their culture. They vary in how completely they cross-dress, from one article of clothing to fully cross-dressing. Those who cross-dress are usually comfortable with their assigned sex and do not wish to change it. Cross-dressing is a form of gender expression and is not necessarily tied to erotic activity. Cross-dressing is not indicative of sexual orientation. (See Answers to Your Questions: For a Better Understanding of Sexual Orientation and Homosexuality for more information on sexual orientation.) The degree of societal acceptance for cross-dressing varies for males and females. In some cultures, one gender may be given more latitude than another for wearing clothing associated with a different gender.
The term drag queens generally refers to men who dress as women for the purpose of entertaining others at bars, clubs, or other events. The term drag kings refers to women who dress as men for the purpose of entertaining others at bars, clubs, or other events.
Genderqueer is a term that some people use who identify their gender as falling outside the binary constructs of “male” and “female.” They may define their gender as falling somewhere on a continuum between male and female, or they may define it as wholly different from these terms. They may also request that pronouns be used to refer to them that are neither masculine nor feminine, such as “zie” instead of “he” or “she,” or “hir” instead of “his” or “her.” Some genderqueer people do not identify as transgender.
Other categories of transgender people include androgynous , multigendered , gender nonconforming , third gender , and two-spirit people . Exact definitions of these terms vary from person to person and may change over time, but often include a sense of blending or alternating genders. Some people who use these terms to describe themselves see traditional, binary concepts of gender as restrictive.
Why are some people transgender?
There is no single explanation for why some people are transgender. The diversity of transgender expression and experiences argues against any simple or unitary explanation. Many experts believe that biological factors such as genetic influences and prenatal hormone levels, early experiences, and experiences later in adolescence or adulthood may all contribute to the development of transgender identities.
How prevalent are transgender people?
It is difficult to accurately estimate the number of transgender people, mostly because there are no population studies that accurately and completely account for the range of gender identity and gender expression.
What is the relationship between gender identity and sexual orientation?
Gender identity and sexual orientation are not the same. Sexual orientation refers to an individual’s enduring physical, romantic, and/or emotional attraction to another person, whereas gender identity refers to one’s internal sense of being male, female, or something else. Transgender people may be straight, lesbian, gay, bisexual, or asexual, just as nontransgender people can be. Some recent research has shown that a change or a new exploration period in partner attraction may occur during the process of transition. However, transgender people usually remain as attached to loved ones after transition as they were before transition. Transgender people usually label their sexual orientation using their gender as a reference. For example, a transgender woman, or a person who is assigned male at birth and transitions to female, who is attracted to other women would be identified as a lesbian or gay woman. Likewise, a transgender man, or a person who is assigned female at birth and transitions to male, who is attracted to other men would be identified as a gay man.
How does someone know that they are transgender?
Transgender people experience their transgender identity in a variety of ways and may become aware of their transgender identity at any age. Some can trace their transgender identities and feelings back to their earliest memories. They may have vague feelings of “not fitting in” with people of their assigned sex or specific wishes to be something other than their assigned sex. Others become aware of their transgender identities or begin to explore and experience gender-nonconforming attitudes and behaviors during adolescence or much later in life. Some embrace their transgender feelings, while others struggle with feelings of shame or confusion. Those who transition later in life may have struggled to fit in adequately as their assigned sex only to later face dissatisfaction with their lives. Some transgender people, transsexuals in particular, experience intense dissatisfaction with their sex assigned at birth, physical sex characteristics, or the gender role associated with that sex. These individuals often seek gender-affirming treatments.
What should parents do if their child appears to be transgender or gender nonconforming?
Parents may be concerned about a child who appears to be gender-nonconforming for a variety of reasons. Some children express a great deal of distress about their assigned sex at birth or the gender roles they are expected to follow. Some children experience difficult social interactions with peers and adults because of their gender expression. Parents may become concerned when what they believed to be a “phase” does not pass. Parents of gender-nonconforming children may need to work with schools and other institutions to address their children’s particular needs and ensure their children’s safety. It is helpful to consult with mental health and medical professionals familiar with gender issues in children to decide how to best address these concerns. It is not helpful to force the child to act in a more gender-conforming way. Peer support from other parents of gender-nonconforming children may also be helpful.
How do transgender individuals make a gender transition?
Transitioning from one gender to another is a complex process and may involve transition to a gender that is neither traditionally male nor female. People who transition often start by expressing their preferred gender in situations where they feel safe. They typically work up to living full time as members of their preferred gender by making many changes a little at a time. While there is no “right” way to transition genders, there are some common social changes transgender people experience that may involve one or more of the following: adopting the appearance of the desired sex through changes in clothing and grooming, adopting a new name, changing sex designation on identity documents (if possible), using hormone therapy treatment, and/or undergoing medical procedures that modify their body to conform with their gender identity.
Every transgender person’s process or transition differs. Because of this, many factors may determine how the individual wishes to live and express their gender identity. Finding a qualified mental health professional who is experienced in providing affirmative care for transgender people is an important first step. A qualified professional can provide guidance and referrals to other helping professionals. Connecting with other transgender people through peer support groups and transgender community organizations is also helpful.
The World Professional Association for Transgender Health (WPATH), a professional organization devoted to the treatment of transgender people, publishes The Standards of Care for Gender Identity Disorders , which offers recommendations for the provision of gender affirmation procedures and services.
Is being transgender a mental disorder?
A psychological state is considered a mental disorder only if it causes significant distress or disability. Many transgender people do not experience their gender as distressing or disabling, which implies that identifying as transgender does not constitute a mental disorder. For these individuals, the significant problem is finding affordable resources, such as counseling, hormone therapy, medical procedures and the social support necessary to freely express their gender identity and minimize discrimination. Many other obstacles may lead to distress, including a lack of acceptance within society, direct or indirect experiences with discrimination, or assault. These experiences may lead many transgender people to suffer with anxiety , depression or related disorders at higher rates than nontransgender persons.
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), people who experience intense, persistent gender incongruence can be given the diagnosis of "gender dysphoria." Some contend that the diagnosis inappropriately pathologizes gender noncongruence and should be eliminated. Others argue that it is essential to retain the diagnosis to ensure access to care. The International Classification of Diseases (ICD) is under revision and there may be changes to its current classification of intense persistent gender incongruence as "gender identity disorder."
What kinds of discrimination do transgender people face?
Anti-discrimination laws in most U.S. cities and states do not protect transgender people from discrimination based on gender identity or gender expression. Consequently, transgender people in most cities and states face discrimination in nearly every aspect of their lives. The National Center for Transgender Equality and the National Gay and Lesbian Task Force released a report in 2011 entitled Injustice at Every Turn , which confirmed the pervasive and severe discrimination faced by transgender people. Out of a sample of nearly 6,500 transgender people, the report found that transgender people experience high levels of discrimination in employment, housing, health care, education, legal systems, and even in their families.
Transgender people may also have additional identities that may affect the types of discrimination they experience. Groups with such additional identities include transgender people of racial, ethnic, or religious minority backgrounds; transgender people of lower socioeconomic statuses ; transgender people with disabilities ; transgender youth; transgender elderly; and others. Experiencing discrimination may cause significant amounts of psychological stress, often leaving transgender individuals to wonder whether they were discriminated against because of their gender identity or gender expression, another sociocultural identity, or some combination of all of these.
According to the study, while discrimination is pervasive for the majority of transgender people, the intersection of anti-transgender bias and persistent, structural racism is especially severe. People of color in general fare worse than White transgender people, with African American transgender individuals faring far worse than all other transgender populations examined.
Many transgender people are the targets of hate crimes . They are also the victims of subtle discrimination—which includes everything from glances or glares of disapproval or discomfort to invasive questions about their body parts.
How can I be supportive of transgender family members, friends, or significant others?
Educate yourself about transgender issues by reading books, attending conferences, and consulting with transgender experts. Be aware of your attitudes concerning people with gender-nonconforming appearance or behavior.
Know that transgender people have membership in various sociocultural identity groups (e.g., race, social class, religion, age, disability, etc.) and there is not one universal way to look or be transgender.
Use names and pronouns that are appropriate to the person’s gender presentation and identity; if in doubt, ask.
Don’t make assumptions about transgender people’s sexual orientation, desire for hormonal or medical treatment, or other aspects of their identity or transition plans. If you have a reason to know (e.g., you are a physician conducting a necessary physical exam or you are a person who is interested in dating someone that you’ve learned is transgender), ask.
Don’t confuse gender nonconformity with being transgender. Not all people who appear androgynous or gender nonconforming identify as transgender or desire gender affirmation treatment.
Keep the lines of communication open with the transgender person in your life.
Get support in processing your own reactions. It can take some time to adjust to seeing someone you know well transitioning. Having someone close to you transition will be an adjustment and can be challenging, especially for partners, parents, and children.
Seek support in dealing with your feelings. You are not alone. Mental health professionals and support groups for family, friends, and significant others of transgender people can be useful resources.
Advocate for transgender rights, including social and economic justice and appropriate psychological care.Familiarize yourself with the local and state or provincial laws that protect transgender people from discrimination.
Where can I find more information about transgender health, advocacy and human rights?
- American Psychological Association Office on Sexual Orientation and Gender Diversity Programs and Projects 750 First Street, NE Washington, DC 20002 Email
- Children's National Medical Center Gender and Sexuality Advocacy and Education 111 Michigan Avenue, NW Washington, DC 20010 (202) 476-4172
- Family Acceptance Project San Francisco State University 3004 16th Street, #301 San Francisco, CA 94103 Email
- FTMInternational (FTM means Female-to-Male) 601 Van Ness Ave., Suite E327 San Francisco, CA 94102 (877) 267-1440 Email
- Gender Spectrum (510) 788-4412 Email
- National Center for Transgender Equality 1325 Massachusetts Ave., Suite 700 Washington, DC 20005 (202) 903-0112 (202) 393-2241 (fax) Email
- Parents, Families, and Friends of Lesbians and Gays (PFLAG) Transgender Network (TNET) PFLAG National Office 1828 L Street, NW, Suite 660 Washington, DC 20036 (202) 467-8180 Email
- Sylvia Rivera Law Project 147 W. 24th Street, 5th Floor New York, NY 10011 (212) 337-8550 (212) 337-1972 (Fax) Email
- Transgender Law Center 870 Market Street Room 400 San Francisco, CA 94102 (415) 865-0176 Email
- TransYouth Family Allies P.O. Box1471 Holland, MI 49422-1471 (888) 462-8932
- World Professional Association for Transgender Health Email
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, D.C.: Author.
American Psychological Association. (2008). Answers to questions: For a better understanding of sexual orientation and homosexuality . Washington, D.C.: Author.
Coleman, E., Bockting, W., Botzer, M., Cohen-Kettenis, P., DeCuypere, G., Feldman, J., ... Zucker, K. (2012). Standards of care for the health of transsexual, transgender, and gender nonconforming people (7th version). International Journal of Transgenderism, 13 , 165-232. doi:10.1080/15532739.2011.700873
National Center for Transgender Equality and the National Gay and Lesbian Task Force. (2011). Injustice at every turn .
World Health Organization. (1990). ICD-10: International classification of diseases and related health problems (10th ed).
Purchase this brochure
Pamphlets in English and Spanish may be purchased in bundles of 25 for $4.00 plus shipping by calling (800) 374-2721 or by email .
Other versions
This pamphlet also is available in the following languages:
Arabic (PDF, 191KB)
Traditional Chinese (PDF, 376KB)
Simplified Chinese (PDF, 297KB)
English (PDF, 206KB)
Russian (PDF, 140KB)
Spanish (PDF, 568KB)
Related resources
- Sexual orientation and gender diversity
- Transgender Identity Issues in Psychology
- Guidelines for Psychological Practice with Transgender and Gender Nonconforming People (PDF, 472KB)
- APA LGBTQ Resources and Publications
You may also like

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- BJPsych Bull
- v.47(2); 2023 Apr
- PMC10063975
Transgender children and young people: how the evidence can point the way forward
Philip graham.
University College, London, UK
Associated Data
Data availability is not applicable to this article as no new data were created or analysed in this study.
The development of gender identity in children from around the age of 3 years is described. Wishes for transgender identity are distinguished from gender-atypical behaviour. Reasons for the recent rise in transgender referrals in the early teen years are discussed. The now widely used protocol developed by the Amsterdam group for assessing transgender children and young people and, where appropriate, offering them puberty blockers, cross-sex hormones and sex reassignment surgery is described. Evidence for the effectiveness of this approach is considered. The competence of young people to give consent to these procedures is discussed. Finally, proposals are made for topics urgently requiring further research.
Children first begin to develop a sense of biological gender at around the age of 2 to 3 years. 1 At this age, they are able to label pictures of boys and girls according to typical presentations of heteronormativity. At 4 years, boys understand that it is the possession of a penis that marks them out as biologically male and girls understand it is the lack of a penis that means they are biologically female. By this age, children have a sense of the stability of biological gender, an understanding that it remains constant with time. From this point up to the age of 6 or 7 years, their judgement of gender in pictures of clothed children is heavily influenced by appearance so that they label boys pictured in dresses as girls and boys with long hair as girls. By 7 years they recognise biological sex as constant and independent of external appearance. 1
By the age of 7 years, therefore, children understand three different concepts related to sex/gender identity: biological sex, self-perceived gender identity and social gender identity. They understand that they and others are biologically male or female, that they and others have a sense of their own gender identity as male or female and that they and others, depending on their appearance and clothing, are usually perceived by others as male or female. As they develop into adolescence and adulthood, people recognise that, with the use of hormones and surgical interventions, some features of biological sex can be changed. Both self-perceived gender identity and social gender identity may also undergo change.
The great majority of young children develop a self-perceived gender identity consonant with their gender assigned at birth, but some, from the age of 3 or 4 years, develop a self-perceived gender identity which is other than that assigned at birth. This sense of another gender identity can be accompanied by a feeling of discomfort or gender dysphoria. There are many autobiographical examples of the first awareness of gender dysphoria. The best known is that written by Jan Morris, who lived as a highly successful male journalist under the name of James Morris until her mid-30s when, following treatment with hormones, she underwent a surgical reconstruction and thereafter lived as a woman. 2 Jan Morris describes very clearly the onset of her gender dysphoria: 2 ‘I was three or perhaps four years old when I realized I had been born into the wrong body and should really be a girl. I remember the moment well, and it is the earliest memory of my life’ (p. 1). Her sense of discomfort with her assigned gender at birth persisted throughout her childhood, adolescence and early adult life. She describes how, when in role as a young man, she used to pray ‘please God make me a girl’ (p. 39). Gender dysphoria persisted throughout her marriage and parenthood. It was only in her late 30s, after she had had gender reassignment surgery, that she felt at ease.
The majority of prepubertal girls and boys have a clear sense of their own gender identity as female or male. This is nearly always consistent with their gender assigned at birth; in some, like Jan Morris, it is not. In a study of adolescents who had been referred to a gender identity clinic in earlier childhood, Steensma et al were able to show that a high proportion of prepubertal children with gender dysphoria did not continue to show such dysphoria after puberty, 3 a finding that had previously been reported by the same group. 4 Further, children who had shown gender-atypical behaviour (see below) without intense gender dysphoria did not generally show gender dysphoria in adolescence. Those with gender dysphoria who had been assigned a female gender at birth were less likely to desist than those assigned a male gender. Those who persisted were much more likely to have a homosexual or bisexual orientation.
A sense of gender identity must be distinguished from the presence of gender-atypical behaviour, which may occur with or without gender dysphoria. Gender-atypical behaviour (boys behaving like girls and having interests generally regarded as feminine and vice versa ) is not uncommon in the general population. In a total population study, using a standardised instrument, Golombok et al were able to identify 112 boys and 113 girls aged 3.5 years who showed gender-atypical behaviour to an extreme degree. 5 This represented about 2.2% of the population studied (S. Golombok, personal communication, 5 Jan 2021). Especially for girls, there was considerable continuity between gender-atypical behaviours at 3.5 years and such behaviour at the age of 13 years. These investigators do not report whether any of the children in their study were referred for gender dysphoria. The prevalence of 2.2% for gender-atypical behaviour needs to be contrasted with the much less frequent prevalence of 1 per 6800 Dutch adolescents aged 12 to 18 years who requested medical help for gender dysphoria. 6
Gender dysphoria and the onset of sexual feelings
Between 9 and 13 years of age, children start to experience sexual feelings arising from their genitalia. This onset of sexual feelings coincides with biological changes known as gonadarche. At this point, as a result of changes in the hypothalamus and pituitary, the gonads begin to secrete the sex hormones, testosterone and oestradiol, in relatively small quantities. This results in a modest growth of hair around the pubes and in the armpits and growth of the penis and breasts respectively. Spontaneous penile erections and clitoral excitement occur. Around 2 years later, positive feedback occurs in the hypothalamo–pituitary–gonadal axis which stimulates the testes to produce much larger amounts of testosterone and the ovaries to secrete more oestradiol, leading to menstruation. These hormonal changes also result in much more intense experience of sexual desire.
In the majority of children, sexual attraction is heterosexual but around 10% of 16- to 44-year-old adults report some previous sexual contact with a member of the same sex. 7 Most of those who experience homosexual attraction are not transgender. Usually, they have not even shown gender-atypical behaviour; they have been typically masculine, if boys, and feminine, if girls. Transgender boys usually, but not always, feel attraction to others of the same natal sex, i.e. they have homosexual feelings, and transgender girls similarly feel attracted by others of the same natal sex. Inevitably, these sexual feelings are often associated with some degree of confusion and uncertainty. For most transgender boys and girls, however, homosexual feelings have the effect of confirming the child in their transgender role: ‘If I'm really a girl, it isn't surprising I'm attracted to boys’, a transgender natal boy might say to himself and vice versa for girls. But some transgender children develop sexual attraction for others of the opposite natal sex, again with the creation of confusion and uncertainty over the transgender role.
Adolescence and gender identity
Adolescence is a social construction, i.e. it is a phase of life defined by society. 8 In Western society, it is regarded as beginning at the onset of biological puberty. Its end is not, however, defined biologically, but usually by a social criterion such as the age at which the individual develops significant autonomy. In practice, most psychologists, clinicians and members of the general public equate adolescence with the teen years, from 13 to 19, although many young people are well into biological puberty by 13 years and will have completed the biological changes of puberty well before 19 years. Recently, Sawyer and colleagues in an influential article have argued for an expanded and more inclusive definition of adolescence corresponding with the longer period of transition from childhood to adulthood now experienced by young people in Western society. They suggest that the period of 10 to 24 years is more consistent with this experience. 9 It is of relevance that there is considerable variation in ages at onset and termination of biological puberty, some young people normally starting at 10 or 11 years old and others not completing puberty until their later teen years. Relatively recent neuroscientific studies have pointed to the fact that rapid biological changes occur in the brain during the teen years, 10 but these are by no means specific to this phase of life. 11
The general public regard various behaviours as characteristic of adolescence. These may be summarised as impulsiveness, a tendency to take risks, moodiness and fractious relationships with parents. The public image of adolescents accords with this view of ‘the typical adolescent’. It is certainly the case that some teenagers show these characteristics, but population studies suggest that they make up no more than about 10–15% of this age group, 12 although they are certainly the most conspicuous. Another important and, in the context of this article, the most relevant feature of adolescence is thought to be self-questioning about identity. Young people of this age are seen as preoccupied with the question ‘Who am I?’, a question relating to all aspects of their identities, including their gender and sexuality. Such self-questioning is not experienced in intense form by most teenagers. The prevalence of ‘identity problems’ was found to be 14.3% in a group of 15- to 18-year-old American high school students 13 and a similar prevalence of ‘identity distress’ was found in a study of Flemish adolescents and young people aged 14–30 years. 14 The considerable increase in exposure of teenagers in the past 10 to 15 years to social media replete with references to gender identity would make it surprising if there had not been at least some increase of such self-questioning and confusion in this area.
Teenage presentation of transgender
Clinics serving the adolescent transgender population observed a change in the referral pattern after about 2005. Most notably, the gender identity clinic in Toronto, Canada, reported a dramatic increase in referrals at that time. 15 At the Portman Clinic in London (part of the Tavistock and Portman NHS Trust) referrals increased very significantly from 2009 to 2016. 16 At the Tampere University Hospital, Finland, referrals between 2011 and 2013 far exceeded the number expected from the findings of epidemiological studies. 17 This had not been the case previously. There were two other changes in the referral pattern over this period. First, previously, roughly equal numbers of boys and girls had been referred, whereas the increase was associated with much higher numbers of those who had been assigned female gender at birth. Second, previously, the rates of mental ill health among referred children had been about the same as in the general population, 18 whereas now much higher rates of psychiatric disorder, including autism, were reported. 14 , 16
It is therefore clear that from 2005 in Toronto and a few years later in other centres, the characteristics of patients referred to transgender clinics in their early and mid-teen years changed very significantly. In considering the reasons for this new pattern, Aitken et al 15 suggest that one possibility is that, during this period, societal factors made it easier for gay and lesbian youth and their families to seek clinical care. It could be argued, those authors say, that it became easier for girls to ‘come out’ than boys. It might therefore be easier for girls to opt for a transgender identity. Although there is no evidence to this effect, transgender natal girls who found themselves attracted to girls at puberty might have also found it easier to come out as transgender than hitherto. This implies that the increased presentation at adolescence was of girls who had experienced gender dysphoria since their early years. There is another possibility. It is that girls in their teens who are showing mental health problems for other reasons might, searching for an answer to their identity problems or distress, be influenced by social media to question for the first time their gender identity and to see gender change as an answer to their mental dilemmas. This might be more likely if they had previously shown ‘tomboyish’ behaviour. This possibility has been suggested in considering reasons for an increase in referrals of natal girls to a gender identity service between 2009 and 2016. 15 However, both these possibilities remain hypothetical at present and the reasons for the increase in referrals to transgender clinics is unknown.
Although one should not draw conclusions from a single case, it is of interest that one of the claimants in a judicial review brought about because they felt they had been inappropriately treated with puberty blocking drugs gives an account of her transgender development very much in accord with this second possibility. The claimant described a highly traumatic childhood in which she showed many gender-atypical behaviours: ‘ From the age of 14 she began actively to question her gender identity and started to look at YouTube videos and do research on the internet about gender identity disorder and the transition process’ (para. 78). 19
Although some cases of first presentation of transgender in the early teen years may arise from so-called adolescent identity problems or identity distress, it is likely that others do occur because the young person has been reluctant to come out as transgender beforehand, even though gender dysphoria has been present from the early years. Further, it is well established that such reluctance may persist well into adulthood, so that there are a number of recorded cases of people who have waited until their 30s or 40s to make this decision. 20
There is a need for both quantitative and qualitative research to investigate the early histories of girls referred with gender dysphoria for the first time in adolescence. Such research should include interviewing parents about their children's early years.
Life for children who are transgender from their early years can be challenging. At home, they have to try to communicate how they feel to potentially sceptical parents. At school, they are likely to experience disbelief, mockery and bullying. To cope they need resilient personalities as well as sensitive and understanding parents who are able to explore and talk openly about their children's feelings with acceptance and without trying to influence decisions one way or another. For, as we have seen, although some prepubertal children persist in their transgender identity, in the course of time many will, for reasons we do not understand, desist. 3 It is remarkable that most children who have been transgender from a young age reach adolescence without developing a higher-than-expected rate of significant mental health problems. 17
Many prepubertal children and their parents will benefit from having available a sympathetic counsellor, psychotherapist or other mental health professional. This will allow exploration of the reasons for the presence of gender dysphoria. Material from voluntary organisations such as Mermaids may be helpful, but parents of young children need to monitor this to ensure that their children are not being encouraged to persist, but are just accepted for what they are at the present time. Difficult decisions about changes of name and the use of toilets need to be negotiated with hopefully sympathetic, open-minded teachers.
As puberty approaches, difficult decisions have to be made. The Amsterdam group has been offering transgender adolescents puberty blockers for 30 years, their first case having been treated in 1991. 21 The group has pioneered an approach to assessment and management of gender dysphoria. It has produced a protocol for medical treatment of transgender children and adolescents that has been widely followed, 22 for example in Italy, Canada, the USA and the UK. The protocol is summarised below and in Box 1 :
- Psychological counselling for children and parents starts well before any medical treatment is considered and continues while such intervention is being administered.
- Once Tanner stage 2–3 is reached, and not before, gonadotropin-releasing hormone analogues (GnRHa) are prescribed where there is a clear indication that this is the appropriate course. This medication is given to block pubertal changes, so that the bodily changes rejected by the young person do not occur. Such treatment is only offered to children and young people aged 12 years and older who have intense gender dysphoria and no significant mental health problems. Informed consent by the young person and by the parents is required. The purpose of the use of puberty blockers is to ensure that young people with gender dysphoria do not live through pubertal bodily changes they find abhorrent. Further, the blocking of pubertal changes means that when, as is nearly always the case, transgender adults choose to have at least some degree of gender reassignment surgery, some procedures, particularly bilateral mastectomy for those assigned female gender at birth, will not be necessary.
- With careful assessment and selection, a very small minority of young people prescribed puberty blockers (between 1.4 and 3.5%) change their minds and do not wish to proceed further. 23 For the large majority who do wish to proceed, around the age of 16 years or older, cross-sex hormones are prescribed. For this treatment to be started, the young person must be living in the role of the preferred gender. Again, informed consent by the young person and, preferably, the parents is required.
- At the age of 18 years or older, those (again the great majority) who meet eligibility criteria can begin the process of gender reassignment surgery. Such surgery occurs variably according to the degree and at the pace desired by the individual concerned.
Management of gender dysphoria 22
- Make a full assessment as early as possible
- Follow with supportive counselling throughout childhood and adolescence
- Subsequent interventions should only take place with informed consent, first by parents and then by the young person, with reflection before each phase
- If intense gender dysphoria persists, consider using puberty blockers at Tanner stages 2–3
- Consider use of cross-sex hormones at age 16
- At age 18–19 and subsequently, consider gender reassignment surgery
Effectiveness of treatment
The aims of treatment are twofold:
- to explore with the child or young person with gender dysphoria the reasons for their discomfort with their gender assigned at birth and to consider alternative ways forward, including living in the role of their birth-assigned gender or pursuing medical intervention that will enable them to transition;
- in those who choose to live in their preferred transgender role, to start treatment, pausing for reflection before each step, first with puberty blockers, then with cross-sex hormones and finally with gender reassignment surgery to relieve gender dysphoria.
Among those who opt for medical treatment, the degree of success of intervention is measured by the absence of gender dysphoria and mental health problems and by the presence of psychological well-being. Ideally it would be possible to quote findings from a number of controlled trials of each of the interventions. Given the impracticability of obtaining agreement from children and young people with intense gender dysphoria to participate in controlled trials, the findings from uncontrolled but carefully conducted studies provide the main evidence for effectiveness.
There have now been a number of such uncontrolled studies, in which patients have been followed up to see whether their physical and psychological states have improved or deteriorated after the use of puberty blockers alone 24 – 26 and puberty blockers followed by cross-sex hormones followed by surgery. 27 – 29 The most recently published study of the effects of puberty blockers was reported from the Portman Clinic, London. 30 This study reported on the short-term outcome over 2 years of 44 children and young people aged 12 to 15 years when they started treatment with puberty blockers. Overall, the patient experience was positive. Although there were some children who showed some negative outcomes in mood and quality of relationships with family and friends, the majority showed positive change. There was no change in the rate of parent- or child-rated behaviour problems or risk of self-harm. All adverse effects, when they occurred, were mild. In line with other studies, only 1 of the 44 children and young people treated with puberty blockers did not go on to request cross-sex hormone treatment.
All the studies quoted above have provided valuable information. In all cases, there has been benefit from the interventions for the majority and an absence of significant harm. The most recent critical review of the use of puberty blockers has concluded: ‘Although large long-term studies with diverse and multicultural populations have not been done, the evidence to date supports the finding of few serious adverse outcomes and several potential positive outcomes. This literature suggests the need for transgender youth to be cared for in a manner that not only affirms their gender identities but that also minimises the negative physical and psychological outcomes that could be associated with pubertal development’. 31 In all published cases, the majority has reported benefit from the interventions and an absence of significant harm. Where it has been measured, an improvement in psychological well-being has always been found. It is well established that adults who transition ‘experience fewer psychological problems and interpersonal difficulties as well as a strongly increased life satisfaction’ than before the transition and show no wish to revert to their gender assigned at birth. 32
It should be added that the use of puberty blockers in early adolescence has been strongly criticised. 33 , 34 It has been claimed that there has been undue reliance on an affirmative approach (self-identification) in making a transgender diagnosis, that the complexity of the underlying problems of young people presenting as transgender has been inadequately assessed, that a high proportion of those who are treated with puberty blockers regret that they have received this treatment and that the young people who have been treated have not been capable of giving informed consent to treatment that has such profound implications for their future.
Adverse effects of medical interventions
The effect of puberty blockers is generally, though not universally, regarded as reversible. Their use has been associated with apparently reversible stunting effects on height velocity and bone maturation. 29 , 35 General cautions that have been expressed by clinicians about the possibility of irreversibility, such as those by Professor Butler and Dr de Vries quoted in a judicial review, 19 are no more than one might expect in relation to a large number of interventions in routine use. Caution about possible harm is always an appropriate clinical stance. It should not be taken to mean that the intervention in question should not be used where it is indicated.
There is one undeniable loss that occurs as a result of the use of puberty blockers. The individual does not go through the experience of the ‘normal’ adolescence he or she would have had without their use. However, most transgender young people do not consider this to be a loss or in any way regrettable.
The use of cross-sex hormones exposes the individual to the risk of a metabolic abnormality in about 15% of cases, but the significance of this finding is not clear and it does not seem a contraindication to their use. 36 Further research is required on the nature of possible metabolic abnormalities arising from the use of cross-sex hormones.
Informed consent
The competence of young people to give informed consent to the use of puberty blockers and cross-sex hormones is currently a matter of great relevance to clinical management. In UK law, 16 years is regarded as the youngest age at which it can be assumed, on the basis of chronological age, that a young person can give informed consent to a medical procedure. Below that age, it is widely accepted that, in considering whether a young person is capable of giving informed consent, the so-called Gillick principle should be applied. This principle, expressed by Lord Scarman in a 1985 House of Lords judgment and repeated in the above-mentioned judicial review, 19 is that ‘as a matter of law the parental right to determine whether or not their minor child below the age of 16 will have medical treatment terminates if and when the child achieves sufficient understanding and intelligence to […] understand fully what is proposed’. There is a controversy as to whether, because of the unusually complicated issues involved, children under the age of 16 could ever have the cognitive competence to give consent to puberty blockers or cross-sex hormones. This matter was considered in great detail in the judicial review whose judgment was published in December 2020. 19 This court decided that young people under 16 years could not give informed consent to the use of puberty blockers. Further, the court ruled that, even in cases where parents give their informed consent and clinicians are in agreement, an application should be made to the courts for authorisation before a child under 16 years can be administered puberty blockers. However, on appeal, this decision was reversed. The Appeal Court decided that the initial judgment had placed an improper restriction on the Gillick test and that it would not be appropriate for an application to the courts to be required before a child could be administered puberty blockers. 37
There is a need for systematic psychological investigation into the capacity of children and young people to make decisions in this area. Although there is some evidence on the capacity of young people aged 14–16 years to understand medical procedures, there is no evidence relating to the specific question of their understanding of the use of puberty blockers and cross-sex hormones, for example, in comparison with that of older people. Such evidence should be obtained. In the meantime, it would seem reasonable to rely on the findings of Weithorn & Campbell, whose study provides the most relevant data. 38 These investigators looked at 24 individuals in each of four age groups: 9, 14, 18 and 21 years. They tested their competence to make informed treatment decisions in a series of medical dilemmas, involving conditions such as epilepsy, diabetes and psychological problems. The children, adolescents and young adults were given the nature of the problem, treatments options, expected benefits, possible risks and consequences of failure, and then assessed on how much they understood. The 14-year-olds did as well as the 21-year-olds. The 9-year-olds did distinctly less well. Although it is many years since this study was carried out, until more relevant evidence is produced, there is no reason why its findings should not be regarded as highly pertinent.
Conclusions
One can conclude from the evidence that gender dysphoria is a relatively rare but well-defined condition, characterised by a strong desire to be of the gender opposite to that assigned at birth and by an insistence that one is, indeed, of the other gender. Affected transgender individuals are usually aware of its existence by the age of 5 years. Gender dysphoria needs to be distinguished from gender-atypical behaviour, where those assigned male gender at birth showed an interest in activities generally preferred by girls and vice versa . Marked gender-atypical behaviour occurs in around 2–3% of the population, most of whom are not transgender. Further, many children who show gender dysphoria before puberty do not continue to do so during and after pubertal changes occur. However, if gender dysphoria does persist into adolescence, its intensity tends to increase at this time.
From about 2005 until the present, there has been a considerable, perhaps tenfold, increase in the number of children and young people referred to gender identity clinics. This change has been observed not just in the UK, but in Canada, the USA and Finland. These more recent referrals have differed from previous cases in three ways. More recent referrals have been older, often not presenting until the early teen years. Whereas previously referrals were relatively evenly balanced between those assigned male and female gender at birth, there is now a considerable preponderance of those assigned female gender at birth. Further, whereas previously children and young people with transgender did not show high rates of behavioural and emotional disturbance, this is not the case for recent referrals.
The assessment and management of gender dysphoria has been pioneered by a Dutch group based in Amsterdam. This group has laid down a number of principles of management, which have been widely adopted by gender identity clinics in other countries. The effectiveness of this sequence of interventions is now reasonably well established, with good evidence that it relieves gender dysphoria and usually improves psychological well-being. Physical side-effects may occur but as far as can be ascertained at present, not to a degree where possible harm outweighs benefit. There are, however, unresolved issues concerning the capacity of young people with gender dysphoria to give informed consent to the use of puberty blockers.
There are a number of gaps in knowledge requiring urgent attention. First, it is unclear whether the considerable increase in referrals to gender identity clinics in the past 15 years is due to greater willingness of early affected individuals to come out at this age or whether clinics are dealing with a different population with different needs. There is clearly a need for both quantitative and qualitative research to investigate the early histories of those assigned female gender at birth referred with gender dysphoria for the first time in adolescence. Such research should include interviewing parents about their children's early years. Second, although it is reasonably well established that the use of puberty blockers is not accompanied by serious adverse effects, further research is required on the nature of possible metabolic abnormalities arising from the use of cross-sex hormones. Finally, there is a need for research into the capacity of children and young people, compared with older people, to understand the implications of the use of puberty blockers and cross-sex hormones.
About the author
Philip Graham is Emeritus Professor of Child Psychiatry in the Institute of Child Health, University College, London, UK.
Data availability
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
"I'm a trans woman – this is what I've learnt so far"
From an uplifting queer community to (at times) crushing gender dysphoria, my transition has been full of ups and downs. These are pieces of wisdom I wish I'd known earlier on in my journey

This will be my 14th trip to 2Pass as a trans woman . There, I will submit myself to a session of electrolysis, a form of permanent hair removal that involves eight hours of my face being injected with lidocaine, before each individual hair follicle is electrocuted with a fine metal probe. And yes, the experience is as delightful as it sounds. I will emerge swollen – so cartoonishly swollen, in fact, that the clinic will provide me with a letter to present to the passport control officers at Brussels station, in order to explain the visual discrepancy between my passport photo and the person before them, who will look more like Shrek than me.

It makes for a fairly traumatising experience – but it’s my only option after two and a half years of limited success with laser hair removal on my fair hair. It turns out that blondes don’t have more fun, they just have more electrolysis. For me, the results are just about worth it so that I can move forward in my transition, which can otherwise feel painfully slow at times. When I first started transitioning years ago, I would never have predicted hair removal would come to dominate my days. I wish someone had told me about the many challenges I’d face – and the many incredible realisations I’d have about myself along the way. Really, hair removal is just the tip of the iceberg.
There are some lessons I would love to have learned earlier – and the six below are probably the most crucial.
1/ Progress isn’t linear
When I first started transitioning, I drew up a roadmap of important milestones I expected to achieve by certain dates. It covered things like switching pronouns, starting hormone replacement therapy, coming out to my employer and going ‘full-time’ (in other words, presenting as a woman day-to-day). Committing this information to writing felt empowering; it gave me a sense of direction and a way to track my progress. Somewhere, at some point along the journey, I thought there would be an ‘Aha!’ moment when everything would just suddenly click into place: womanhood achieved, transition complete. This was admittedly slightly harder to schedule, but I was certain the moment would come, provided I worked hard and hit every target on the roadmap.
Well, guess what? So far, nothing has gone to plan and, on reflection I see how naïve I was to think it could. Transitioning isn’t a paint-by-numbers exercise. My roadmap didn’t account for the possibility of coming up against challenges, setbacks, the occasional need for off-piste travel, or even the simple fact that I might not want to take certain steps at the time I’d previously decreed I would. The reality is that my transition has felt much more like a game of snakes and ladders – three steps forward, two steps back. Some of the procedures I have undertaken to address my gender dysphoria have, frustratingly, only made it worse – at least in the short term (see my Shrek-style experience above). Even the moments when I felt invincible and brimming with self-confidence could quickly collapse into insecurity if I so much as detected a funny look from a stranger. Nothing has felt guaranteed, and I’ve learnt to just roll with the punches.
2/ Self-discovery can be awkward
Remember the makeover montage scenes in early Noughties films, where just removing a pair of glasses or swapping paint overalls for a slip dress would somehow catapult the heroine into social acceptance? There’d be a rock’n’roll soundtrack, maybe a round of high fives. Transitioning isn’t like that: it’s weird and gawky and painfully slow, and mostly just trial-and-error. For me, there were the mullet months, when, in waiting for the sides of my hair to catch up with the back, I unintentionally looked like an extra from Footloose ; there was the whole year it took my non-existent right breast to catch up with my fairly developed left; there was that strange period of androgyny, when I neither resembled a girl nor a boy, and so was misgendered by strangers as frequently as I was gendered correctly. And then there was the irrational dread of travelling under my old passport, and coming face-to-face with a pre-transition me like some unwelcome run-in with an ex.
.css-1pfpin{font-family:NewParisTextBook,NewParisTextBook-roboto,NewParisTextBook-local,Georgia,Times,Serif;font-size:1.75rem;line-height:1.2;margin:0rem;padding-left:5rem;padding-right:5rem;}@media(max-width: 48rem){.css-1pfpin{padding-left:2.5rem;padding-right:2.5rem;}}@media(min-width: 64rem){.css-1pfpin{font-size:2.5rem;line-height:1.2;}}.css-1pfpin b,.css-1pfpin strong{font-family:inherit;font-weight:bold;}.css-1pfpin em,.css-1pfpin i{font-style:normal;font-family:NewParisTextItalic,NewParisTextItalic-roboto,NewParisTextItalic-local,Georgia,Times,Serif;} "Transitioning isn’t a paint-by-numbers exercise – I've learnt to just roll with the punches"
The thing is – and this really is the thing – with the best will in the world, you still can’t leapfrog the awkward parts of transitioning and skip to the finish line. To be honest, I’m not even sure that finish line even exists, at least not for me – I’ve embraced fridge magnet wisdom, particularly the phrase: “The journey is the destination”. And while it’s so easy, so tempting to focus on the before and after, I’ve found that it’s all the in-between stuff that really matters and has formed the bedrock of my own personal metamorphosis. Those awkward and sometimes ugly bits of self-discovery have empowered me to find a home in my own skin. So, if you can, remember to celebrate all of your gradual changes: month to month you are ushering in a new iteration of yourself, and there’s something quietly magical about that. Don’t miss out. Don’t yearn to skip ahead. All of you is a working title and it’s a privilege to watch yourself grow.
3/ Your community is everything
I cannot overstate the importance of queer friendships and connections. They have been a vital and meaningful reminder of my own humanity, that I am valid, that I belong and that I am heard, particularly at a time when it so often feels like I am still working out who I am. London is buzzing with queer-friendly spaces and I would encourage anyone who is in the infancy of their transition to explore queer culture at its grassroots, if you’re lucky enough to live in the city (or near any city that offers something similar). This could be a queer bar (I am a big fan of Dalston Superstore and The Glory ) or club night (check out Queer Frequencies ) or even a support group (mine was the now-defunct NW Girls).
"My transition has felt like a game of snakes and ladders: three steps forward, two steps back"
Whilst there’s obviously no blueprint for transitioning, social media can be another great resource: a place to feel connected, to gather useful and trustworthy information and to create your own personal support hub. I have loved following Dani St James (who posts uplifting content but never shyes away from discussing the uglier realities of transitioning), Shon Faye (who has made trauma-dumping an art form and, now, my drug of choice) and Charlie Craggs (who has this extraordinary ability to find levity and humour in bleakness and whose book, To My Trans Sisters , is one I’d recommend to everyone). I have found all their accounts informative and genuine; seeing these trans women talk about their experiences in such real and often exposing ways has been an inexpressible source of comfort to me. They’re also hilarious, encouraging and very strong on the meme front.
4/ The desire to ‘pass’ is problematic, but don’t hate yourself for wanting to
To my trans siblings: I get it. The will to ‘pass’. It’s almost unavoidable and, for many of us, it is a suffocating obsession. It can take a lot of work to appreciate that, in fact, there’s beauty in your transness – even when it doesn’t align with conventional aesthetics of cisgender beauty – that offers its own unique affirmation.
To the blissfully unaware: ‘passing’ describes someone who is invisibly trans. So, for example, a trans man is said to ‘pass’ if a stranger assumes he is a cisgender man without so much as a second glance. Passing is not about beauty: it’s about camouflage, blending into the fabric of everyday society without raising an eyebrow or arousing the ‘wrong’ attention. For a minority of trans people, passing is irrelevant. For the vast majority, the desire to pass can at times feel all-consuming and the only metric for judging the success of their transition.
The concept of passing is screwed up, and for so many reasons. It’s screwed up because it turns the lived realities of trans people into performance, some elaborate game of deception. It’s screwed up because it reinforces restrictive and damaging cultural attitudes to gender presentation. It’s screwed up because its empowerment of trans people is built on their very disempowerment – and their complicity in that disempowerment by willingly gatekeeping their own bodies. It’s screwed up because, despite all of these reasons, for so many the allure of passing simply cannot be helped – not when it promises apparent safety and the ability to walk the street without the expectation of discrimination, harassment or even violence along the way.
5/ An open mind can be invaluable
We live in a country in which we are consistently demonised, pathologised, stigmatised and delegitimised by mainstream media outlets. Trans people in the UK are already the group most likely to be the victims of violent crime, and there was a massive 56 per cent increase in hate crimes against trans people last year. What this means is that we move through the world in a state of hypervigilance, constantly assessing risk, judging safety and making snap decisions about how we will be received by strangers.
An unfortunate consequence of this fight-or-flight mentality is that we tend to assume the worst of people and, like a fire curtain, close our minds to people who we suspect will be unsympathetic to us. Yes, some people are assholes. This is an unavoidable fact of life. The vast majority, however, are not – and you’d be surprised at how expansive, compassionate and accepting their minds can be. Don’t let your own expectations of rejection and negative judgement exclude you from spaces that, while unfamiliar or even clumsy with your transness, are nonetheless welcoming of it; you might just find that the people inside those spaces become your unexpected allies.
"I cannot overstate the importance of queer friendships and connections"
The same goes for your existing support networks. Before I formally came out as trans, I lost hours agonising over all the ways my transition would test and disrupt these relationships. That I might lose friends felt a distinct possibility, not (thankfully) for their lack of sympathy but for their fundamental lack of understanding – they just might not ‘get it’, they might never ‘get it’. Many people, as you might expect, struggled with the idea of being born into the wrong body – but inviting them to share in my journey, to experience first-hand its high and lows, has afforded us the most extraordinary kind of renewed closeness.
Asking friends for advice about clothes and make-up (particularly how to do winged eyeliner). Confiding in my brother all my fears and doubts about staying the course. Holding each of my sisters’ hands as I navigate the journey home from Antwerp after yet another electrolysis session that has left me a dysphoric mess. Having my mum not only administer my quarterly hormone injection, but dutifully diarise the next one, and the next, because she knows just how important they are to me. Explaining to my dad why I’ve never been his son – not really, anyway. All of these moments, in their own way, have been profound bonding experiences.
6/ Engaging with hate rarely ends well
Honey, put the keyboard down. Trust me on this, Twitter is not your friend – no good that way lies.
I used to think that it was my duty to wade in on the ‘trans debate’. I’d trawl newspaper columns, the comments section on social media, televised political debates, even radio phone-ins, and be met each time with the same anti-transgender rhetoric. Surely, I thought, if I could just understand their point of view, if I could identify the root cause of their antipathy, I could dismantle it from the inside. But reasoning with trolls is a fool’s errand. Even where it’s possible to have a debate, it becomes a relentless game of whack-a-mole – you think you’ve eliminated one troll, only for five more to pop up in their place. It’s exhausting, demoralising and, in my experience, not even remotely worth it when the inevitable trade-off is your own mental wellbeing.
Now, to be clear, I’m not advocating a life of complete dissociation, nor am I suggesting that there isn’t value in trans activism. I’m saying that if you consistently look for hate, chances are that you will find it. Since opposition is so often louder than support, you might become blinkered to the reality that a lot of people – trans, cis, and everyone in between – are really rooting for you.

Why I’m here for a Practical Magic sequel

Should they do a second series of ‘Normal People’?

Gala Gordon recommends 'People, Places & Things'

This is what it's like to live with bipolar

Why Ryan Gosling can still do no wrong

Is gossip good for you?

The obsession with Sydney Sweeney's body

What 'Baby Reindeer' teaches us about compassion

Tom Ripley, style and the art of lying

Camille Charriere: Female misogyny is a problem

Why are we all so obsessed with reboots?
Things you buy through our links may earn Vox Media a commission
My surgeries were a bridge across realities, a spirit customizing its vessel to reflect its nature.

“However, to be ogbanje is to be categorized other and to bring alterity home in a way that transcends the more ordinary bifurcated ‘otherness’ of gender. We could even speculate that ogbanje children fall under a third category of gender, of human-looking spirit. This gender is marked from birth—as male and female statuses are marked—by special behaviors towards and physical adornment of the child. The sexual appearance of the ogbanje may, indeed, be seen as a sham—yet another promise that the ogbanje is likely to break in its refusal to act according to human norms.” — Misty Bastian, “Irregular Visitors: Narratives about Ogbanje (Spirit Children) in Southern Nigerian Popular Writing.”
The robot was called a da Vinci.
It was delicate, precise, inserted through my navel to slice my uterus and fallopian tubes into small unimportant pieces, which were then suctioned out of my body. The procedure had a technical name that filled my mouth — a robotic-assisted subtotal hysterectomy with a bilateral salpingectomy. I had to repeat this about seven times on the day of my surgery, as nurses came in with forms clarifying that I knew what I was getting, but I didn’t mind. I’d waited years for this surgery. In another life, I’d trained to be a surgeon myself, dissecting cadavers and cutting through layers of dermis and fascia and muscle with a ten-blade. But in this one, I was 28 and cold, my numb skin wrapped in a hospital gown as nurses draped warmed blankets over me. Still, anticipation rang clear chimes. I couldn’t wait for when they’d wheel me out of that operating room, finally sterile.
It had been five years since I figured out I was transgender, after falling into a vibrant queer scene in Brooklyn that showed me so many more ways to be than I’d ever known. I moved there from Massachusetts, leaving behind scalpels and skinned horses dangling from a warehouse ceiling at a veterinary school, coming to reddened cabaret nights and play parties and a brief stint as a drag king. With a new world wrapping around me, the discomfort that had been spreading sour and wrong through my body for ages finally had a name — gender dysphoria. It came with a sort of relief: If I knew what it was, I knew what I could do about it.
My best friend Rachel flew into upstate New York for the hysterectomy. After the excision, she unfolded a cot in my hospital room while I ordered waffles from room service. When the nurses came in, they tried to get me to stand up, but the pain was a riptide dragging me under. I swayed, nearly collapsing, so they eased me back into bed and upped my pain meds. I caught my breath as Rachel and I exchanged alarmed looks, her hand warm around mine.
“I didn’t think it would be this bad,” I managed to say.
“Me either,” she replied.
The nurse gave us a brief but incredulous look. “You got an entire organ removed from your body,” she pointed out. “It’s kind of a major surgery.”
I made it out of bed a few hours later, walking in slow motion around the hospital floor with my IV stand rolling beside me, my palm scraping against the walls and the nurse at my elbow. The next day, Rachel drove me home to my attic apartment. Most of my early recovery was spent there, in a wingback recliner the color of wet moss. It had a wooden handle on the side that opened the back hinge and made the foothold pop up with a creaky jerk, stretching the chair out. I slept in it for a week because I had difficulty standing up or bending into narrow angles, and my bed was too close to the floor. I was full of stitches and hydrocodone, and my guts had been rearranged. It wasn’t my first mutilation, but it was one of my best.
An ogbanje is an Igbo spirit that’s born into a human body, a kind of malevolent trickster, whose goal is to torment the human mother by dying unexpectedly only to return in the next child and do it all over again. They come and go. They are never really here — if you are a thing that was born to die, you are a dead thing even while you live. Igbo ontology explains that everyone is in a cycle of reincarnation anyway — you are your ancestor, you will become an ancestor, the loop will keep looping within the lineage. Ogbanje , however, are intruders in this cycle, unwelcome deviations. They do not come from the lineage; they come from nowhere. As such, it’s important for an ogbanje never to reproduce: if it did, it would contribute to the lineage, and when it died, its spirit would join those of the humans, participating in their reincarnation loop.
Removing a uterus is an efficient way to make sure this never happens.
While my gender had asserted itself in different ways since my childhood, one of its strongest features was always a violent aversion toward reproduction, toward having a body that was marked by its reproductive potential — a uterus to carry children, full breasts to feed them with. My first surgery was an outpatient procedure two years after I moved to Brooklyn, a breast reduction: some fat removed from my chest, some glands, some skin, nothing much. It required a letter from my therapist to prove that I was sane.
“I’ve never heard of anyone like this,” the surgeon told me. He was an old white man who had performed many surgeries on trans patients, from breast augmentations to double mastectomies. “Male to female, female to male, fine. But this in-between thing?”
I ground my teeth into a smile and handed him my letter, along with printed images of the chest I wanted. It was one that felt right for me, one that wouldn’t move much, wouldn’t sway with pendulous wrongness or leave me gasping shallow breaths because my ribs were encased in the flattening black of a chest binder every day. I paid his office $10,000 skimmed from my student loans and tried not to be angry at the hoops I had to jump through. If I’d asked for an augmentation, it would’ve been fine, but wanting smaller breasts in the absence of back pain was considered ridiculous enough to require a therapist’s approval. During my post-op visit, the surgeon complained that he’d never had to spend as much time in consultation with a patient as he had with me. We’d spent maybe 30 minutes together over a few appointments.
My scars hypertrophied, leaving shiny brown keloids and flat glossy rivers on my chest. Sometimes, when I felt like I wasn’t trans enough, I’d look at them to remind myself that I’d chosen to modify my body and even though dysphoria and surgery aren’t prerequisites for being trans, the scars still served as a grounding reflection of my own certainty. I wasn’t sure then what I was transitioning my body to, but I was clear that the gender I’d been raised as was inaccurate — I’d never been a woman.
After that first surgery, my depression lifted significantly. It was a connection I hadn’t made before, how my dysphoria was affecting my mental health — the suicide attempt I’d survived just four months before the surgery. The choice to finally modify my body felt like a big deal in large part because other people treated it that way. Their alarm was almost infectious, but I was the one who had to live in this body; I was the one who suffered in it. The reduction was simply a necessary procedure, something that helped pull me away from wanting to die, something that made living a little easier.
Still, there was a deep sense of transgression about what I was doing that I couldn’t shake, especially as a Nigerian. It was too easy to tune into our communities and hear the voices heavy with disgust, saying that what I had done was disfiguring, that God had made me one way for a reason and I had no right to say or do otherwise, that I was mutilating myself. There was an ideal my body was supposed to conform to, and I was deviating from it by having surgery. I was rejecting it as a center and choosing something else: a world where the deviation itself was the ideal. I chose it readily. I’ve never minded being a mutilated thing.
If ogbanje represent an overlapping of realities — a spirit who looks incredibly convincing as a human, then what does it look like for one to experience gender dysphoria and take surgical steps to resolve that? Our language around gender identity is often so Western, how can we intersect that with non-Western realities? For example, is there a term for the dysphoria experienced by spirits who find themselves embodied in human form? It was inevitable that I’d be drawn to these overlaps, since I live there, inhabiting simultaneous realities that are usually considered mutually exclusive.
The possibility that I was an ogbanje occurred to me around the same time I realized I was trans, but it took me a while to collide the two worlds. I suppressed the former for a few years because most of my education had been in the sciences and all of it was Westernized — it was difficult for me to consider an Igbo spiritual world equally, if not more valid. The legacy of colonialism had always taught us that such a world wasn’t real, that it was nothing but juju and superstition. When I finally accepted its validity, I revisited what that could mean for my gender. Did ogbanje even have a gender to begin with? Gender is, after all, such a human thing.
However, being trans means being any gender different from the one assigned to you at birth. Whether ogbanje are a gender themselves or without gender didn’t really matter, it still counts as a distinct category, so maybe my transition wasn’t located within human categories at all. Instead, the surgeries were a bridge across realities, a movement from being assigned female to assigning myself as ogbanje ; a spirit customizing its vessel to reflect its nature.
It is considerably difficult to convince a doctor to remove an uninjured organ, even if your wholeness depends on its absence, especially if that organ is a reproductive one and they think you’re a woman.
I didn’t have a letter for my uterus — it was too difficult to find a therapist who had experience with nonbinary trans patients and I didn’t have any money. But I thought perhaps I could save up for it one day, so I made appointments with a few gynecologists to discuss my options. I chose not to disclose my gender (or lack thereof), but instead expressed my desire for the surgery as an elective choice, only because I didn’t want children. The doctors received me with resistance and thin contempt.
“What if you change your mind?” they asked me, in exam room after exam room, metal and glass and white coats all blurring into a single closed door. I had a thousand comebacks but I bit them all back because these people had what I needed — gloved hands to cut me open and toss my uterus into the bright plastic of biological waste, or wherever unwanted organs end up. My dysphoria had built a tight knot of a home in my body, since I had no idea how I was going to afford another surgery or, at this rate, even find a doctor willing to perform it. It wasn’t as severe as before my first surgery, but it was still there — a reminder so red it was almost black, showing up every month. I couldn’t rest easy knowing there was even a chance I could get pregnant, so I tried an IUD. When they inserted it, I screamed from the pain, the excruciating wrongness of something passing through my cervix. In the months afterward, I bled too heavily, through ultra tampons and overnight pads, flooding menstrual cups. Eventually, an ultrasound showed that the IUD was out of position, so they had to remove it. It felt like my body had spat it out, a reminder that nothing short of an excision would suffice.
I’d left Brooklyn and moved upstate by then, to the attic apartment with the moss green recliner. Occasionally, I would have bouts of searing pelvic pain that trapped me in bed for hours. A few weeks into my second winter there, I went to see a urogynecologist, thinking there was something wrong with my bladder. It took the entire afternoon to run tests; then he called me into his office to tell me there was an 84 percent chance I had endometriosis. “We could put you on birth control,” he suggested. I refused.
“Why not?” he asked, and just like that, the air in his office stopped moving. I could feel my nerves jangling, the familiar taste of the moment right before each and every disclosure like a sharp film over my tongue.
It’s easier when I’m alone. My friends and family know I’m not a woman — I’ve told them — but some continue to think of me as one anyway. I ignore it because sometimes it’s easier to not fight, to accept the isolation of being unseen as a safe place. I exist separate from the inaccurate concept of gender as a binary; without the stricture of those categories, I don’t even have to think about my gender. Alone, there’s just me, and I see myself clearly.
Speaking to other people, though, requires channeling who or what I am into language they can understand. “I’m trans,” I explained. “And I’ve had a breast reduction, so hormones would reverse that.”
The doctor nodded while my stomach churned. “I’ve had a few trans patients,” he said. “We could do a hysterectomy, if that’s something you’d want. Your insurance would cover it.”
I stared at him, hope and disbelief numbing my hands. I’d been terrified that he was going to say something transphobic, that I’d have to deal with the violence of that tearing through my skin, a bullet I hadn’t scheduled when I showed up there that afternoon. Instead, when I left his office, I had a surgery date only two weeks away.
He renovated my navel during the hysterectomy, unfolding it and then tucking it back into my abdomen in its new configuration. At my post-op appointment, he called the nurse over to brag about how well it had healed. There were only two small scars, each barely a centimeter long, at the top and bottom of my new navel. I called my mother a week or two after the surgery and told her what I’d done, even though I knew she wouldn’t understand. She sighed with the resignation of a mother who has tried to stop her child before and failed. “Could you try not to cut off any more parts of your body?” she said, and I laughed so hard my stitches hurt.
I flew to her house for Christmas a few days later, attendants pushing me around both airports in a wheelchair, weak but giddy. The rest of my recovery was uneventful. After 17 years and approximately 200 periods, I slipped easily into my new and bloodless life.
There is a vivid history of mutilation with ogbanje : a dead one can be cut, scarred to prevent it from returning undetected. Ogbanje are also a cohort, they separate from each other when they get born, but they return to the cohort when they die. I like to think that there is a form of shared or generational memory within that; being dead or mutilated are not unfamiliar things to any of us, we’re not afraid of either.
It has been grueling to remake myself each time I learn more about who or what I am — to take the steps that such remaking requires, to bear the costs. Sometimes, those costs are worn on your heart, like when the people you love no longer have space in their worldview for you. Other times, it’s the body that bears them, in markings and modifications. By now, I’ve come to think of mutilation as a shift from wrongness to alignment, and of scars as a form of adornment that celebrates this shift. The keloids on my chest and the small lines spilling out of my navel function as reminders — that even when it meant stepping out of one reality to be swallowed by another, I kept choosing to move toward myself.
- first person
- transgender issues
The Cut Shop
Most viewed stories.
- What’s the Deal With ‘Hawk Tuah’ Girl?
- J.Lo and Ben Affleck Have Reportedly Been ‘Over for Months’
- The Best Classic Jeans, According to Fashion Experts
- How the NDA Became the Defining Legal Document of Our Time
- Filth and Glory at Twinks vs. Dolls Olympics 3.0
Editor’s Picks

Most Popular
- Sports Are the New Dating Apps
What is your email?
This email will be used to sign into all New York sites. By submitting your email, you agree to our Terms and Privacy Policy and to receive email correspondence from us.
Sign In To Continue Reading
Create your free account.
Password must be at least 8 characters and contain:
- Lower case letters (a-z)
- Upper case letters (A-Z)
- Numbers (0-9)
- Special Characters (!@#$%^&*)
As part of your account, you’ll receive occasional updates and offers from New York , which you can opt out of anytime.
- Share full article

When Students Change Gender Identity, and Parents Don’t Know
Educators are facing wrenching new tensions over whether they should tell parents when students socially transition at school.
A student from California felt it was critical for his school to respect his gender identity after his parents expressed their hesitation. Credit... Morgan Lieberman for The New York Times
Supported by
By Katie J. M. Baker
For this article, Katie J.M. Baker interviewed more than 50 people, including parents and their children, public school officials, medical professionals and lawyers for both L.G.B.T.Q. and conservative advocacy groups.
- Published Jan. 22, 2023 Updated June 26, 2024
Jessica Bradshaw found out that her 15-year-old identified as transgender at school after she glimpsed a homework assignment with an unfamiliar name scrawled at the top.
When she asked about the name, the teenager acknowledged that, at his request, teachers and administrators at his high school in Southern California had for six months been letting him use the boy’s bathroom and calling him by male pronouns.
Mrs. Bradshaw was confused: Didn’t the school need her permission, or at least need to tell her?
It did not, a counselor later explained, because the student did not want his parents to know. District and state policies instructed the school to respect his wishes.
“There was never any word from anyone to let us know that on paper, and in the classroom, our daughter was our son,” Mrs. Bradshaw said.
The Bradshaws have been startled to find themselves at odds with the school over their right to know about, and weigh in on, such a major development in their child’s life — a dispute that illustrates how school districts, which have long been a battleground in cultural conflicts over gender and sexuality, are now facing wrenching new tensions over how to accommodate transgender children.
The Bradshaws accepted their teenager’s new gender identity, but not without trepidation, especially after he asked for hormones and surgery to remove his breasts. Doctors had previously diagnosed him as being on the autism spectrum, as well as with attention deficit hyperactivity disorder, PTSD and anxiety. He had struggled with loneliness during the pandemic, and, to his parents, seemed not to know exactly who he was yet, because he had repeatedly changed his name and sexual orientation.
We are having trouble retrieving the article content.
Please enable JavaScript in your browser settings.
Thank you for your patience while we verify access. If you are in Reader mode please exit and log into your Times account, or subscribe for all of The Times.
Thank you for your patience while we verify access.
Already a subscriber? Log in .
Want all of The Times? Subscribe .
Advertisement
Find anything you save across the site in your account
We Need to Change the Terms of the Debate on Trans Kids
Every night, when I walk my dog, several strangers, similarly tethered, will ask me the same two questions: “Boy or girl?” and “How old?” The pragmatic meaning of these questions escapes me. The answers do not inform the interactions between our dogs, nor do they tell a story. Wouldn’t it be more interesting to learn whether the dog was a longtime family member or a pandemic puppy, whether it lived with other pets, how much exercise it got or desired, how it tolerated last summer’s orgy of fireworks, or to learn at least the dog’s name? These are the questions I usually ask other dog owners as our pets sniff each other, but in response I am still asked—hundreds of times a year—about my dog’s age and gender. These categories, it seems, are so central to the way we organize the world around us that we apply them to everything, including random dogs in the night.
No wonder, then, that attempts to subvert these two categories make people uncomfortable and, often, scared and angry. This happens when children act with particular independence; when people challenge the norms of gender; and, especially, when both of these things happen at once, as in the case of trans children. In December, the British High Court of Justice ruled on the question of whether young people under the age of eighteen are capable of giving informed consent to treatments that forestall puberty. Such treatments can be prescribed to children given a diagnosis of gender dysphoria, both to alleviate discomfort that can stem from the physical changes brought on by puberty and to pave the way for later medical gender transition. The court ruled that children under sixteen cannot consent to such treatment because they are unable to grasp its long-term consequences, and cast doubt on the ability of young people between the ages of sixteen and eighteen to give informed consent. The decision effectively bars British children and adolescents from transitioning medically.
British media coverage of the High Court’s decision was generally positive. “Other countries should learn from a transgender verdict in England” the Economist wrote . “The court was correct to curb a disturbing trend,” the Observer wrote . Later in the month, the BBC’s media editor, Amol Rajan, published his list of the five best essays of the year, among them J. K. Rowling’s piece explaining her position “on sex and gender issues.” Rowling, who presents herself as a defender of bathrooms, dressing rooms, and other “single-sex spaces” against trans women, wrote that she was “concerned about the huge explosion in young women wishing to transition and also about the increasing numbers who seem to be detransitioning.” She cited the controversial hypothesis that some adolescent transitions may stem from a kind of social contagion. Had transition been an option during her own adolescence, Rowling wrote, she might have chosen it as a way to deal with her own mental-health challenges: “The allure of escaping womanhood would have been huge.”
In the United States, this line of argument has been advanced by Abigail Shrier, a writer for the Wall Street Journal who published a book last year titled “ Irreversible Damage: The Transgender Craze Seducing Our Daughters .” The cover art is a drawing of a prepubescent girl with a giant round cutout where her abdomen should be. The book is currently ranked “#1 Bestseller in Transgender Studies” on Amazon. Bills that would ban trans care for young people have already been prefiled for this year’s legislative sessions in Alabama, Texas, and Missouri; last year, a similar bill was defeated in South Dakota, thanks to opposition from the pharmaceutical industry. When such bills contain language explaining their rationale, they make similar arguments to those of Rowling, Shrier, and the British High Court: that the effects of trans care are irreversible and that many people who want to transition when they are adolescents will ultimately choose to identify with the gender they were assigned at birth.
The state bills tend to lump all kinds of trans care—puberty blockers, cross-sex hormones, and surgeries—together. As a narrative, this is not unreasonable: the vast majority of people who receive puberty blockers do go on to take cross-sex hormones, and many choose surgery. But the short- and long-term effects of the medical interventions are markedly different. Agonists of gonadotropin-releasing hormone, originally developed to treat prostate cancer and endometriosis in adults, can have the effect of preventing puberty-related changes: genital growth, breasts, body and facial hair, and voice changes. Estrogen promotes breast growth, and testosterone will likely lead to a lower voice and more body and facial hair; both kinds of hormones affect fat and muscle distribution. The effects of hormones are not as predictable—and the line between reversible and irreversible effects of hormone treatments isn’t as clear—as their opponents seem to think, but a person whose puberty is effectively prevented and who later receives cross-sex hormones is unlikely to preserve their fertility. Some European researchers are experimenting with reserving gonad tissue that may be used to create biological progeny later (similar efforts are made with children undergoing cancer treatment that is likely to render them infertile). Natal males and females who transition during adolescence forfeit their fertility equally, but Rowling, Shirer, and other opponents of pediatric trans care seem particularly concerned with people they see as girls clamoring to escape womanhood. (The lead plaintiff in the British case, Keira Bell, who was assigned female at birth, began taking puberty blockers at sixteen and testosterone at seventeen and had a double mastectomy at twenty. Bell later transitioned back to being female.)
“Women and children are always mentioned in the same breath,” the visionary feminist activist Shulamith Firestone observed in the book “ The Dialectic of Sex: The Case for Feminist Revolution ,” from 1970. “I submit . . . that the nature of this bond is no more than shared oppression. And that moreover this oppression is intertwined and mutually reinforcing in such complex ways that we will be unable to speak of the liberation of women without also discussing the liberation of children, and vice versa.” Firestone noted that women and children were inextricably linked not only by the women’s duty of childbearing and child rearing but by the obligation, for both groups, to maintain innocence, fragility, immaturity, and dependence on others. She saw the path to liberation in divorcing the reproductive function from women’s biology, and in abolishing childhood. One might argue that young people who seek trans care are pursuing both of these projects, and that is why they inspire such panicked opposition.
Yet the arguments in favor of trans care for young people are usually not so much liberationist as they are determinist. Advocates generally claim that trans children are innately, immutably different from cis children and that access to medical transition is essential for staving off depression and even suicide. “The fear that puberty per se can be a threat to life for transgender children permeates pediatric trans care,” Sahar Sadjadi wrote in an essay in Transgender Studies Quarterly last year. (Sadjadi is a medical anthropologist who has studied clinical practices for transitioning and other non-gender-conforming children for a decade.) This type of advocacy, she argues, builds on two long-standing tendencies: the habit of thinking of gender transition as primarily a medical process, and the habit of grounding L.G.B.T. civil-rights claims in “born this way” rhetoric. These habits make for a compelling, easily digestible argument: transness is an immutable characteristic, and denying young people access to medical transition can be tantamount to killing them. This argument is grounded in the lived experience of some advocates, whose own medical transition relieved extreme anguish. But an argument rooted in despair cannot and should not represent all young trans people.
When we are not talking about children and adolescents, trans people talk about a much broader range of options than medical transition—a spectrum of gender expression more varied than the linear path of puberty blockers followed by cross-sex hormones. Some adult trans people consider themselves binary, and some don’t; some use hormones and have surgeries, some choose one or the other, some try different approaches, and some eschew medical interventions altogether. Medical intervention requires a diagnosis of gender dysphoria, even if the person is paying for surgery and hormones out of pocket. In general, though, adults are not required to prove that they have always felt like they were in the wrong body (although some have).
If we hold to the premise that transness is an immutable, inborn trait, it follows that every young person who chooses to detransition will undermine the case any other young person may have for seeking trans care. “The main debate has become whether these young people will ‘persevere,’ ” Sadjadi told me by Zoom from Montreal, where she is on the faculty at McGill University’s Department of Social Studies of Medicine. “I think this is the wrong question. Gender changes with age. The gender of a fifty-year-old woman is not the same as of a five-year-old girl. Nothing terrible happens if a person transitions again, which is how I think we should think about it.”
The British High Court’s decision makes a point that appears compelling and compassionate. A child, the panel decided, cannot fully comprehend the meaning of infertility and possible loss of sexual function that come with transitioning at a young age. (One concern is that puberty blockers prevent genital growth, making gender-affirming bottom surgery more complicated.) But this argument rests not only on a narrow definition of sexual pleasure but on an impossible ideal of comprehension: we can never fully imagine loss, especially the loss of something we’ve never had. Keira Bell testified, “It is only until recently that I have started to think about having children and if that is ever a possibility, I have to live with the fact that I will not be able to breastfeed my children. I still do not believe that I have fully processed the surgical procedure that I had to remove my breasts and how major it really was.” As heartbreaking as that admission is, all available data indicate that such regrets are exceedingly rare. That one person’s testimony convinced the court to make a decision that will affect untold thousands tells us more about the pull that human reproduction has on the imagination than it does about gender transition.
“People change their minds about all kinds of decisions,” Sadjadi added. Hers is not an argument against thinking of transition as a serious, consequential decision, but rather an argument for viewing gender transition as one of the many important choices some people face. People—including young people, acting legally, with their parents’ support—choose to have babies, move continents, subject themselves to extreme physical risk by engaging in certain sports, make what often amounts to commitments to lifelong medical intervention with S.S.R.I.s for depression or stimulants for attention deficit hyperactivity disorder, join the R.O.T.C. or the National Guard. None of these decisions is just like the decision to transition. But are they really so much lighter, so much less consequential, that the possibility of one person reversing course shouldn’t prevent others from making the same choices?
In her 1970 book, Firestone discussed the arbitrary historical boundaries of childhood. In other eras, boys would be expected to abandon toys and take up adult vocations at the age of seven; girls were historically married off as soon as they went through puberty. Firestone’s point was that childhood was a relatively new category, and an unstable one. Our own ideas of maturity are no less arbitrary than our ancestors’. We know that a fifteen-year-old is probably better equipped to make life decisions than is a nine-year-old, who is still vastly more experienced and informed than a four-year-old. But for the purposes of the law, we lump them in the same category. An eighteen-year-old, on the other hand, is deemed capable of making the full range of life choices—except for whether to ingest alcohol. There is little doubt, however, that the experience, wisdom, and skill for assessing risk and making decisions continue to accumulate well past middle age. If you think about it, a fifty-year-old who has experienced life in a particular gender is in a much better position to make a decision about transition than is a twenty-year-old. But at that point, it’s too late to decide to be a young person in the other gender, and this, too, is irreversible. I began my own transition at fifty, long after experiencing the misery of pregnancy and the incomparable joy of breastfeeding. I have no regrets. Had I had the option of transitioning as a teen-ager, I would have chosen to do so—and I am almost certain that I would have had no regrets then, either, because I would have had a different life.
Sadjadi, who was a physician before she became an anthropologist, has written that puberty blockers are not as medically inconsequential as they are often portrayed. Although they appear to have no long-term physical effects if they are used for a short time (a year or less), some studies suggest that they can have long-term detrimental effects for the musculoskeletal system if they are used for three or four years. (Long-term data comes from the use of puberty blockers to forestall what is deemed “precocious” puberty, occurring in children under the age of nine.) The manufacturer of Lupron, the drug most commonly used as a puberty blocker, warns of depression as a possible side effect. Sadjadi suggested freeing gender transition in young people from the assumption that they will necessarily take puberty blockers. For some kids, she said, it may be worth considering social transition as the first or even only step. Social transition is often conspicuously absent from the menu offered to adolescents. For others, cross-sex hormones may be preferable to puberty blockers, which are supposed to “buy time” before a child is deemed old enough to make the commitment to transitioning. There is not enough data to say whether and when these may be the better care options.
To be able to talk about a range of transition options, at different times in life, we would need to change the terms of the debate. We would need to view both age and gender on a continuum, not as binary states. None of us has ever been as innocent and ignorant as the children of our imagination, and none of us will ever be as wise and competent as the adults we make ourselves out to be. What if we saw ourselves as always changing, always uncertain, but always capable of making choices? What if we accepted that some losses are desirable and some are regrettable, and that we can’t always know the difference? What if we knew that we are always changing not only as individuals but as societies, and the categories we use to sort ourselves mutate faster than we realize? Then maybe we could have a real conversation about trans care for young people.
By signing up, you agree to our User Agreement and Privacy Policy & Cookie Statement . This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.

- Tools and Resources
- Customer Services
- Conflict Studies
- Development
- Environment
- Foreign Policy
- Human Rights
- International Law
- Organization
- International Relations Theory
- Political Communication
- Political Economy
- Political Geography
- Political Sociology
- Politics and Sexuality and Gender
- Qualitative Political Methodology
- Quantitative Political Methodology
- Security Studies
- Share This Facebook LinkedIn Twitter
Article contents
Gender and transitional justice.
- Maria Martin de Almagro Maria Martin de Almagro University of Ghent
- and Philipp Schulz Philipp Schulz Institute for Intercultural and International Studies, University of Bremen
- https://doi.org/10.1093/acrefore/9780190846626.013.669
- Published online: 19 October 2022
Transitional justice (TJ) refers to a set of measures and processes that deal with the legacies of human rights abuses and violent pasts, and that seek to aid societies transitioning from violence and conflict toward a more just and peaceful future. Much like the study of armed conflict and peacebuilding more broadly, the study and practice of transitional justice was traditionally silent on gender. Historically, gendered conflict-related experiences and harms have not been adequately addressed by most transitional justice mechanisms, and women in particular have been excluded from the design, conceptualization, and implementation of many TJ processes globally. While political violence perpetrated against men remained at the center of TJ concerns, a whole catalogue of gendered human rights abuses perpetrated primarily against women has largely remained at the peripheries of dominant TJ debates and interventions.
Catalyzed by political developments at the United Nations within the realm of the Women, Peace, and Security (WPS) agenda and by increasing attention to crimes of sexual violence by the International Criminal Tribunal for Rwanda (ICTR) and the former Yugoslavia (ICTY), however, the focus in the 2000s has been radically altered to include the treatment of gender in transitional contexts. As such, considerations around gender and sex have increasingly gained traction in TJ scholarship and praxis, to the extent that different justice instruments now seek to engage with gendered harms in diverse ways. Against this background, to the authors review this growing engagement with gender and transitional justice, offering a broad and holistic overview of legal and political developments, emerging trends, and persistent gaps in incorporating gender into the study and practice of TJ. The authors show how gender has been operationalized in relation to different TJ instruments, but the authors also unearth resounding feminist critiques about the ways in which justice is approached, as well as how gender is often conceptualized in limited and exclusionary terms. To this end, the authors emphasize the need for a more sustained and inclusive engagement with gender in TJ settings, drawing on intersectional, queer, and decolonial perspectives to ultimately address the variety of gendered conflict-related experiences in (post)conflict and transitional settings.
- transitional justice
- truth and reconciliation commissions
- queer perspectives
- structural violence
- criminal courts
- reparations
- gender justice
- masculinities
- sexual and gender-based violence (SGBV)
Gender and Transitional Justice: An Overview
In July 2020 , the United Nation’s Special Rapporteur on the promotion of truth, justice, reparation, and guarantees of nonrecurrence issued a report on gender perspectives in transitional justice (TJ), which “considers multiple aspects of adopting a gender perspective in transitional justice processes” ( United Nation’s Special Rapporteur, 2020 , p. 4). This report came at a time when there had been much progress in gendering peacebuilding and transitional justice work ( Weber, 2021 ), but also when gender sensitivity in transitional justice work still remained elusive ( Ní Aoláin, 2019 ) and numerous gendered blind spots persisted in delivering justice for various gendered conflict-related harms and experiences.
Much like the study of armed conflict more broadly ( Sjoberg, 2016 ), the field of transitional justice was traditionally silent on gender ( Buckley-Zistel & Stanley, 2012 ; O’Rourke, 2013 ), leading feminist scholars to pose the question of “where are women, where is gender and where is feminism in transitional justice?” ( Bell & O’Rourke, 2007 , p. 23).
Partly in response to these questions, there has been a radical shift in viewing the role of gender in transitional justice, which has witnessed an increasing feminist curiosity ( Enloe, 2004 ) about gender justice in postconflict transitions ( Buckley-Zistel & Stanley, 2012 ). As such, considerations around gender and sex have increasingly gained traction in the growing TJ literature, to the extent that as of the early 21st century , gender constitutes “a burgeoning focus of investigation within TJ scholarship and practice globally” ( O’Rourke, 2017 , p. 117). For one, considering gender is important for participation and representation ( O’Rourke, 2013 ) in terms of ensuring equal participation and involvement of men, women, and persons with diverse sexual orientations, gender identities, and expressions and sex characteristics (SOGIESC) in the design and implementation of these processes—for instance, as active protagonists and beneficiaries but also as witnesses. At the same time, incorporating gender lenses and perspectives is crucial for broadening conceptions of gender, peace, and security ( Rees & Chinkin, 2015 ) and the types of violence addressed by different TJ processes—including, for instance, gendered socioeconomic harms ( Lai, 2020 ) or gender-based violence ( Aroussi, 2011 ). In particular, women’s movements around the world have led important efforts to ensure that gender justice is put at the center of political, legal, and humanitarian agendas of transitional justice ( Bell & O’Rourke, 2007 , p. 24); that sexual violence is considered a war crime ( Aroussi, 2011 ); and that transitional justice also addresses social, economic, and cultural rights, as well as collective rights to socioeconomic development ( Roht-Arriaza & Mariezcurrena, 2006 ). Collective reparations are based on a redistribution of resources and wealth to the most marginalized, and the concept extends the definition of “victims” not only to include those physically affected but to compensate for the social effects of war, such as hunger, disease, or forced displacement to which women are particularly vulnerable. In policy terms, much of this engagement with gender and transitional justice unfolds within the realm of the U.N. Women, Peace, and Security Agenda (WPS), spearheaded by United Nations Security Council Resolution 1325 , which, inter alia, focuses on access to justice, the rule of law, and the investigation and prosecution of wartime sexual violence ( Martin de Almagro, 2017 ).
Yet, despite this increasing engagement with gender, Fionnuala Ní Aoláin has reminded us that gender lenses and a “feminist presence in transitional justice is complex, multilayered and still in the process of engagement”( Ní Aoláin, 2012 , p. 205). As such, 15 years after Bell and O’Rourke’s call for feminist theorizing in TJ, “gender parity remains elusive in transitional justice implementation” ( Ní Aoláin, 2019 , p. 1), and numerous gendered blind spots persist. As such, various gendered experiences remain largely unaccounted for in the implementation and practice of dealing with the past, and existing TJ processes across the globe have largely fallen short in advancing actual transformations for women. In particular, structural forms of gender-based violence and discrimination, rooted in patriarchal value systems, need to be engaged with more comprehensively by TJ processes to continue to address violence across time and space, spanning from conflict to peace and beyond ( Cockburn, 2008 ). At the same time, an engagement with gender in transitional justice must be broader and more inclusive, moving beyond a singular focus on women (and on sexual violence against women, in particular) to also include masculinities and queer perspectives.
The objective of this article is to offer a concise yet comprehensive overview of developments and debates in scholarship and policymaking concerning gender and transitional justice. As such, the article aims to provide a state-of-the-field assessment of how an incorporation of gender into transitional justice processes and debates has unfolded since 2000 , and what gendered blind spots, gaps, and avenues for further engagement nevertheless persist. To this end, the section titled “ Historical, Political, and Legal Advances in Transitional Gender Justice ” will discuss the key historical and legal advances in transitional gender justice in a post-Cold War context. The section titled “ Gendering Transitional Justice Instruments ” then outlines how different transitional justice mechanisms have tried to deal with gender specific harms and women’s experiences from war, in retributive justice, truth seeking, and reparation processes. Based on this overview, the section titled “ Reparations ” offers dominant feminist critiques of these advances to transform women’s lives before moving on to an assessment of persisting gendered blind spots with regard to masculinities and queer perspectives in TJ. The article concludes by proposing some new avenues and strategies for transformative transitional gender justice.
Historical, Political, and Legal Advances in Transitional Gender Justice
Broadly referring “to the set of measures implemented [. . .] to deal with the legacies of massive human rights abuses” ( de Greiff, 2012 , p. 34) in the aftermath of armed conflicts or authoritarian regimes, the study and implementation of transitional justice (TJ) has significantly expanded and globalized since the beginning of the 21st century ( Teitel, 2015 ). Transitional justice mechanisms and institutions thereby seek to redress past wrongs, institutionalize the rule of law, and construct new legal and normative frameworks in postconflict contexts or in societies that have dealt with occupation or authoritarian regimes so as to prevent violent conflict from reemerging. Traditionally, transitional justice measures are a set of judicial and nonjudicial instruments and mechanisms, such as trials, truth commissions, lustration, or memorials. The aims of TJ are thereby often linked to the normative objectives of democratization, nation-building, and the primacy of the rule of law but also fostering a free market economy ( Rees & Chinkin, 2015 , p. 1012). This approach is embedded within a liberal peacebuilding model ( Sriram, 2014 ), which often unfolds through a primary focus on civil and political rights placed over an engagement with socioeconomic and cultural rights ( Hamber, 2016 ).
While there is not a predetermined set of standards on how and where transitional justice should be applied, the practice of TJ has frequently been critiqued for following a standardized toolkit or “one-size-fit-all” approach ( Sharp, 2013 ). At the same time, various scholars have emphasized that TJ mechanisms and their implementation must vary depending on geographical contexts ( Teitel, 2003 , p. 76), hence requiring a localization and contextualization of TJ processes ( Shaw & Waldorf, 2010 ). These dynamics in many ways also apply to the ways in which gender perspectives in TJ are conceptualized and understood, which often follow a standardized procedure but neglect the locally-contingent meanings of “justice” and “gender” in different geopolitical regions ( Schulz, 2019 ).
While many of the foundations of TJ date back to the post-World War II Tokyo and the Nuremberg criminal tribunals, the first time the actual concept of TJ was used was in the context of the collapse of the Soviet Union in the late 1980s and the reordering of geopolitical dynamics in Africa, South and Central America, and Eastern Europe ( Bell, 2009 , p. 7). Whereas certain countries descended to civil wars, particularly on the African continent, others started transitioning from authoritarian to democratic rule. This is important because since then, there has been a normative assumption that transitional justice needs to ensure the basis of a peaceful transition toward Western-like democracies based on liberal individualism ( Arthur, 2009 ; Rees & Chinkin, 2015 , p. 1212; Teitel, 2003 , p. 75). This historical origin has conditioned the horizon of possibilities of what justice means and which kind of measures are necessary to ensure it. While prosecutions, truth-telling commissions, reparations, and institutional reform of authoritarian and centralized states were deemed necessary, distributive socioeconomic justice was not ( Arthur, 2009 , p. 326). This liberal notion of justice has gendered and gendering consequences, as the discussion to unfold throughout this article demonstrates.
Over the decades, then, the study, praxis, and implementation of transitional justice in many ways experienced its own transition ( McEvoy, 2007 ), emerging from its initially exceptionalism origins toward becoming a standardized, institutionalized, and globalized practice ( Teitel, 2015 ). As such, transitional justice expanded to include a whole variety of processes, measures, and instruments, and to be applied to a wide range of violence-affected situations. Not only the points of departure, however, but also the end-goals of transitional justice processes are increasingly recognized as being more diverse than initially assumed, and transitional justice has been increasingly emancipated from the bonds of the assumingly linear transition from war to peace ( Sharp, 2013 ), which cannot live up to the complexities and nonlinearity of lived realities in times of violence, conflict, and peace ( Hamber, 2008 ). As part of this expansion process, transitional justice has over the years also been increasingly localized ( Shaw & Waldorf, 2010 ), turned its attention to (post)colonial dynamics ( Bueno-Hansen, 2015 ) or to socioeconomic aspects ( Lai, 2020 ), and has also become more attentive to the gender dynamics of political transitions ( O’Rourke, 2013 ).
Historically, however, the experiences of women have not been adequately addressed by transitional justice mechanisms and processes. Women experience direct violence, such as sexual violence, domestic and sexual slavery, forced displacement, and forced marriage. They also have more difficulties rebuilding their lives after war because gender norms and traditional women’s societal roles make it difficult for women to access property, land, and jobs, as well as health and education services. Nevertheless, the gendered nature of direct and structural violence as well as different gendered experiences that men, women, and people with diverse gender identities faced during war have rarely been a concern of transitional justice projects ( Fobear, 2014 ; Franke, 2006 ).
In terms of design and procedure, the first decades of transitional justice processes did not provide sufficient participation and representation of women and minorities ( O’Rourke, 2017 ). This led to the reproduction of patriarchal logics and discourses about what transitional justice is for, and what human rights violations and crimes should be addressed and how ( Ní Aoláin, 2012 ). While political violence most suffered by men has been at the center of transitional justice, the systemic violence most commonly experienced by women—such as poverty, internal displacement, lack of access to public infrastructure, and unequal access to land, employment, or education ( Martin de Almagro & Ryan, 2019 )—was not recognized or redressed ( Ní Aoláin, 2009 ; Weber, 2021 ).
While much of an engagement with gender in transitional justice has taken place in scholarship evidenced through a growing body of literature (see Fobear, 2014 ; Franke, 2006 ; Ní Aoláin, 2012 ; O’Rourke, 2013 ), there are also legal, normative, and political developments that have addressed gender and transitional justice. Much of this policy engagement is unfolding within the realms of the United Nations Security Council and its mandate to maintain international peace and security, and specifically under the umbrella of the U.N. Women, Peace, and Security (WPS) framework ( Martin de Almagro, 2017 ). As a result of intensive efforts by a transnational coalition of women’s movements and feminist organizations, the agenda specifically calls for increased representation of women in decision making at all levels in the prevention, management, and resolution of conflict; the protection of women’s rights in conflict; the prevention of violence against women in conflict; and the importance of gender-sensitive humanitarian assistance, relief, and recovery ( Aroussi, 2011 ). Under this mandate, the WPS agenda also specifically engages with gender and transitional justice, which comprises a vast set of tools to fight against gender injustices ( Martin de Almagro, 2017 ). For instance, United Nations Security Council Resolution (UNSCR) 1888 focused on access to justice; the rule of law, legal; and judicial reforms; investigations; and prosecutions specifically for victims of wartime sexual violence. UNSCR 2106 specifically asked to punish sexual violence in conflict, and UNSCR 2242 recommended “reparation for victims as appropriate” ( United Nations Security Council, 2015 , p. 7), while reminding that the Security Council can enact sanctions against those who commit conflict-related sexual violence. The Global Study on the Implementation of UNSCR 1325 also called on the United Nations and its member states to “prioritize the design and implementation of gender sensitive reparations programs with transformative impact” ( UN Women, 2015 , p. 124).
Similarly, the resolution of the U.N.’s Human Rights Council that in 2011 established the mandate of the Special Rapporteur on Truth, Justice, Reparation, and Guarantees of Non-Recurrence—through which much of the U.N.’s engagement with transitional justice unfolds—specifically referred to gender, emphasizing that the Special Rapporteur must integrate gender lenses throughout its work (see O’Rourke, 2017 ). Outside the realm of the United Nations, the monitoring Committee of the Convention and Elimination of All Forms of Violence Against Women (CEDAW) similarly developed normative guidance in gender and transitional justice. As Catherine O’Rourke observed, “the Committee’s General Recommendation Number 30 on the rights of women in conflict prevention, conflict and post-conflict situations calls on state parties to address transitional justice mechanisms as part of broader activities to ensure women’s access to justice” ( O’Rourke, 2017 , p. 125). However, the U.N. Special Rapporteur was only established in 2011 , and the CEDAW general recommendation 30 was adopted in 2013 , signaling how TJ as a matter of international peace and security in general, as well as attention to gender and TJ specifically, has become increasingly mainstreamed since the early 2010s.
Gendering Transitional Justice Instruments
As a result of these cumulative efforts, then, gender lenses have been increasingly incorporated into and applied to the different aspects, mechanisms, and instruments of transitional justice, as reviewed throughout this section, structured along retributive and criminal justice, truth-seeking efforts, reparations, and bottom-up TJ mechanisms.
Retributive Justice and Criminal Courts
Much of the engagement with gender in transitional justice unfolds within the context of criminal courts and tribunals, with an emphasis on responding to wartime sexual violence through criminal accountability and retributive justice ( Aroussi, 2011 ; Campbell, 2004 ; Schulz & Kreft, 2022 ). This emphasis on criminal justice thereby mirrors larger trends in TJ, whereby criminal retribution and legal punishment still often are seen as ultimate responses to crimes ( Fletcher & Weinstein, 2002 ).
Since the late 1990s and early 2000s, notable progress has been made toward an engagement with gender in international criminal law ( Chappell, 2011 ). Progressive developments by the International Criminal Tribunal for the former Yugoslavia (ICTY) and for Rwanda (ICTR) in the 1990s contributed toward the recognition of crimes of rape and sexual violence as constitutive of war crimes, crimes against humanity, and genocide ( Mibenge, 2013 ). Throughout the literature, these two ad hoc tribunals are generally credited with the responsibility for the contemporary evolution of jurisprudence on conflict-related sexual violence ( Haffajee, 2006 ), and are seen as having established landmark and precedence cases concerning sexual violence.
These developments also set the precedent for other hybrid tribunals—such as the Special Courts for Sierra Leone (SCSL) and the Extraordinary Chambers in the Courts of Cambodia (ECCC)—as well as the permanent International Criminal Court (ICC), which has heard several cases that include charges of sexual and gender-based violence (SGBV; Chappell, 2014 ). Since 2014 , prosecuting gender-based violence (GBV) has been among the ICC’s Office of the Prosecutor’s (OTP) key strategic goals, reflected in the “Policy Paper on Sexual and Gender-Based Crimes.” Since then, as of 2018 , 16 out of 23 cases pending at the International Criminal Court have included charges of SGBV. This process of ensuring accountability for conflict-related sexual violence (CRSV) is important, and has “contributed toward documenting the patterns and dynamics of sexual violence” ( Schulz & Kreft, 2022 , p. 7) across contexts, in addition to contributing to the development of international jurisprudence on sexual violence. At the same time, testifying in a court of law about their experiences of sexual abuse may for some survivors be healing, empowering, and a “cathartic process that equips them with a sense of agency and enables them to articulate their voices” ( Schulz & Kreft, 2022 , p. 13; see also Mertus, 2004 ).
Yet, despite growing attention, the track record of actually delivering justice for sexual violence survivors remains limited. And while the ICC’s conception of SGBV has broadened over the years to also include crimes of forced marriage and pregnancy alongside sexual torture or crimes of rape, the emphasis remains on sexual violence over other forms of gendered violence and discrimination. What is more, despite only a handful of exceptions, most proceedings involving sexual violence at international courts have focused on women survivors, but have tended to sideline sexual violence against men or against persons with diverse SOGIESC ( Schulz, 2020 ). Influenced by and in tandem with these developments in the international criminal justice arena, and in the interest of complementarity, there also is a growing collection of cases concerning CRSV at national and domestic courts—including for instance the Bosnian War Crimes Chamber, or courts in Guatemala, El Salvador, or the Democratic Republic of Congo ( Seelinger, 2020 ).
Despite much of this progress of investigating and prosecuting crimes of sexual violence, however, the existing caseload of successful convictions remains limited at best. This in many ways mirrors the “justice gap” for SGBV that persists not only in (post)conflict settings but more widely across time and space ( McGlynn & Westmarland, 2019 ). In addition, feminist scholars in particular have identified various legal, political, technical, and gendered shortcomings of criminal proceedings. As such, Houge and Lohne (2017) have cautioned that treating CRSV simply as “a problem of law” overlooks more structurally-engrained forms of violence and discrimination, as well as potential alternative justice conceptions and mechanisms. A growing body of scholarship has also identified more practical limitations, evidencing victims’ and survivors’ dissatisfaction with criminal justice processes ( Henry, 2009 ). This body of work takes note of the fact that many survivors feel “footnoted” in the proceedings, silenced, deprived of any agency ( Mertus, 2004 ), or revictimized ( Franke, 2006 ; see Schulz & Kreft, 2022 ). Focused on the ICTY, Mertus showed that women’s agency during criminal proceedings was severely stunted, and that survivors of wartime rape who participated in criminal trials often felt “like [they were] shouting from the bottom of a well” ( Mertus, 2004 , p. 113). Drawing on an analysis of the SCSL, Kelsall and Stepakoff (2007) similarly showed how women who participated in the trials “were prohibited from speaking about the principal manner in which they were victimized [sexually] during the conflict” (p. 365), and how as a result, women’s experiences were removed from the Court’s records (see Mibenge, 2013 ). As such, “experience[s] of giving testimony [are] likely to be mixed” ( Henry, 2009 , p. 114), leading feminist scholars to question whether criminal proceedings constitute adequate means to deliver accountability for GBV ( Henry, 2009 ; Mertus, 2004 ; Otto, 2009 ).
Truth and Reconciliation Commissions
As an alternative to some of these structural limitations with regards to criminal justice, an emphasis on restorative justice, often in the form of Truth and Reconciliation Commissions (TRCs), has gained growing popularity over the decades—perhaps most notably in South Africa as well as across Latin America. In their broadest terms, truth (and reconciliation) commissions are entities that seek to establish facts, causes, and impacts of past human rights violations with a focus on victims’ and survivors’ testimonies, thereby seeking to provide recognition of harm and suffering.
The first Truth Commissions in Argentina, Peru, Guatemala, and South Africa did not include gendered harms in their terms of reference; but were instead focused on political crimes to the exclusion of ordinary and structural violence. In these proceedings, women’s testimonies were primarily limited as witnesses of harms committed between men. This had consequences not only for the lack of recognition of violence against women, but also for the ensuing policy recommendations and reparations identified as necessary in the TRC reports. As Sanne Weber (2021) noted, “Truth Commissions have historically tended to leave out women’s particular conflict experiences” (p. 214).
The South African Truth and Reconciliation Commission ( 1996–2003 ), established to deal with human rights violations of the apartheid system, was the first to adopt ad hoc gender-sensitive strategies such as holding special women’s hearings, creating gender-sensitive statement-taking protocols, and adding a chapter on women in the final report ( Fiske, 2019 ). After sustained advocacy from key women activists and even though it had not been part of the original plan, the Peru Truth and Reconciliation Commission ( 2001–2003 ) established a specific Gender Unit in charge of examining gendered and sexual patterns of violence, training staff on gender-sensitive approaches to truth and reconciliation, and leading a public hearing on women’s human rights. The Commission’s final report devoted two individual chapters to a gendered analysis of the conflict and the use of sexual violence against women. Nevertheless, the lack of an appropriate budget to support the activities of the Gender Unit prevented it from achieving much and many Peruvian activists saw it as a lost chance for a more systematic and transformative approach for enhancing women’s access to justice ( Nesiah et al., 2006 ).
Later TRCs included a focus on gender in their mandates and tried to actively understand how violence and oppression are gendered ( Bell & O’Rourke, 2007 , p. 28). In particular, the Truth Commissions of Sierra Leone ( 2002–2004 ) and East Timor ( 2002–2005 ) are regarded as best practices. Their reports in 2004 and 2005 included a stand-alone chapter on gender and sexual violence, as well as recommendations for reparations ( Nesiah et al., 2006 ). Furthermore, the Sierra Leone TRC’s procedures for engagement with women were also gender-sensitive. First, it proactively looked for women testimonies, offering material support and counseling for those willing to testify. Second, women could choose whether to provide written or oral testimony and whether to testify at an open or closed hearing. Third, the Commission trained specialized women statement takers to work with sexual violence victims. In general terms, Truth Commissions have been criticized for overtly focusing on sexual violence, and for not taking into consideration how women often face the socioeconomic consequences of conflicts. In the context of the Sierra Leone TRC (SLTRC), however, sexual violence and abuse were the terms of reference under which women could testify as victims, and even though the SLTRC was determined “to capture the experiences of both women and girls in respect of sexual violence, as well as their complete gendered experiences at a political, legal, health and social welfare level” ( Sierra Leone Truth and Reconciliation Commission, 2004 , p. 87), the commission’s final report focused mainly on rape and other sexual violence crimes committed against women during the conflict. As such, both truth commissions and courts have been criticized for their singled-issue focus on sexual violence at the expense of the complex nature of gender violence in conflict-affected settings.
In addition to these formalized and institutionalized truth commissions, more informal and/or grassroots-level, truth-seeking, and historical memory processes have evolved across a number of conflicts, including most prominently the Gacaca courts in Rwanda ( Bronéus, 2008 ), but also Colombia’s National Centre for Historical Memory , and the National Memory and Peace Documentation Centre (NMPDC) in Uganda. These and similar efforts across contexts document and preserve conflict-related experiences and enable survivors to share their experiences in often more informal processes, thereby at times offering more space for diverse stories. At the same time, these informal efforts are also often structured around heteronormative conceptions of gender, thereby restricting the space of what experiences can be openly talked about, and have also been experienced as retraumatizing and threatening by women giving testimony ( Bronéus, 2008 ). This mirrors shortcomings of criminal tribunals as discussed in the subsection “ Retributive Justice and Criminal Courts ,” and of bottom-up transitional justice mechanisms as discussed in the section “ Reparations .”
Reparations
Reparations are typically portrayed to be among the most victim-centric elements of transitional justice ( Hamber, 2008 ). As emphasized by de Greif, reparations provide financial or other material compensations, such as property restitution as a form of corrective justice, obliging the wrongdoer to provide goods to the victim so that the latter find themselves in the original position before the harm ( de Greiff, 2008 , p. 435). In practice and implementation, the U.N. Basic Principles and Guidelines on the Right to a Remedy and Reparation ( 2005 ) lists five components of reparations: (a) restitution, (b) compensation, (c) rehabilitation (including access to medical and psychological care), (d) satisfaction and, (e) guarantees of nonrepetition. Importantly, reparations not only imply material gains for survivors, but crucially “can be profoundly meaningful to victims or survivors at a psychological level” ( Hamber, 2008 , p. 8). In this reading, reparations can be individual and/or collective, and material and/or symbolic ( Hamber & Palmary, 2009 ) as well as prospective and retrospective.
For the most part, however, reparations programs are not “designed with an explicit gender dimension in mind” ( Rubio-Marín et al., 2006 , p. 23), nor have they “focused on the forms of victimization that women are more commonly subject to,” including forms of CRSV. As Ní Aoláin et al. (2015) observed, global discussions aimed at ensuring accountability and ending impunity for CRSV have largely neglected and marginalized reparations.
However, reparations have been increasingly linked to sexual and gender-based violence. In March 2007 , international legal and gender experts and women survivors of sexual violence met in Nairobi (Kenya) to draft the Nairobi Declaration on the Right of Women and Girls to a Remedy and Reparation. The declaration is key because it sought to redefine reparations from a gendered perspective that makes visible the linkages between direct and structural violence. The declaration had two core principles: First, reparations should be transformative, go to the root causes of gender violence, and “must go above and beyond the immediate reasons and consequences of the crimes and violations; they must address structural inequalities that negatively shape women’s and girls’ lives” (Nairobi Declaration, supra n 3, Principle 3[h]). The second core principle is the participation and involvement of women at all stages of the planning, design, and implementation of reparations programs because the involvement of women in the reform of social structures will also lead to recognition and to political empowerment.
This emphasis on structural discrimination and transformation thereby speaks to some conceptual shortcomings of reparations, as well as a recent emphasis on transformational reparations within a broader shift from transitional to transformative justice ( Gready & Robins, 2019 ). As suggested by the Nairobi Declaration, a gender perspective indeed reveals that if reparative justice and reparations aim to quite literally repair conflict-related harms ( Hamber, 2008 ), this can potentially translate into a reconstitution of an unequal preconflict status quo (see Ní Aoláin et al., 2015 ; Rubio-Marín & de Greiff, 2007 ). In transitional and (post)conflict settings, this frequently implies a reparation of and return to hetero-patriarchal societal structures, characterized by vast gendered inequalities and the systematic discrimination of women ( Goldblatt & Meintjes, 2011 ). Rather than transforming unequal gendered and intersectional structures—which may have given rise to conflict and violence in the first place—reparations thus risk reinstating that status quo, thus reinstating patriarchy.
Since then, there has been growing attention within scholarship and policymaking ( Duggan et al., 2008 ; Ní Aoláin et al., 2015 ; Walker, 2016 )—evidenced for instance through the Global Survivors Fund, founded by the 2018 Nobel Peace Prize laureates Nadia Murad and Dr. Denis Mukwege, which seeks to enhance access to reparations for survivors of CRSV. In particular, the United Nations Secretary-General’s adoption of a Guidance Note on Reparations for Conflict-Related Sexual Violence ( 2014 ) marked an important turning point in the area of reparations for SGBV ( Ní Aoláin et al., 2015 ). At the same time, several of the U.N. Security Council resolutions that make up the WPS agenda, such as Resolution 2122 , repeatedly refer to reparations in response to gender-based violence.
This process of repairing preconflict structures specifically for women can often imply a return to an unequal gendered status quo ante and to inferior female subject positioning ( Buckley-Zistel, 2013 ). Rubio-Marín and de Greiff (2007) therefore urged that reparations programs need to ensure that they do “not conform to or contribute to the entrenchment of pre-existing patterns of female land tenure, education or employment” (p. 325). Further, most reparations programs primarily concentrate on civil and political rights, at the expense of other violations, including socioeconomic rights, many of which are often heavily gendered ( Rubio-Marín, 2009 ), thereby mirroring gendered trends and shortcomings in transitional justice more broadly ( Boesten & Wilding, 2015 ; O’Rourke, 2013 ).
As such, there are, as of 2022 , a handful of cases of reparations for gender-based crimes, for instance in the War Crimes Chambers in Bosnia ( Björkdahl & Selimovic, 2015 ), and by national courts in Sierra Leone and Guatemala, where “an urgent reparation scheme awarded one-off payments for survivors of sexual violence, together with medical treatment” ( Weber, 2021 , p. 221). In Guatemala, apart from the individual compensation to victims of rape in the case of Sepur Zarco, the judges ordered the construction of a health clinic in the village and the creation of an education scholarship fund for women and girls. In Mexico, the European Court for Human Rights (ECHR) and Inter-American Court of Human Rights (IACHR) and its “Cotton Field” judgement on femicide cases have contributed precedent-setting cases for the award of reparations in response to gender violence and harms ( Rubio-Marín & Sandoval, 2011 ) and, more precisely, for the development of gender-just transformation processes ( Ketelaars, 2018 ). As explained by Sane Weber (2021) , the Cotton Field judgement “stated that when violations were committed in a context of structural discrimination, reparations should aim to transform this pre-existing situation” (p. 222).
Colombia adopted a transformative approach to reparations and land restitution in its 2011 Victims’ Law. Since land titles are in their majority in men’s names, the Law provides for the allocation of joint land titles to men and women as a way to ensure a better social and economic security in case of divorce or of the husband’s death and in this way transforms gender inequality. In practice, however, transforming attitudes toward women and agricultural work are difficult to achieve and the agricultural projects that have accompanied land restitution in Colombia have focused on men’s agricultural work and have devalued women’s work as just family work to “help make ends meet” ( Weber, 2021 ), reinforcing rather than ending gender inequalities. What is more, most reparations programs globally focus on female victims at the neglect of male survivors and persons with diverse SOGIESC ( Schulz, 2020 ). As noted by Ní Aoláin et al. (2015) , “a limited understanding of who can be a victim of sexual harms means that violence against men is often unseen and unaccounted for when states and other international actors conceive and implement reparations” (p. 97). Challenges therefore remain to ensure that reparations can address the gendered manifestations of violence in their holistic occurrence, and that reparations can cement real gendered progress, in particular for conflict-affected women ( Rubio-Marín & de Greiff, 2007 ) as well as for sexual violence survivors of all genders ( Duggan et al., 2008 ; Ní Aoláin et al., 2015 ; Schulz, 2020 ).
In light of these conceptual and practical gaps of implementing reparations in response to gendered harms and violence, several scholars have emphasized that “a commitment to transformative reparations is critical to gender-sensitive reparations” ( Ní Aoláin et al., 2015 , p. 98; see also Kettelaars, 2018 ; Walker, 2016 ).Transformative reparations, especially in the context of redressing gendered violence, require “go[ing] beyond the immediacy of sexual violence, [and] encompassing the equality, justice and longitudinal needs of those who have experienced sexual harms” ( Ní Aoláin et al., 2015 , pp. 98–99).
Bottom-Up Transitional Justice Mechanisms
In the absence of concrete, tangible results for specific crimes committed against women, an array of civil society-led and locally-embedded mechanisms have seen the day. Much of this growing attention to processes at the grassroots and micro level is embedded within the so-called “local turn” in transitional justice ( Shaw & Waldorf, 2010 ), which has also increasingly engaged with gender ( Baines, 2010 ; Kent, 2014 ). As an illustrative example of such bottom-up initiatives, women’s tribunals have constituted a collective effort at putting women’s experiences of war and violence at the center of truth, justice, and reparation processes necessary to rebuild more gender just societies. In Kosovo, Albano–Kosovar women created an initiative of legal support for victims of sexual violence through the Kosovo Women’s Network, and joined forces with the Serb Women in Black Network Serbia to create the Women Peace Coalition on May 7, 2006 ( Kosovo Women’s Network, 2013 ). Together, they participated in the Women’s Tribunal, a regional initiative of restorative justice led by women survivors of conflict in Yugoslavia ( Mujika Chao, 2017 ).
In Northern Uganda, too—the context in which one of the authors primarily works—a variety of civil society-supported and locally-driven processes exist to deal with past human rights abuses ( Baines, 2007 ). While such processes catalyze a sense of justice on the micro level, in the absence of sufficient processes at the state or international level, however, such processes nevertheless also contain gendered challenges. In many conflict-affected societies—frequently characterized by masculine, patriarchal, and heteronormative constructions of gender—a turn to the local simultaneously often implies a geographical move toward, and a reinforcement of, largely masculinized, homophobic, and sexually conservative societal contexts, which raises challenges for the participation of and roles played by women and youths. For instance, Boege (2006) described how women and girls are often excluded from the administration of these measures and only “become the subjects of these decisions” (p. 16). In Northern Uganda, “the most visible proponents of traditional justice and the most visible participants in the ceremonies are male elders” ( Lonergan, 2012 , p. 1)—excluding women (and youth) from active roles and instead only passively subjecting them to these processes. With regard to the application of justice, Baines (2007) consequentially argued that “it is unlikely that mato oput [one of the most common traditional justice rituals] will be able to reflect [women’s] interests without significant modification” (p. 107).
In addition to gendered participation and involvement, a localization of justice likewise carries implications for the treatment of gendered conflict-related experiences, including women’s structural inequalities and crimes of sexual violence against women and men. In many conflict-affected societies, a localization of transitional justice measures likely implies that taboo and culturally stigmatized crimes of sexual violence against men fall outside the realm and framework of local means of delivering justice ( Schulz, 2020 ).
Feminist Critiques of Transitional Gender Justice
In light of this overview, and against the background of many of these shortcomings and gaps of extant approaches to gender and transitional justice as discussed in the section on “ Gendering Transitional Justice Instruments ,” feminist scholars, activists, and practitioners in particular have articulated profound and resounding critiques of transitional gender justice—which constitute the focus of discussion in this section. In particular, feminist perspectives on justice have argued that violence cannot be understood as separate, single acts, but rather as a continuum—as a manifestation of structural inequality and gendered power relations ( Braithwaite & D’Costa, 2018 ). Therefore, these perspectives have criticized transitional justice mechanisms’ focus on “extraordinary” violence during a specific historical moment—from the war declaration to the signature of a peace accord. They have argued that this focus renders invisible the complexities of individual and collective war experiences ( Bunch, 1990 ; Rao, 2001 ). This, in turn, impairs women’s access to justice ( Fiske, 2019 ). At the same time, a persistent focus of most TJ processes on women as passive, vulnerable victims overlooks and downplays the active roles and agency exercised by women in (post)conflict and transitional settings ( Björkdahl & Selimovic, 2015 ), thereby reinforcing essentialist gender stereotypes of female victimhood ( Enloe, 2000 ).
The Experiences of Violence
The differentiation between extraordinary and ordinary violence does not reflect women’s lived experiences during war and in postwar justice efforts and socioeconomic restructuring processes. First, this distinction has resulted in the reinforcement of harmful tropes about sexual violence committed in “ordinary” circumstances in conflict and postconflict settings ( Grewal, 2015 ) and has not addressed rapes and sexual violence committed by peacekeepers, (civilian) men from the same ethnic group, or from the victims’ own families and communities, or any other circumstances than those considered as rape as a strategic weapon of war perpetrated by enemy armed soldiers ( Fiske & Shackel, 2014 ).
Second, this false and binary differentiation between ordinary and extraordinary also ignores the fact that wartime violence is not only physical and direct, but rather is inherently relational and takes many forms, and that these cannot be separated in lived experiences ( Hozić & True, 2017 ). This is due to the fact that acts of violence are “dynamically connected through social, political and economic factors in the surrounding context” ( Krause, 2015 , p. 16). For example, many women become widowed during war and as a result are dispossessed of land and other resources in patrilinear societies ( Shackel & Fiske, 2016 ), are excluded from social life ( Yadav, 2016 ), and are vulnerable to further violence due to their precarious economic situation ( True, 2012 ). In addition, war also blurs the boundaries between production and social reproduction because violent conflict pushes both productive and reproductive activities into private spaces. For example, families need to go into subsistence production to access food and other basic goods; there is an absence of social or public spaces for childcare, healthcare, and the elderly; and the gendered, classed, and racial patterns of everyday violence get exacerbated by militarization and economic collapse ( Elias & Rai, 2019 ; Rai et al., 2019 ). Furthermore, this socioeconomic violence tends to be reproduced in postwar economic and political reforms by the national and the international community.
The Continuum of Violence
Feminist activists and scholars have pointed out that while sexual violence and rape during war have been recognized as crimes against humanity and war crimes, the persistence of physical, sexual, and gender-based violence in the aftermath of conflict is barely given any attention. Nevertheless, the consequences of war, such as a militarized society, impoverishment, unemployment, and posttraumatic stress disorder, as well as men’s feelings of inability to fulfill their perceived gender roles as providers and protectors of their families often lead to domestic and sexual violence ( El Bushra, 2003 ; Ní Aoláin et al., 2011 ; Rubio-Marín, 2009 ).
Furthermore, the focus on sexual violence has ignored that gendered violence takes many forms. For example, the lack of access to social services and infrastructure results in women taking the burden of reproductive work, while often being the only bread winners in separated or destroyed families. Ultimately, feminist have argued for a long time that in contexts of war and peace, transitional justice is “brought” to war-torn countries by the international community ( Nagy, 2014 , p. 217). However, looking at injustices and conflict-related violence also entails accounting for the role that international financial institutions and their postwar reconstruction projects play in reproducing wartime gender-based violence and preexisting economic inequalities through their politics of privatization, liberalization, and austerity ( Lai, 2020 ). The lack of a serious engagement with the socioeconomic legacies of the war and the justice claims deriving from it provokes the sidelining of access to health services, education, and job market policies to the benefit of macrostructural reforms and reconstruction projects of roads, airports, and other transport infrastructure ( Manjoo & McRaith, 2011 ; Martin de Almagro & Ryan, 2019 ; Ní Aoláin et al., 2011 ; Rubio-Marín, 2009 ).
Crucially, the justice model envisioned in liberal peacebuilding reforms often excludes redistributive demands as security and justice are defined in a state-centric manner ( Ní Aoláin, 2009 ), where the reintegration of the state in global markets provide further economic exploitation and exclusion of women through the reestablishment of traditional gender roles and feminized low-paying jobs ( Sassen, 2000 ). These concerns have evolved toward larger debates on redistributive policies and the role of states and markets in postconflict economies. Lai (2020) explained how postwar countries such as Bosnia-Herzegovina with a socialist past had social services available to support social reproduction while women were at work. These services disappeared once International Financial Institutions (IFIs) reconstructed the country according to liberal standards, entrenching gendered inequalities and injustices that the war brought with it. While women lost their jobs in the factories, had difficult access to food and water during wartime, and were responsible for the survival of the household, the IFIs reconstruction project did not redress but rather reproduced wartime socioeconomic violence. The transition post-Apartheid period in South Africa also marked a case in point: the South African government started implementing neoliberal policies that negatively affected black people in general, and women’s economic and social conditions in particular ( Hunter, 2007 ).
Feminist Solutions to Achieve Transformative Justice
In light of these dynamics, feminist analytical lenses underscore the continuities between (gendered) public and private violence; distinctions between prewar, war, and postwar violence; and physical to structural violence and inequalities ( Boulding, 1984 ; Enloe, 2000 ; Tickner, 1992 ; True, 2012 ). Such feminist takes contend that gender justice can only happen through the direct and substantive participation by ordinary people, and in particular conflict-affected women and girls ( Rees & Chinkin, 2015 ). Taking their participation seriously, these scholars have argued, will result in a broadening of transitional justice’s scope to include economic, social, and cultural rights ( Nagy, 2014 ; Rees & Chinkin, 2015 ). Feminist scholars thus have claimed that TJ measures should reflect transformative understandings of justice directed at ensuring that gender-based violence will not happen again and at tackling the inequalities, marginalizations, and exclusions that underlie and fuel wars ( Cohn & Duncanson, 2020 ; True & Hozić, 2020 ).
Therefore, for justice to be transformative, transitional justice mechanisms must also operate hand in hand with postwar reforms ( Lai, 2020 ; Martin de Almagro & Ryan, 2019 , 2020 ). As argued, many of the underpinning components of transformative justice, such as a commitment to challenge unequal status quos and structural (often gendered) inequalities as well as a prioritization of socioeconomic rights (see Sharp, 2013 ), have long been advocated for by feminist scholars (see Cockburn, 2008 ). In particular, “for women, periods of societal transition have to aim for the transformation of the underlying inequalities that provided the conditions in which [their] specifically gendered harms were possible” ( Boesten & Wilding, 2015 , p. 1); see also ( Davies & True, 2017 ). As outlined by Ní Aoláin (2019) , transformation and transformative (gender) justice “depend on the redistribution of formal and informal power” and a feminist “commitment to profoundly recalibrate power relationships” ( Ní Aoláin, 2019 , p. 150; also see Enloe, 2000 ). In this capacity, transformative reparations and remedies to conflict-related violations of socioeconomic or “subsistence” rights ( Arbour, 2007 ; Sankey, 2014 ) carry important implications for feminist projects of gender justice and women’s equality in transitional justice in particular ( Boesten & Wilding, 2015 ).
Inclusive Gender: Integrating Masculinities and Queer Perspectives on Transitional Justice
Despite this vastly growing and diversifying engagement with gender in the study of transitional justice, the dominant conceptualization of “gender” in transitional contexts effectively remains an incomplete and exclusive one. Indeed, discussions about gender and TJ often circle around how transitional processes can advance “gender justice” for female victims of violence ( Boesten & Wilding, 2015 ) and for women survivors of wartime sexual violence in particular ( Aroussi, 2011 ). According to these prevailing understandings, “gender” is often synonymous with “women,” and conflict-related experiences are only considered “gendered” when they represent and reinforce “the unequal position of women in society” ( Pillay, 2007 , p. 317). As argued by feminist anthropologist Kimberly Theidon (2007) , in transitional justice, “from gender hearings to gender units and gender-sensitive truth commissions, ‘adding gender’ is policy-speak for ‘adding women’” (p. 353). To illustrate, the implementation of transitional justice measures put forward in several resolutions of the WPS agenda also primarily understand “gender” as “women.” For example, the 2010 U.N. Secretary-General report on the implementation of UNSCR 1325 included both the “number and percentage of transitional justice mechanisms called for by peace processes that include provisions to address the rights and participation of women and girls in their mandates” and the “number and percentage of women and girls receiving benefits through reparation programs, and types of benefits received” ( United Nations Secretary General, 2010 , p. 48).
Without a doubt, owing to the pervasive and structural discrimination of women in conflict-affected and transitional settings globally and the marginalization of women’s perspectives and experiences throughout TJ scholarship and praxis, such a focus remains urgently needed ( O’Rourke, 2017 ). Yet, despite this importance, such a focus also reinforces the on-going exclusion of masculinities and queer perspectives throughout international relations (IR) and conflict research at large, and within the fields of peacebuilding and transitional justice in particular ( Bueno-Hansen, 2018 ; Duriesmith, 2016 ; Fobear, 2014 ; Hagen, 2016 ; Schulz et al., 2023 ). In fact, specific masculinities perspectives and careful consideration for men’s and boys’ experiences as gendered—as well as for the lived realities of persons with diverse sexual orientations, gender identities and expressions, and sex characteristics (SOGIESC; Daigle & Myrttinen, 2018 )—remain omitted from most gendered TJ analyses. This has slowly begun to change, and emerging critical research has increasingly called for attention to masculinities and SOGIESC questions in transitional justice scholarship ( Bueno-Hansen, 2018 ; Fobear, 2014 ; Hamber, 2016 ; Theidon, 2009 ). Yet, as one of the authors cautioned previously, “these few studies thus far exist primarily in silos, and are often characterized by an often unitary focus on either masculinities or sexual and gender minorities” ( Schulz, 2019 , p. 692).
Masculinities Perspectives
In their broadest sense, masculinities are socially constructed gender norms, specifically referring to the multiple ways of “doing male” within and across societies. The foundational work by R. W. Connell (1995) in particular teaches us about the multiplicities and variations of masculinities (in plural) as well as about the inherent power relations within and between masculinities and gender hierarchies more widely. Since the early 2000s, a growing body of literature has begun to pay critical attention to masculinities and their relations to and positioning in the global gender order ( Connell & Messerschmidt, 2005 ), and specifically in relation to armed conflicts ( Duriesmith, 2016 ). However, while a “fairly substantial amount of literature has been generated over the years regarding the forms of masculinity that emerge in times of armed conflict and war” ( Ní Aoláin et al., 2011 , p. 231), this has not yet sufficiently travelled toward postconflict and transitional contexts, with only few exceptions ( Hamber, 2016 ; Theidon, 2009 ). Tracing the marginalization of these intersections over a decade, Hamber (2007 , 2016 ) attested that masculinities perspectives in TJ scholarship presently find themselves in an embryonic state and are only gradually emerging. This is not to suggest, however, that TJ scholarship does not incorporate the voices and views of men. On the contrary, and as convincingly argued by feminist scholars, TJ can largely be seen as inherently dominated by masculine values and actors ( O’Rourke, 2017 ). What remains underdeveloped, however, is careful consideration for men’s experiences as gendered .
If and when there is engagement with masculinities in TJ contexts, this often unfolds against the backdrop of a violation-centric lens. That is, emerging research on masculinities and TJ focuses either on violent and militarized masculinities, so the violations they perpetrate; or on masculine vulnerabilities, and specifically on sexual violence against men, so the (sexual) violations perpetrated against men. A primary concern of this existing literature has centered around questions of how to disarm and transform violent masculinities in postconflict and transitional periods ( Cahn & Ní Aoláin, 2010 ), for instance through disarmament, demobilization, and reintegration (DDR) programming ( Theidon, 2009 ). This focus is underpinned by the argument that facilitating transitions from conflict to peace requires that militarized masculinities—embodied by (former) combatants—are successfully transformed. As Cahn and Ní Aoláin (2010) argued, one of the central quandaries for TJ and DDR processes “is how to undo the [violent] masculinities learned during wartime” and its wake (p. 118). Research by Theidon (2009) similarly centralized the importance of sustainably mobilizing former combatants to respond to the security challenges posed by them, as well as to the perceived loss of masculine privilege that often attends such processes. Theidon (2009) argued that “transforming the hegemonic, militarized masculinities that characterize former combatants can help further the goals of both DDR and transitional justice processes [. . .] to contribute to building peace on both the battlefield and the home front” (p. 34).
At the same time, however, previous research has also acknowledged the complexities and difficulties of these transformation processes due to the ways in which these masculinities constructions are socially embedded within patriarchal and nationalistic societal structures. In many ways, this focus on militarized masculinities is reflective of dominant research on men and masculinities within the context of war and insecurities more broadly, which has mostly examined the “violences of men” ( Hearn, 1998 ) and the linkages between certain forms of masculinities and the various forms of violence associated with them ( Myrttinen et al., 2017 ).
Another angle through which an engagement with masculinities has unfolded is based on attention to men’s vulnerabilities, and in particular to sexual violence against men and boys (SVAMB). For a long time, men’s experiences of sexual violence were often overlooked and “tailored intervention to address male-centred sexual harms remains exclusive and marginalized” ( Ní Aoláin et al., 2015 , p. 109). In practical terms, despite a handful of cases involving sexual violence against men in the international criminal justice arena, and in the context of some truth and reconciliation commissions (TRC) in Latin America, TJ instruments have thus far almost entirely turned a blind eye to the experiences of sexually violated men ( Schulz, 2020 ).
Despite this prevailing marginalization of sexual violence against men, emerging scholarship has begun to explore how socially constructed masculinities render men vulnerable to gender-based violence in the first place and how sexual violence impacts male survivors’ gendered identities as men in myriad ways ( Myrttinen et al., 2017 ; Schulz, 2020 ). Accordingly, there has also been some attention to the intersections between SVAMB and TJ in the form of growing engagement with the ways in which male survivors conceptualize justice in postconflict settings ( Schulz, 2020 ). Focused specifically on Northern Uganda, previous research by one of the authors has begun to highlight male survivors’ gender-specific justice needs and conceptions ( Schulz, 2019 , 2020 ), as well as how numerous gendered, cultural, and sociopolitical barriers often uphold a vacuum of justice and persisting impunity for those crimes committed against most male survivors of sexual violence globally. Paying attention to male survivors’ lived realities and their justice-related concerns, needs, and priorities is important to address some of the persisting gendered gaps and blind spots.
However, what arguably still requires further examination are the experiences of noncombatant and nonmilitarized civilian men, who arguably constitute the majority of men during most armed conflicts globally, as well as nonheterosexual masculinities, which are still largely rendered invisible by heteronormative frames of conflict and TJ ( Schulz et al., 2023 ). As such, a much needed avenue for further engagement is to consider “how hidden masculine cultures operate within a variety of hierarchies and social spaces ( Hamber, 2016 , p. 30).
Queer Perspectives
Paying sustained attention to masculinities, however, also bears the risk of reinforcing binary constructions of gender, which have been remarkably consistent throughout the study of armed conflict ( Sjoberg, 2016 ). To avoid this, careful consideration for gender and sexualities as fluid spectrums, for the elasticity of gender, as well as the inclusive recognition of people with diverse sexual orientations, gender identities, and expressions and sex characteristics (SOGIESC) is important to fully comprehend gendered understandings of conflicts and political transitions. These nonbinary experiences and perspectives, however, are only seldom taken into account in the context of conflict studies and peacebuilding in general ( Hagen, 2016 ) and in relation to transitional justice processes specifically ( Bueno-Hansen, 2018 ; Fobear, 2014 ). As summarized by McQuaid (2017) , “on the subject of the particular justice needs and harms experienced by sexual minorities, much current transitional justice scholarship remains silent” (p. 1). Katherine Fobear (2023) similarly attested that even though the field of transitional justice has grown substantially, including with regard to incorporating gender, the question of “what it would mean to better incorporate and engage with queer bodies and theory in transitional justice is still very relevant today” (p. 2; also see Fobear, 2014 ). Queer and queering in the context of this discussion serves as an umbrella term to recognize a variety of expressions, identities, and actions that disrupt cis-heteronormative frames based on strict and binary conceptions of gender and sexualities.
It would, however, be misleading to claim that there has been no movement within the field of TJ to queer it, thanks to critical interventions from scholars and activists alike ( Fobear, 2023 ). Many of these developments can be observed in relation to truth commissions ( Bueno-Hansen, 2023 ; Fobear, 2014 ) as well as processes of dealing with the past in Latin American contexts, “some of which have expanded their purview to include human rights investigations of violence against sexual and gender minorities” ( Schulz, 2019 , p. 701; see also Bueno-Hansen, 2018 ). Colombia in particular serves as a contemporary example of the precedent-setting work for the inclusion of persons with diverse SOGIESC and their experiences into TJ processes ( Oettler, 2019 ), for instance with the 2011 Victim’s and Land Restitution Law and its Victim’s Unit, which include “a differential approach that recognizes sexual orientation and gender identity” ( Bueno-Hansen, 2018 , p. 5). In Ecuador, too, a feminist-informed and gender inclusive approach contributed toward “a holistic understanding of sexual and gender-based violence,” including attention to violence against persons with diverse SOGIESC in the Truth Commission’s final report ( Bueno-Hansen, 2023 , p. 2).
However, to queer transitional justice processes, it is not enough to only address antiqueer violence directed against LGBTQI communities and people with diverse SOGIESC, but also to address and critically interrogate larger systems of homophobia, transphobia, patriarchy, and heteronormativity ( Bueno-Hansen, 2018 ; Fobear, 2023 ). To this end, critical scholars have argued for the need of queer, intersectional, and decolonial approaches ( Bueno-Hansen, 2018 ; Ní Aoláin & Rooney, 2007 ) that expose “how institutionalized categories and identities are used to regulate and socialize” ( Fobear, 2023 , p. 6), and that would contribute toward circumventing the neoliberal and heteronormative foundations of TJ. In combination, this triangulation of queer, intersectional, and decolonial analytical lenses to examine queer lived realities can challenge the hetero- and cis-normativity of the field ( Bueno-Hansen, 2018 ; Hagen, 2016 ), and can thus contribute toward a more inclusive understanding of gender in the context of TJ. Nevertheless, across time and space, states’ accountability to address systematic forms of violence against persons with SOGIESC and to push for greater inclusion remains severely limited—consequentially requiring further engagement and advocacy to push the conversation forward by focusing on greater engagement across different spheres and for a variety of populations in transitional settings ( Fobear, 2023 ).
Ways Forward: Toward More Comprehensive and Inclusive Conceptions of “Gender” and “Justice”
This article has offered an overview of transitional (gender) justice mechanisms and their limitations and has put forward questions as to whether transitional justice and its “formulaic approach” ( Rees & Chinkin, 2015 , p. 1211) can ever succeed in changing women’s and other marginalized population’s lives. Without a doubt, much progress has been made in gendering transitional justice processes, and gendered harms have received increasing attention in the international policy arena. However, several shortcomings persist in effectively addressing gendered conflict-related experiences and in advancing transformations for women. When it comes to the implementation of transitional justice, all too often gender remains an afterthought, and is often implemented through a typical “add women and stir” approach—which in turn falls short in fully understanding the ways in which gender permeates all aspects of social and political life, including of armed conflicts and political transitions.
In light of these limitations and shortcomings, then, more needs to be done to address gender in postconflict and transitional spaces. This includes a move beyond transitional justice toward transformative justice, for instance in the form of transformative reparations to ultimately address gendered and patriarchal structures and root causes of violence and conflict and contribute toward more gender-just societal structures. Gendering transitional justice also requires going beyond a conflation of “gender” with “women,” to instead fully consider the full spectrum and elasticity of gender in the form of paying more sustained attention to masculinities and queer experiences and perspectives. To gain a more complete picture of gender in transitional justice and to ultimately advance this progress in practical turn, relational, intersectional, de-colonial and queer approaches are required that take into account the ways in which gender intersects with other identities and forms or exclusions and discrimination. Such approaches, then, also hold the potential to move beyond neoliberalized notions of justice (and gender) that dominate the study and practice of transitional justice, and to instead think of justice in more relational and creative terms.
- Arbour, L. (2007). Economic and social justice for societies in transition. NYU Journal of Law and Politics , 40 (1), 1–28.
- Aroussi, S. (2011). “Women, peace and security”: Addressing accountability for wartime sexual violence. International Feminist Journal of Politics , 13 (4), 576–593.
- Arthur, P. (2009). How “transitions” reshaped human rights: A conceptual history of transitional justice. Human Rights Quarterly , 31 (2), 321–367.
- Baines, E. (2007). The haunting of Alice: Local approaches to justice and reconciliation in Northern Uganda. International Journal of Transitional Justice , 1 (1), 91–114.
- Baines, E. (2010). Spirits and social reconstruction after mass violence: Rethinking transitional justice. African Affairs , 109 (436), 409–430.
- Bell, C. (2009). Transitional justice, interdisciplinary and the state of the “field” or “non-field.” International Journal of Transitional Justice , 3 (1), 5–27.
- Bell, C. , & O’Rourke, C. (2007). Does feminism need a theory of transitional justice? An introductory essay. International Journal of Transitional Justice , 1 (1), 23–44.
- Björkdahl, A. , & Selimovic, J. M. (2015). Gendering agency in transitional justice. Security Dialogue , 46 (2), 165–182.
- Boege, V. (2006). Traditional approaches to conflict transformation: Potentials and limits . Berghof Foundation.
- Boesten, J. , & Wilding, P. (2015). Transformative gender justice: Setting an agenda. Women’s Studies International Forum , 51 , 75–80.
- Boulding, E. (1984). Focus on: The gender gap. Journal of Peace Research , 21 (1), 1–3.
- Braithwaite, J. , & D’Costa, B. (2018). Cascades of violence. War, crime and peacebuilding across South Asia . ANU Press.
- Bronéus, K. (2008). Truth-telling as talking cure? Insecurity and retraumatization in the Rwandan Gacaca Courts. Security Dialogue , 39 (1), 55–76.
- Buckley-Zistel, S. , & Stanley, R. (2012). Gender in transitional justice . Palgrave Macmillan.
- Buckley-Zistel, S. (2013). Redressing Sexual Violence in Transitional Justice and the Labelling of Women as ‘Victims’. In Bonacker, Thorsten / Safferling, Christoph (Eds.), Victims in Transitional Justice, The Hague: T. C. M. Asser Press, pp. 91-100.
- Bueno-Hansen, P. (2015). Feminist and human rights struggles in Peru: Decolonizing transitional justice . University of Illinois Press.
- Bueno-Hansen, P. (2018). The emerging LGBTI rights challenge to transitional justice in Latin America. International Journal of Transitional Justice , 12 (1), 126–145.
- Bueno-Hansen, P. (2023). What can transitional justice do about the heterosexual system? The Ecuadorian Truth Commission’s feminist informed gender approach. In P. Schulz , B. Hamber , & H. Touquet (Eds.), Masculinities and queer perspectives in transitional justice (pp. 158–171). Intersentia.
- Bunch, C. (1990). Women’s rights as human rights: Towards a re-vision of human rights. Human Rights Quarterly , 12 (4), 486–498.
- Cahn, N. , & Ní Aoláin, F. D. (2010). Gender, masculinities and transition in conflicted societies. New England Law Review , 44 , 101–122.
- Campbell, K. (2004). The trauma of justice: Sexual violence, crimes against humanity and the International Criminal Tribunal for the former Yugoslavia. Social & Legal Studies , 13 (3), 329–350.
- Chappell, L. (2011). Nested Newness and Institutional Innovation: Expanding gender justice in the International Criminal Court. In M. L. Krook & F. Mackay (Eds.), Gender, politics, and institutions (pp. 163–180). Palgrave McMillan.
- Chappell, L. (2014). “New,” “old,” and “nested” institutions and gender justice outcomes: A view from the International Criminal Court. Politics & Gender , 10 (4), 572–594.
- Cockburn, C. (2008). From where we stand: War, women’s activism and feminist analysis . Bloomsbury.
- Cohn, C. , & Duncanson, D. (2020). Whose recovery? IFI prescriptions for postwar states. Review of International Political Economy , 27 (6), 1214–1234.
- Connell, R. W. (1995). Masculinities (2nd ed.). University of California Press.
- Connel, R. W. , & Messerschmidt, J. (2005). Hegemonic masculinity: Rethinking the concept. Gender & Society , 19 (6), 829–859.
- Daigle, M. , & Myrttinen, H. (2018). Bringing diverse sexual orientation and gender identity (SOGI) into peacebuilding policy and practice. Gender & Development , 26 (1), 103–120.
- Davies, S. , & True, J. (2017). When there is no justice: Gendered violence and harm in post-conflict Sri Lanka. The International Journal of Human Rights , 21 (9), 1320–1336.
- de Greiff, P. (2008). The handbook of reparations . Oxford University Press.
- de Greiff, P. (2012). Theorizing transitional justice. Nomos , 51 , 31–77.
- Duggan, C. , Paz y Paz Bailey, C. , & Guillerot, J. (2008). Reparations for sexual and reproductive violence: Prospects for achieving gender justice in Guatemala and Peru. International Journal of Transitional Justice , 2 (2), 192–213.
- Duriesmith, D. (2016). Masculinity and new war: The gendered dynamics of contemporary armed conflict . Routledge.
- El Bushra, J. (2003). Fused in combat: Gender relations, and armed conflict. Development in Practice , 13 (2–3), 252–265.
- Elias, J. , & Rai, S. (2019). Feminist everyday political economy: Space, time, and violence. Review of International Studies , 45 (2), 201–220.
- Enloe, C. (2000). Manoeuvres . University of California Press.
- Enloe, C. (2004). The curious feminist. Searching for women in a new age of empire . University of California Press.
- Fiske, L. (2019). The rise (and fall?) of transitional gender justice: A survey of the field. In R. Shackel & L. Fiske (Eds.), Rethinking transitional gender justice (pp. 17–36). Palgrave MacMillan.
- Fiske, L. , & Shackel, R. (2014). Ending rape in war: How far have we come? Cosmopolitan Civil Societies Journal , 6 (3), 123–138.
- Fletcher, L. E. , & Weinstein, H. M. (2002). Violence and social repair: Rethinking the contribution of justice to reconciliation. Human Rights Quarterly , 24 (3), 573–639.
- Fobear, K. (2014). Queering truth commissions. Journal of Human Rights Practice , 6 (1), 51–68.
- Fobear, K. (2023). Queering transitional justice: Reviewing the field of transitional justice and looking towards queer possibilities. In P. Schulz , B. Hamber , & H. Touquet (Eds.), Masculinities and queer perspectives in transitional justice (pp. 121–131). Intersentia.
- Franke, K. M. (2006). Gendered subjects of transitional justice. Columbia Journal of Gender and Law , 15 (3), 813–828.
- Goldblatt, B. , & Meintjies, S. (2011). Dealing with the aftermath: Sexual violence and the Truth and Reconciliation Commission. Agenda , 13 (36), 7–18.
- Gready, P. , & Robins, S. (2014). From transitional to transformative justice: A new agenda for practice. International Journal of Transitional Justice , 8 (3), 339–361.
- Gready, P. & Robins, S. (Eds.) (2019). From Transitional to Transformative Justice. Cambridge: Cambridge University Press.
- Grewal, K. (2015). International criminal law as site for enhancing women’s rights? Challenges, possibilities, strategies. Feminist Legal Studies , 23 (2), 149–165.
- Haffajee, R. L. (2006). Prosecuting crimes of rape and sexual violence at the ICTR: The application of joint criminal enterprise theory. Harvard Journal of Law and Gender , 29 , 201–222.
- Hagen, J. (2016). Queering women, peace and security. International Affairs , 92 (2), 313–332.
- Hamber, B. (2007). Masculinity and transitional justice: An exploratory essay. International Journal of Transitional Justice , 1 (3), 375–390.
- Hamber, B. (2008). Narrowing the micro and the macro. In P. de Greiff (Ed.), The handbook of reparation s (pp. 560–588). Oxford University Press.
- Hamber, B. (2016). There is a crack in everything: Problematising masculinities, peacebuilding and transitional justice. Human Rights Review , 17 (1), 1–25.
- Hamber, B. , & Palmary, I. (2009). Gender, memorialization and symbolic reparations. In R. Rubio-Marín (Ed.), The gender of reparations. Unsettling sexual hierarchies while redressing human rights violations (pp. 324–380). Oxford University Press.
- Hearn, J. (1998). The violences of men: How men talk about and how agencies respond to men’s violence to women . SAGE.
- Henry, N. (2009). Witness to rape: The limits and potential of international war crimes trials for victims of wartime sexual violence. International Journal of Transitional Justice , 3 , 114–134.
- Houge, A. , & Lohne, K. (2017). End impunity! reducing conflict-related sexual violence to a problem of law. Law and Society Review , 51 (4), 755–789.
- Hozić, A. , & True, J. (2017). Brexit as a Scandal: Gender and global Trumpism. Review of International Political Economy , 24 (2), 270–287.
- Hunter, M. (2007). The changing political economy of sex in South Africa: The Significance of unemployment and inequalities to the scale of the AIDS pandemic. Social Science and Medicine , 64 (3), 689–700.
- Kelsall, M. S. , & Stepakoff, S. (2007). “When we wanted to talk about rape”: Silencing sexual violence at the Special Court for Sierra Leone. International Journal of Transitional Justice , 1 (3), 355–374.
- Kent, L. (2014). Narratives of suffering and endurance: Coercive sexual relationships, truth commissions and possibilities for gender justice in Timor-Leste. International Journal of Transitional Justice , 8 (2), 289–313.
- Ketelaars, E. (2018). Gendering Tunisia’s transition: Transformative gender justice outcomes in times of transitional justice turmoil? International Journal of Transitional Justice , 12 (3), 407–426.
- Kosovo Women’s Network . (2013). Women in Black Network Serbia, KWN form Women’s Peace Coalition .
- Krause, U. (2015). A continuum of violence? Refugee Survey Quarterly , 34 (4), 1–19.
- Lai, D. (2020). What has justice got to do with it? Gender and the political economy of post-war Bosnia and Herzegovina. Review of International Political Economy , 27 (6), 1257–1279.
- Lonergan, K. (2012). Gender and generation in Acholi traditional justice mechanisms (JRP Field Note XVII). Justice and Reconciliation Project.
- Manjoo, R. , & McRaith, C. (2011). Gender-based violence and justice in conflict and post-conflict areas. Cornell International Law Journal , 44 , 11.
- Martin de Almagro, M. (2017). Transitional justice and women, peace and security: A critical reading of the EU framework [LSE Women, Peace and Security Working Paper Series (5/2017)]. Centre for Women Peace and Security, London School of Economics and Political Science.
- Martin de Almagro, M. , & Ryan, C. (2019). Subverting economic empowerment: Towards a postcolonial-feminist framework on gender (in) securities in post-war settings. European Journal of International Relations , 25 (4), 1059–1079.
- Martin de Almagro, M. , & Ryan, C. (2020). Introduction: (Re)integrating feminist security studies and global political economy: Continuing the conversation through empirical perspectives. Politics & Gender , 16 (3).
- McEvoy, K. (2007). Beyond legalism: Towards a thicker understanding of Transitional Justice. Journal of Law and Society , 34 (4), 411–440.
- McGlynn, C. , & Westmarland, N. (2019). Kaleidoscopic justice: Sexual violence and victim-survivors’ perceptions of justice. Social & Legal Studies , 28 (2), 179–201.
- McQuaid, K. (2017). “There is violence across, in all arenas”: Listening to stories of violence amongst sexual minority refugees in Uganda.” The International Journal of Human Right s, 1–22.
- Mertus, J. (2004). Shouting from the bottom of the well the impact of international trials for wartime rape on women’s agency. International Feminist Journal of Politics , 6 (1), 110–128.
- Mibenge, C. S. (2013). Sex and international tribunals: The erasure of gender from the war narrative (1st ed.). University of Pennsylvania Press.
- Mujika Chao, I. (2017). Acción feminista en la resistencia civil noviolenta, guerra y posguerra en Kosovo. In I. Mendia Azkue , G. Guzmán Orellana , & I. Zirión Landaluze , (Eds.), Género y justicia transicional: Movimientos de mujeres contra la impunidad (pp. 33–63). Hegoa.
- Myrttinen, H. , Khattab, L. , & Naujoks, J. (2017). Re-thinking hegemonic masculinities in conflict-affected contexts. Critical Military Studies , 3 (2), 103–119.
- Nagy, R. (2014). Transitional justice as a global project: Critical reflections. In R. Buchanan & P. Zumbansen (Eds.), Law in transition (pp. 215–226). Bloomsbury.
- Nesiah, V. , et al. (2006, July). Truth commissions and gender: Principles, policies, and procedures . International Center for Transitional Justice.
- Ní Aoláin, F. (2009). Women, security and the patriarchy of internationalized transitional justice. Human Rights Quarterly , 31 (4), 1055–1085.
- Ní Aoláin, F. (2012). Advancing feminist positioning in the field of transitional justice. International Journal of Transitional Justice , 6 (2), 205–228.
- Ní Aoláin, F. (2019). Transformative gender justice? In P. Gready & S. Robins (Eds.), From transitional to transformative justice (pp. 150–171). Cambridge University Press.
- Ní Aoláin, F. , Cahn, N. , & Haynes, D. F. (2011). Masculinities and child soldiers in post-conflict societies. In A. McGinley (Ed.), Masculinities and the law. A multidimensional approach (pp. 231–251). New York University Press.
- Ní Aoláin, F. , Haynes, D. F. , & Cahn, N . (2011). On the frontlines: Gender, war, and the postconflict process . Oxford University Press.
- Ní Aoláin, F. , O’Rourke, C. , & Swaine, A. (2015). Transforming reparations for conflict-related sexual violence: Principles and practice. Harvard Human Rights Journal , 28 , 97–146.
- Ní Aoláin, F. , & Rooney. E. (2007). Underenforcement and intersectionality: Gendered aspects of transition for women. International Journal of Transitional Justice , 1 (3), 338–354.
- Oettler, A. (2019). The struggle for gendered peace and LGBT rights in Colombia [Violence, Security and Peace Working Papers]. London School of Economics and Political Science.
- O’Rourke, C. (2013). Gender politics in transitional justice (1st ed.). Routledge.
- O’Rourke, C. (2017). Transitional justice and gender. In C. Lawther , L. Moffett , & D. Jacobs (Eds.), Research handbook on transitional justice (pp. 117–142). Edward Elgar.
- Otto, D. (2009). The exile of inclusion: Reflections on gender issues in international law over the last decade. Melbourne Journal of International Law , 10 (1).
- Pillay, N. (2007). Editorial Note. Special Issue: Gender and transitional justice. International Journal of Transitional Justice , 1 (3), 315–317.
- Rai, S. M. , True, J. , & Tanyag, M. (2019). From depletion to regeneration: Addressing structural and physical violence in post-conflict economies. Social Politics: International Studies in Gender, State & Society , 26 (4), 561–585.
- Rao, A. (2001). Right in the home: Feminist theoretical perspectives on international human rights. In P. Hayden (Ed.), The philosophy of human rights (pp. 505–525). Paragon House.
- Rees, M. , & Chinkin, C. (2015). Exposing the gendered myth of post conflict transition: The transformative power of economic and social rights. New York University Journal of International Law and Politics , 48 , 1211–1226.
- Roht-Arriaza, N. , & Mariezcurrena, J. (Eds.). (2006). Transitional justice in the twenty-first century: Beyond truth versus justice . Cambridge University Press.
- Rubio-Marín, R. (Ed.). (2009). The Gender of reparations: Unsettling sexual hierarchies while redressing human rights violations . Cambridge University Press.
- Rubio-Marín, R. , & de Greiff, P. (2007). Women and reparations. International Journal of Transitional Justice , 1 (3), 318–337.
- Rubio-Marín, R. , de Greiff, P. , & Mayer-Rieckh, A. (Eds.). (2006). What happened to the women? Gender and reparations for human rights violations . International Center for Transitional Justice. Social Sciences Research Council.
- Rubio-Marín, R. , & Sandoval, C. (2011). Engendering the reparations jurisprudence of the Inter-American Court of Human Rights: The promise of the cotton field judgment. Human Rights Quarterly , 33 (4), 1062–1091.
- Sankey, D. (2014). Towards recognition of subsistence harms: Reassessing approaches to socioeconomic forms of violence in transitional justice. International Journal of Transitional Justice , 8 (1), 121–140.
- Sassen, S. (2000). Women’s burden: Counter-geographies of globalization and the feminization of survival. Journal of International Affairs , 53 (2), 503–524.
- Schulz, P. (2019). Towards inclusive gender in transitional justice: Gaps, blind-spots and opportunities. Journal of Intervention and Statebuilding , 14 (5), 691–710.
- Schulz, P. (2020). Male survivors of wartime sexual violence: Perspectives from Northern Uganda . University of California Press.
- Schulz, P. , Hamber, B. , & Touquet, H. (2023). Masculinities and queer perspectives in transitional justice . Intersentia.
- Schulz, P. , & Kreft, A. (2022). Accountability for conflict-related sexual violence. Oxford Research Encyclopedia of International Studies , 1–25.
- Seelinger, K. T. (2020). Close to home. Journal of International Criminal Justice , 18 (2), 219–242.
- Shackel, R. , & Fiske, L. (2016). Making justice work for women. Kenya country report . Sydney University.
- Sharp, D. (2013). Interrogating the peripheries: The preoccupations of fourth generation transitional justice. Harvard Human Rights Journal , 26 , 149–178.
- Shaw, R. , & Waldorf, L. (2010). Localizing transitional justice: Interventions and priorities after mass violence . Stanford University Press.
- Sierra Leone Truth and Reconciliation Commission . (2004). Witness to truth: Report of the Sierra Leone truth and reconciliation commission .
- Sjoberg, L. (2016). Women as wartime rapists: Beyond sensation and stereotyping . New York University Press.
- Sriram, C. (2014). Liberal peacebuilding and transitional justice: What place for socioeconomic concerns? In C. Sriram (Ed.), Justice and economic violence in transition (pp. 27–49). Springer.
- Teitel, R. (2003). Transitional justice genealogy. Harvard Human Rights Journal , 16 , 69–94.
- Teitel, R. (2015). Globalizing transitional justice . Oxford University Press.
- Theidon, K. (2007). Gender in transition: Common sense, women, and war. Journal of Human Rights , 6 (4), 453–478.
- Theidon, K. (2009). Reconstructing masculinities: The disarmament, demobilization, and reintegration of former combatants in Colombia. Human Rights Quarterly , 31 (1), 1–34.
- Tickner, A. (1992). Gender in international relations: Feminist perspectives on achieving global security . Columbia University Press.
- True, J. (2012). The political economy of violence against women . Oxford University Press.
- True, J. , & Hozić, A. (2020). Don’t mention the war! International financial institutions and the gendered circuits of violence in post-conflict. Review of International Political Economy , 27 (6), 1193–1213.
- United Nations General Assembly . (2006). Basic principles and guidelines on the right to a remedy and reparation for victims of gross violations of International Human Rights Law and serious violations of International Humanitarian Law . A/RES160/147.
- United Nations Secretary General . (2010). Women and peace and Security. Report of the Secretary-General . S/2010/498.
- United Nations Security Council . (2015, October 13). United Nations Security Council Resolution 2242 . Adopted by the Security Council at its 7533rd meeting. S/RES12242.
- United Nations’ Special Rapporteur on the Promotion of Truth, Justice, Reparation and Guarantees of Non-recurrence . (2020). Report of the Special Rapporteur on the promotion of truth, justice, reparation and guarantees of non-recurrence, United Nations General Assembly, Seventy-fifth session, Item 72 (b), A/75/174 .
- UNWOMEN . (2015). A Global Study on the implementation of United Nations Security Council Resolution 1325 . Preventing Conflict, Transforming Justice, Securing the Peace.
- Walker, M. (2016). Transformative Reparations? A critical look at a current trend in thinking about gender-just reparations. International Journal of Transitional Justice , 10 (1), 108–125.
- Weber, S. (2021). Gender and transitional justice. In H. Yusuf & H. van der Merwe (Eds.), Transitional justice: Theories, mechanisms and debates (pp. 207–229). Oxford University Press.
- Yadav, P. (2016). Social transformation in post-conflict Nepal. A gender perspective . Routledge.
Related Articles
- Gender, Religion, and International Relations
- Gender and Governance
- Gender Issues in Ethnicity, Nationalism, and Migration
- Gender, Mobility, and Displacement: From the Shadows to Questioning Binaries
- Transitional Justice
Printed from Oxford Research Encyclopedias, International Studies. Under the terms of the licence agreement, an individual user may print out a single article for personal use (for details see Privacy Policy and Legal Notice).
date: 03 July 2024
- Cookie Policy
- Privacy Policy
- Legal Notice
- Accessibility
- [185.80.150.64]
- 185.80.150.64
Character limit 500 /500
Inclusion, Diversity, Equity and Accountability
- IDEA Response to COVID-19 Crisis
- IDEA@Berkeley Lab
- IDEA Strategic Framework
- IDEA Accountability Model
- FY22-FY25 IDEA Strategic Plan
- FY23 Progress Report
- IDEA Key Campaigns
- Sample IDEA Goals for PMP
- IDEAs in Action
- IDEA Office
- IDEA Senior Leadership Council
- IDEA Community of Practice
- Employee Resource Groups
- Current IDEA Working Groups
- Area & Division IDEA Committees
- Berkeley Lab Workforce Demographics
- Visible Spectrum Series
- IDEA Speaker Series
- IDEAs in Action Case Studies
- IDEA FOA Handbook
- Name Change for Published Research Outputs
Gender Identity and Transition in the Workplace
- Equity Reset
- Wellness News & Events
- Family News & Events
- Lab Ambassador Program
- Accessibility Resources
- Women in Science Speaker Series
- Berkeley Lab and TechWomen
- Pathways to Report Misconduct
- Harassment & Discrimination Prevention Policies
- IDEAs-in-Action Workshops
- IDEA Office Newsletters
Gender Identity and Transition Guidelines at Berkeley Lab
At Berkeley Lab, we are committed to conducting great science,fostering technological advancement to solve the world’s most challenging problems, and answering its most elusive questions. Just as science reveals nature’s diversity, science organizations reveal their own nature by the diversity and inclusion they foster. Diversity of people and thought is part of our unique social fabric and a key to our research success. It is also a daily and personal commitment — and an expectation. Each employee has a role to play. Every employee has a responsibility to act. We believe in Berkeley Lab’s mission to share the benefits of scientific discovery with the world. We also respect the differences in our workplace community.
PURPOSE FOR GUIDELINES
This document is intended to delineate guidelines for addressing the needs and issues that may arise in the workplace for any employee seeking to affirm their gender identity and/or planning to initiate or continue their gender transition while working at Berkeley Lab. Employees who are undergoing or plan to undergo some form of gender transition may at some point want or need to involve their supervisor for support and advocacy. Supervisors need to be adequately prepared to assist a transitioning employee at any time.
These guidelines support Berkeley Lab’s Nondiscrimination Policy , which includes gender identity and expression. This document is intended for use by supervisors and employees. If any assistance understanding something in this document is needed, contact the IDEA Office at [email protected] . As with all change, gender transition affects many people – the person transitioning, supervisors, peers, and users. However, it is the responsibility of the employee initiating or continuing their gender transition as well as all supervisors and HR representatives to become and remain informed of these guidelines. These guidelines provide a starting point for building awareness, and are intended to guide and support all parties involved.
POLICY STATEMENT
Berkeley Lab has been and continues to be an advocate for diversity and equal employment opportunities. Every person makes a unique contribution toward establishing Berkeley Lab as a place where people can grow and succeed. We enable these contributions by maintaining a workplace environment that embraces diversity and fosters creativity and innovation. Accordingly, fairness and equity must be defining characteristics of our workplace environment.
Per Berkeley Lab’s Nondiscrimination Policy: “Lawrence Berkeley National Laboratory (Berkeley Lab) is committed to nondiscrimination in employment. The Laboratory does not engage in discrimination against or harassment of any person employed by or seeking employment with the Laboratory on the basis of race, color, national origin, religion, sex, gender, gender expression, gender identity, pregnancy, physical or mental disability, medical condition (cancer-related or genetic characteristics), genetic information (including family medical history), ancestry, marital status, age, sexual orientation, citizenship, or service in the uniformed services (as defined by the Uniformed Services Employment and Re-employment Rights Act of 1994). This policy is intended to be consistent with the provisions of applicable state and federal laws and Laboratory policies. This applies to all personnel actions, including hiring, transfer, training, promotion, termination, and other terms and conditions of employment.”
By providing a work environment of respect, trust, collaboration and cooperation, Berkeley Lab can fulfill its mission of conducting great science and fostering technological advancement. Lab employees who can bring their whole selves to work can thrive in their careers.
- Employee Resource – Gender Identity and Transition in the Workplace
- Supervisor Resource – Gender Identity and Transition in the Workplace
- Gender Transition Plan Worksheet/Checklist
EXTERNAL RESOURCES
The following resources have been compiled for additional information. It should be noted that these resources are not controlled by the Berkeley Lab and may be out of date.
- California Transgender Law 101 : This reference guide is designed to provide a broad overview of California laws affecting transgender people. If you have a question about these laws or other issues your clients are facing, contact the Transgender Law Center.
- ID Please : This comprehensive publication is a guide for navigating processes of updating California and federal identity documents to reflect accurate gender markers. This timely release coincides with the recent change in California law, which simplifies the requirements for a name change.
- State-by-State Overview: Changing Gender Markers on Birth Certificates : Resources for changing gender markers on legal documents.
- Name Changes Laws by State : Resources for changing legal name.
- National Center for Transgender Equality : The National Center for Transgender Equality is the nation’s leading social justice advocacy organization winning life-saving change for transgender people.
- Tips for Allies of Transgender People (compiled by GLAAD) : The following are tips that can be used as you move toward becoming a better ally to transgender people. Of course, this list is not exhaustive and cannot include all the “right” things to do or say – because often there is no one “right” answer to every situation you might encounter. When you become an ally of transgender people, your actions will help change the culture, making society a better, safer place for transgender people – and for all people who do not conform to gender expectations (regardless of gender identity).
- Transgender Law Center : Transgender Law Center works to change law, policy, and attitudes so that all people can live safely, authentically, and free from discrimination regardless of their gender identity or expression. We envision a future where gender self-determination and authentic expression are seen as basic rights and matters of common human dignity.
- Glossary of Terms : A list of terms compiled by the Human Rights Campaign.
- World Professional Association for Transgender Health (WPATH) : WPATH’s mission is to promote evidence based care, education, research, advocacy, public policy, and respect in transgender health. WPATH’s vision is to bring together diverse professionals dedicated to developing best practices and supportive policies worldwide that promote health, research, education, respect, dignity, and equality for transgender, transsexual, and gender-variant people in all cultural settings.

A U.S. Department of Energy National Laboratory Managed by the University of California
Questions & Comments Privacy & Security Notice
- google plus
- Election 2024
- Entertainment
- Newsletters
- Photography
- AP Investigations
- AP Buyline Personal Finance
- AP Buyline Shopping
- Press Releases
- Israel-Hamas War
- Russia-Ukraine War
- Global elections
- Asia Pacific
- Latin America
- Middle East
- Election Results
- Delegate Tracker
- AP & Elections
- Auto Racing
- 2024 Paris Olympic Games
- Movie reviews
- Book reviews
- Financial Markets
- Business Highlights
- Financial wellness
- Artificial Intelligence
- Social Media
Can a marriage survive a gender transition? Yes, and even thrive. How these couples make it work
Avril Clark lived “a double life” for 15 years until her spouse came out as transgender in 2018, changing her name to Lucy and bringing the couple much attention. Avril now runs the group Distinction Support, an online network that helps supportive partners of trans and nonbinary people. (AP video shot by Kwiyeon Ha)
Avril Clark, left, and Lucy pose for a photograph during an interview at their house in London, Tuesday, June 11, 2024. Avril Clark operates the group Distinction Support, a U.K.-based global online network that helps people whose partner went through or is undergoing a gender transition. Her spouse, a British soccer referee at the time, came out publicly as transgender in 2018, changed her name to Lucy and brought the couple much attention. Avril Clark says that until then, they kept their arrangement private and “lived a double life” for 15 years. (AP Photo/Kin Cheung)
- Copy Link copied
Avril Clark, left, and Lucy speak during an interview at their house in London, Tuesday, June 11, 2024. Avril Clark operates the group Distinction Support, a U.K.-based global online network that helps people whose partner went through or is undergoing a gender transition. Her spouse, a British soccer referee at the time, came out publicly as transgender in 2018, changed her name to Lucy and brought the couple much attention. Avril Clark says that until then, they kept their arrangement private and “lived a double life” for 15 years. (AP Photo/Kin Cheung)
Avril Clark, left, and Lucy watch their dogs playing with chickens at their house in London, Tuesday, June 11, 2024. Avril Clark operates the group Distinction Support, a U.K.-based global online network that helps people whose partner went through or is undergoing a gender transition. Her spouse, a British soccer referee at the time, came out publicly as transgender in 2018, changed her name to Lucy and brought the couple much attention. Avril Clark says that until then, they kept their arrangement private and “lived a double life” for 15 years. (AP Photo/Kin Cheung)
Avril Clark, right, and Lucy pet a cat at their house in London, Tuesday, June 11, 2024. Avril Clark operates the group Distinction Support, a U.K.-based global online network that helps people whose partner went through or is undergoing a gender transition. Her spouse, a British soccer referee at the time, came out publicly as transgender in 2018, changed her name to Lucy and brought the couple much attention. Avril Clark says that until then, they kept their arrangement private and “lived a double life” for 15 years. (AP Photo/Kin Cheung)
Marissa Lasoff-Santos and the person she would marry quickly fell head over heels in love. Lasoff-Santos was a gay woman. Her girlfriend was a bisexual woman — or so they thought. Now her partner has become her husband, and they both identify as queer. And things are better than ever.
“We’ve always just had this deep connection, so that’s why, like, I never stopped loving him throughout any of this,” says Lasoff-Santos, a 33-year-old librarian in Michigan. “I’ve become more attracted to him. I guess part of it is just, like, that confidence in him and, like, he just seems so happy.”
Avril Clark, left, and Lucy speak during an interview at their house in London, Tuesday, June 11, 2024. (AP Photo/Kin Cheung)
Lasoff-Santos’ relationship and others like it show that a partner’s gender transition does not necessarily mean a death sentence for a marriage. Data is scant, but couples and therapists say that in many cases, a relationship grows and flourishes under the light of new honesty.
Such marriages, when they do prevail, can underscore the resilience of love, the flexibility of sexual identity and the diversity in LGBTQ+ relationships 20 years after the first same-sex marriages in the U.S. and with Pride Month in its sixth decade.
“Even though he was the one transitioning, I felt like I was going through my own transition,” Lasoff-Santos says. “It was definitely hard to not, I guess, come across as kind of selfish, because I was going through all these emotions, and he was going through his own journey.”
Kristie Overstreet, a sexologist and psychotherapist who says she has worked with trans people for 18 years, says about 2 in 5 relationships survive a transition. And Kelly Wise, a sex therapist in Pennsylvania, estimates that about half of relationships in his practice that experience a gender transition end — for many reasons.
Avril Clark, left, and Lucy pose for a photograph during an interview at their house in London, Tuesday, June 11, 2024. (AP Photo/Kin Cheung)
“Gender identity milestones often arise around times that many things are evolving within people and their relationships,” Wise says in an email.
A recent U.S. Census Bureau report on same-sex households doesn’t reflect marriages in transition because the bureau doesn’t ask questions about gender identity.
Avril Clark operates Distinction Support, an online network that helps supportive partners of trans and nonbinary people. Her spouse, a soccer referee at the time, came out as transgender in 2018, changed her name to Lucy and brought the couple much attention. Before then, Avril says, they had kept their arrangement private and “lived a double life” for 15 years.
“I needed somebody to talk to that knew how I was feeling,” Avril says. “And I looked around, and there weren’t any groups that were for me. They were full of people that were very angry and bitter and didn’t want anybody else’s relationship to work because their relationship hadn’t worked.”
Avril Clark, right, and Lucy pet a cat at their house in London, Tuesday, June 11, 2024. (AP Photo/Kin Cheung)
Lucy Clark says Avril had been pressing her to come out for years, “but I didn’t because I thought it would affect football. And I loved football and had it in my mind that I would give it up.” She didn’t, and she now manages Sutton United Women in south London.
Avril Clark says that when she took over Distinction in 2017, it had about 50 members worldwide, but now there are “way over 500.”
“I’ve got this group with all these people on it, all fighting, some of them fighting to make their relationship work,” she says.
The Reddit group r/mypartneristrans, which describes itself as “a supportive, educational, and safe space for the partners of trans and gender-diverse people,” counts 61,000 members.
Avril Clark, left, and Lucy watch their dogs playing with chickens at their house in London, Tuesday, June 11, 2024. (AP Photo/Kin Cheung)
Topics include questions about how to handle Mother’s Day and Father’s Day; unwelcoming relatives; sex and pregnancy; and how to categorize a cisgender partner’s sexual orientation. In other words, now that I’m a woman married to a woman, does that make me a lesbian?
Clark says some people call themselves “heteroflexible.”
“It doesn’t mean ‘I am a lesbian’ or ‘I’m a gay person,’” she says. “It just means, ‘For this one person I am prepared to be flexible.’”
She estimates her group is 90% cisgender women and 5% transgender or nonbinary people who may also have a partner in transition. The remaining 5% are cisgender husbands, she says.
For people already in a same-sex relationship, a partner’s gender transition can bring angst but also self-discovery.
Lasoff-Santos says she had previously wondered if she could ever be married to a man. “And I always said no. And I think it’s hilarious just now that I am.”
Couples in transition find different ways to address life from “before” — trips, memories, weddings, anniversaries, family events, photos.
“The partner that isn’t transitioning may want to display and still share all of these versus their partner who may not want these visible or talked about,” Overstreet says in an email.
Lasoff-Santos and her husband married in 2018 as he was beginning his transition. They had a son in 2021. When her husband shows their son pictures of himself pre-transition, it’s just “Papa with long hair,” Lasoff-Santos says.
One partner may sense a shift the other does not. Emily Wilkinson, 33, who lives near Seattle, says she doesn’t doubt “that I love Cameron and will continue to love Cameron.” But her vision of their love has changed since her spouse began transitioning last year.
For Cameron, 39, “Our love doesn’t feel any different to me, but I’m not the one who has to adjust in our relationship.” They spoke on the condition that their last name not be used to avoid potential consequences at work, where they are not out.
There can be joy in coaching a partner in their new identity.
Rhiannon Rippke-Koch, 45, lives in a small city in Iowa with Sophia Koch, her recently transitioned wife of the same age. She recalls the first time Sophia got to be herself for a whole weekend, during a trip to Des Moines.
“I took her to Victoria’s Secret and had them measure her for a bra,” Rippke-Koch says. “And I took her to Sephora, and they did, you know, the whole makeup thing where, you know, with color palettes, and showed her how to do her eyeshadow and foundation and all that sort of stuff. So —”
“It was awesome,” Sophia finishes, beaming.
The couple also bond over experiences Sophia previously denied herself because of notions about masculinity — musicals, flowers. Rhiannon says they’re now “much more intimate, and not even in a sexual way. But we talk about things more. We have more things in common now than we did before.”
This story has been corrected to reflect that Marissa Lasoff-Santos now says her son was born in 2021, not 2020.
Associated Press video journalist Kwiyeon Ha contributed to this report.
- Post-Election
What is Project 2025 And Why Is It Alarming?
By Matt Cohen
June 28, 2024

- Share on Facebook
- Share on Twitter
The general election is still about four months away and, with the latest polls showing an incredibly tight race , anything can happen in that time. But that hasn’t stopped former President Donald Trump who, in concert with top Republicans and conservative figures and organizations, already sketched out a plan to reshape the federal government in their image.
The plan is called Project 2025 — a collection of policy transition proposals that outline how, should Trump win the November election, he can vastly remake the federal government most effectively to carry out an extremist far-right agenda.
“It is not enough for conservatives to win elections,” the project’s website states. “If we are going to rescue the country from the grip of the radical Left, we need both a governing agenda and the right people in place, ready to carry this agenda out on day one of the next conservative administration. This is the goal of the 2025 Presidential Transition Project.”
What, exactly, is Project 2025?
Simply put, Project 2025 is a massive, 920-page document that outlines exactly what the next Trump presidency would look like. This doesn’t just include policy proposals — like immigration actions, educational proposals and economic plans — but rather a portrait of the America that conservatives hope to implement in the next Republican administration, be it Trump or someone else. The document is a thorough blueprint for how, exactly, to carry out such a vision, through recommendations for key White House staff, cabinet positions, Congress, federal agencies, commissions and boards. The plan goes so far as to outline a vetting process for appointing and hiring the right people in every level of government to carry out this vision.
The opening essay of the plan, written by Heritage Project President Kevin D. Roberts, succinctly summarizes the goal of Project 2025: a promise to make America a conservative nation. To do so, the next presidential administration should focus on four “broad fronts that will decide America’s future.”
Those four fronts include:
- Restore the family as the centerpiece of American life and protect our children.
- Dismantle the administrative state and return self-governance to the American people.
- Defend our nation’s sovereignty, borders, and bounty against global threats.
- Secure our God-given individual rights to live freely—what our Constitution calls “the Blessings of Liberty.”
The rest of the document sketches out, in detail, how the next Republican administration can execute their goals on these four fronts. That includes comprehensive outlines on what the White House and every single federal agency should do to overhaul its goals and day-to-day operations — from the Department of Agriculture to the Department of Defense, Small Business Administration and Financial Regulatory Agencies. Every sector of the executive branch has a detailed plan in Project 2025 that explains how it can carry out an ultra-conservative agenda.
Project 2025 is supported by the same right-wing groups bringing dozens of anti-democracy lawsuits that will impact the outcome of this year’s election.
Democracy Docket is the only news outlet tracking and reporting on these cases — sign up for our free daily and weekly newsletters to get the latest updates sent straight to your inbox.
Why should we be worried about Project 2025?
As The New Republic notes , Project 2025 is “a remarkably detailed guide to turning the United States into a fascist’s paradise.” The primary document of Project 2025, the magazine explains, lays out what is essentially a “Christian nationalist vision of the United States, one in which married heterosexuality is the only valid form of sexual expression and identity; all pregnancies would be carried to term, even if that requires coercion or death; and transgender and gender-nonconforming people do not exist.”
It’s a terrifying vision of what American life could look like, but what’s most concerning about Project 2025 is its playbook for the first 180 days of a hypothetical second Trump term. “The time is short, and conservatives need a plan,” the playbook states. “The project will create a playbook of actions to be taken in the first 180 days of the new Administration to bring quick relief to Americans suffering from the Left’s devastating policies.”
Among the numerous troubling suggestions laid out in the playbook is a detailed plan to essentially purge the federal workforce of tens of thousands of workers in favor of hiring ones who will adhere to the conservative principles of Project 2025. Paul Dans, a former Trump administration official who’s director of Project 2025’s Presidential Transition Project, told the Associated Press the 180 day transition plan is a “clarion call to come to Washington… People need to lay down their tools, and step aside from their professional life and say, ‘This is my lifetime moment to serve.’”
Much of the 180-Day Playbook reads like a cult’s recruiting pamphlet, explaining how department and agency heads should be vetting potential candidates. “This book is functionally an invitation for you the reader—Mr. Smith, Mrs. Smith, and Ms. Smith—to come to Washington or support those who can,” Dans writes in the intro to the Playbook . “Our goal is to assemble an army of aligned, vetted, trained, and prepared conservatives to go to work on Day One to deconstruct the Administrative State.”
Who’s behind Project 2025?
Project 2025 is the brainchild of The Heritage Foundation , the 50-year-old conservative think tank that’s among the most influential right-wing organizations in the country.
In its nearly half century of existence, The Heritage Foundation has used its resources, influence and money to push its conservative agenda in just about every facet of American life: anti-abortion advocacy , voter suppression , anti-climate policies , and anti-LGBTQ advocacy .
Though The Heritage Foundation organized Project 2025 , the initiative is actually a coalition made up of more than 100 right-wing groups, including notorious groups like America First Legal , the Public Interest Legal Foundation and Moms For Liberty . According to NBC News , a huge web of right-wing dark money groups connected to Project 2025, led by the Leonard Leo-connected Donors Trust, has seen a large bump in donations since the project was announced.
The chapters in the Project 2025 plan and 180-Day Playbook were written by “more than 400 scholars and policy experts from across the conservative movement and around the country,” the group says. That includes former Trump administration officials and notable right-wing figures, like former Acting Secretary of Defense Christopher Miller , former Deputy Secretary of Homeland Security Ken Cuccinelli , and Peter Navarro , a former top trade advisor to Trump.
Read the full 2025 Project plan here.
Gender: The Process Of Transition Essay
Gender is the most important function in our society today. There are some many people out in the world that struggle finding their true identify. Transgender is a term for those who feel different because of their gender. Some people may define the word Transgender differently; some would like to be called Trans, or Transsexual. As a society we need to educate ourselves more on transgender people because it a process of change that impact them mentally, physical and socially.
The Process of Transition “The term transgender is often used as an all-purpose descriptor for a wide range of nonconventional gender identities that include individual’s identified as transsexual, female-to male trans men, male-to-female trans women, gender queer, nongendered, two-spirited, cross dressers, drag queens and drag kings (Robert)”. “A relatively simple definition provided by Brill and Pepper (2008), defines a Trans person as an ‘individual whose gender identity does not match their assigned birth gender.
For example, a transgender child self-identifies as a girl but is biologically male . The term can also be applied to individuals with a history of ‘transitioning sex’, even though they may not have openly identified themselves with any of the previously mentioned gender identities (Robert)”. The beginning process of being transgender is mentally, at a young age a child who is biologically born male of female identifies themselves as something else; even when they don’t understand what that maybe.
The word two- spirted, is how many Trans feel trapped in another person body, and then they beginning to emotional change the way they feel and think. “For example in many traditional American-Indian cultures, transgender individuals were once known as ‘two-spirit’ people who undertook distinctive forms of work and achieved unique status. In contrast, cross-dressing and transgender expression are disapproved of elsewhere by nearly all religious traditions (Robert)”. The life of a transgender mentally can be very dangerous.
Many Trans still develop emotions of not feeling normal or helplessness and feeling out of place. “For instance, acceptance and support, or rejection and marginalization, affect a person’s role in society and their personal relationships in particular. While trans people struggle internally with feelings of not belonging or not fitting into accepted cultural norms, these feelings are often exacerbated by external factors ranging from mild harassment and discrimination to the denial of basic rights and violence that in some cases can result in serious injury or even death (Robert)”. However, existing studies reveal links between minority stress, emotional distress and mental health problems in the general LGBT population (Health Service Executive, 2009; King et al. , 2008; Kuyper & Fokkema, 2009; Meyer, 1995). King et al. (2008) completed a met analysis of 25 studies that investigated mental disorder, suicide and self-harm in LGB people. Results indicated a twofold increase in suicide attempts and significantly higher rates of depression, anxiety disorders and alcohol dependence among LGB participants (Higgin Agnes)”.
When a transgender fully accept who there are they are mentally prepare for the physically part to transitioning. Coming out for Gays, Lesbians and Bisexuals as well as Trans genders is hard. “Hence, outwardly genderconforming transgender individual usually proceed through the development stages of coming out later in life, often following a long period of pre-coming when years of hiding their crossgender feelings take a different kind of toll (Etther)”. Gender reassignment is term that used for sex change for transgender. Gender reassignment (which includes psychotherapy, hormonal therapy and surgery) has been demonstrated as the most effective treatment for patients affected by gender dysphoria (or gender identity disorder), in which patients do not recognize their gender (sexual identity) as matching their genetic and sexual characteristics (Gennario Selvaggi)”.
Gender reassignment is a produce where the genitals or breast, or face gets removed or changed to fit the proper gender. Genital procedures performed for gender dysphoria, such as vaginoplasty, clitorolabioplasty, penectomy and orchidectomy in male-to-female transsexuals, and penile and scrotal reconstruction in female-to-male transsexuals, are the core procedures in gender reassignment surgery. Nongenital procedures, such as breast enlargement, mastectomy, facial feminization surgery, voice surgery, and other masculinization and feminization procedures complete the surgical treatment available (Gennario Selvaggi)”. Recently, the term Transgender has rebirth into society with the shocking revelation of Bruce Jenner coming out as being Transgender.
Bruce Jenner is an Olympic hero that won the gold medal for the decathlon 1976, the world saw him as male leader. In 2015 Bruce Jenner came out to world on national television and announced that he was living a life internal as a Trans women, Jenner shared that he would cross dress in hotel rooms, and in his home. Bruce Jenner who now is called Caitlyn Jenner changed the world and now we’ve become more aware of Transgender people. For Transgender changing their physically appearance is not the only struggle they face; socially they are not treated equally the same as other. The National Transgender Discrimination Survey found that 90% of respondents were harassed or mistreated at work for being transgender or hid who they were to avoid such treatment, and 26% had lost a job because they were transgender (Tuttle)”. Transgender people all around the world are being mistreated and harassed.
“However, transphobia– institutional, societal, and individual-level discrimination against transgender persons–is still pervasive in the United States and elsewhere. It often takes the form of laws, regulations, violence (physical, sexual, and verbal), harassment, prejudices, and egative attitudes directed against transgender persons (PHD and Brte)”. Unfortunately numerous people suffer from transphobia and or hostile towards Trans and make it hard for them at work, school anywhere social or in the media. “Studies have reported that transgender persons lack access to gendersensitive health care and often experience transphobia in health care and treatment. Transgender persons are frequently exposed to violence, sexual assault, and harassment in everyday life, mainly because of transphobia (PHD and Brte)”. The down fall from being socially harassed leads to depression.
Depression is one of the leading causes to several health risk of the LGBT community. “Psychological indicators such as depression and suicidal ideation and attempts have been reported among transgender persons (PHD and Brte)”. “A major mental health problem among both the transgender population and the non-transgender population is depression. It is important to stress, however, that depression is rarely caused simply by having a transgender identity (Bockting, Coleman, and Benner (2007), but more likely arises from external pressures such as isolation (Robert)”.
Over millions of young Trans teens are being killed and committing suicide. “Specific causes of depression among the transgender population include worries about disclosing their gender identity, family rejection, balancing transition costs, social isolation and an inability to settle down with an understanding partner (Robert)”. The everyday lives for Transgender is a struggle mentally, physically, and emotionally. Transiting to another gender has is scuffle, but I’m sure for the Trans it’s a process that there are willing to take.
More Essays
- The Argument About Gender-Neutral Dishroom Research Paper
- Gender Stereotypes Affecting People’s Identity Essay
- Gender Roles In Media Portrayal Of Gender Stereotypes Research Paper
- Sex: The Invisible Boundaries Of Gender Identity Essay
- Ezekiel: Mixed Gender Schools Essay
- Essay On Media And Gender Inequality
- Gender Roles In Moby Dick And The Yellow Wall-Paper
- Gender Construction Essay
- Media Influence On Society’s Perception Of Gender Essay
- Non-Acceptance In Schools Essay

Call for papers | One-day conference on gender economics

FROGEE 2024 Academic Conference: "How does gender matter in the economy"?
The Forum for Research on Gender Economics in Eastern Europe ( FROGEE ) together with the Stockholm Institute of Transition Economics (SITE), is pleased to announce a call for papers for a one-day conference titled “How Does Gender Matter in the Economy?” to be held at the Stockholm School of Economics (SSE).
Conference Date: 2024-12-06 Location: Stockholm School of Economics, Sveavägen 65, 113 83 Stockholm, Sweden
Call for papers
The conference features four keynote speakers, each for a specific thematic area, and we invite submissions of papers in each of these areas, as listed below:
Gender-gaps in the labor market in historical perspective, and the role of policies to close them Keynote speaker: Prof. Barbara Petrongolo , University of Oxford
Do women and men behave differently in economic situations? Keynote speaker: Prof. Muriel Niederle , Stanford University
Beyond the labor-market: Gender gaps in politics Keynote speaker: Prof. Manuel Bagues , University of Warwick
Beyond the labor market: Violence against women Keynote speaker: Prof. Jeffrey Grogger , University of Chicago
Submission Guidelines
Please send a full paper, including the name of all authors and highlighting the potential presenter, at [email protected] by August 31 th , 2024 . Excellent extended abstracts can also be considered. Decisions will be communicated by September 30 th , 2024. Speakers of accepted papers will be offered full refunding of economy-travel expenses and hotel accommodation in Stockholm for up to 2 nights.
Photo: Ink Drop , Shutterstock
related news

Call for papers | The political economy of environmental policy

New research reveals foreign aid's positive impact on female empowerment in Malawi

Pamela Campa receives one of the Christiaan Huygens Reproduction and Replication Prizes

FROGEE and SITE celebrates Nobel prize to Claudia Goldin for her studies on gender inequality in the labor market
IMAGES
VIDEO
COMMENTS
Overview We conducted a systematic literature review of all peer-reviewed articles published in English between 1991 and June 2017 that assess the effect of gender transition on transgender well-being. We identified 55 studies that consist of primary research on this topic, of which 51 (93%) found that gender transition improves the overall well-being of transgender […]
Jamie Lindemann Nelson, PhD is a professor of philosophy at Michigan State University in East Lansing, Michigan. She is also a fellow of the Hastings Center and co-editor of IJFAB: International Journal of Feminist Approaches to Bioethics.Her work on philosophical and bioethical issues sparked by gender and transgender has appeared in the Hastings Center Report, Journal of Bioethical Inquiry ...
References to gender transitions relate to the process through which trans and nonbinary people express their gender as different from social expectations associated with the sex they were assigned at birth. This may include social, legal and medical transitions. ... In this essay, participants are identified as trans men, trans women, or ...
The term 'gender modality' could enable researchers to broaden their horizons. A person's gender identity is their sense of gender at any given time. By contrast, gender modality refers to ...
This essay approaches this by proposing that we counter unhelpful and harmful questions about gender transition by instead reframing these inquires as a question of how transitions become possible. Doing so allows us to set aside both if and why questions of transition. Focusing on how transitions unfold is a concern distinct from what Julia ...
That gender-affirming health care saves lives is clear: A 2018 literature review by Cornell University concluded that 93 percent of studies found that transition improved transgender people's ...
In 2016, a controversial bill was signed in Georgia, banning transgender individuals from using restrooms designated for the sex with which they identify. In the wake of this legislation, Between the (Gender) Lines: The Science of Transgender Identity explored what was known at the time about transgender identity, discussing scientific evidence ...
Gender transition is undertaken with the goal of improving the well-being of people suffering from gender dysphoria (Coleman et al., 2022). ... In this essay, I discuss emerging clinical and research issues related to transition regret and detransition. I begin by describing recent changes in the epidemiology of gender dysphoria ...
This was rooted in a twentieth-century theory called the "inversion hypothesis," which held that the desire to transition one's gender was the manifestation of intense same-sex attraction — basically, an extreme form of homosexuality. ... I published a series of papers documenting that transgender men who are attracted to men do exist ...
Gendered transitions: a review essay Maxine Molyneux Superwomen and the Double Burden: Women's Experience of Change in Central and Eastern Europe and the Former Soviet Union Chris Corrin (ed.), Second Story Press, (Canada) 1992 The Color of Gender: Re-imaging Democracy Zillah R. Eisenstein, University of California Press, (London, Berkeley) 1994
Gender transition is the process of changing one's gender presentation or sex characteristics to accord with one's internal sense of gender identity - the idea of what it means to be a man or a woman, or to be non-binary, genderqueer, bigender, or pangender, or to be agender (genderless). For transgender and transsexual people, this process commonly involves reassignment therapy (which may ...
Gender identity refers to a person's internal sense of being male, female or something else; gender expression refers to the way a person communicates gender identity to others through behavior, clothing, hairstyles, voice or body characteristics. "Trans" is sometimes used as shorthand for "transgender.". While transgender is ...
1 INTRODUCTION. Transgender and nonbinary youths (TNBY) are youths who feel an incongruence between their gender identity and sex assigned at birth, sometimes experiencing distress known as gender dysphoria (American Psychiatric Association, 2022).Transitions, which can alleviate dysphoria, can be social (changes in presentation, such as in hair, name, or pronouns), legal (changes of name or ...
Also, it discusses in gender transition the relation between "the right to self-determination", "the right to delete", and "the right to identity and individuality". Conclusions on the ethical admissibility of the 'right to be forgotten' to control gender-affirming information are presented. Keywords: Ethics, 'Right to be ...
The claimant described a highly traumatic childhood in which she showed many gender-atypical behaviours: 'From the age of 14 she began actively to question her gender identity and started to look at YouTube videos and do research on the internet about gender identity disorder and the transition process' (para. 78). 19
For a minority of trans people, passing is irrelevant. For the vast majority, the desire to pass can at times feel all-consuming and the only metric for judging the success of their transition ...
By Akwaeke Emezi. "However, to be ogbanje is to be categorized other and to bring alterity home in a way that transcends the more ordinary bifurcated 'otherness' of gender. We could even speculate that ogbanje children fall under a third category of gender, of human-looking spirit. This gender is marked from birth—as male and female ...
This essay takes inspiration on a clinical meditation about the suicidal tendencies of analysands lost in "gender disorders" who "find themselves" in a trans identity. Reference will be made to Freud's case of the young homosexual woman and to my work on trans identity as an "act."
Educators are facing wrenching new tensions over whether they should tell parents when students socially transition at school. A student from California felt it was critical for his school to ...
This type of advocacy, she argues, builds on two long-standing tendencies: the habit of thinking of gender transition as primarily a medical process, and the habit of grounding L.G.B.T. civil ...
Gender and Transitional Justice: An Overview. In July 2020, the United Nation's Special Rapporteur on the promotion of truth, justice, reparation, and guarantees of nonrecurrence issued a report on gender perspectives in transitional justice (TJ), which "considers multiple aspects of adopting a gender perspective in transitional justice processes" (United Nation's Special Rapporteur ...
Gender Identity Transition Essay. Topics concerning transgender can be very overwhelming for some. When one thinks of the term transgender, one may think of the process of an individual identifying as the opposite sex. The opposite sex of what he or she was born as. For some, this may involve undergoing surgical procedures or taken hormonal ...
These guidelines support Berkeley Lab's Nondiscrimination Policy, which includes gender identity and expression. This document is intended for use by supervisors and employees. If any assistance understanding something in this document is needed, contact the IDEA Office at [email protected]. As with all change, gender transition affects many ...
Avril Clark operates the group Distinction Support, a U.K.-based global online network that helps people whose partner went through or is undergoing a gender transition. Her spouse, a British soccer referee at the time, came out publicly as transgender in 2018, changed her name to Lucy and brought the couple much attention.
The plan is called Project 2025 — a collection of policy transition proposals that outline how, ... The opening essay of the plan, written by Heritage Project President Kevin D. Roberts, succinctly summarizes the goal of Project 2025: a promise to make America a conservative nation. ... and transgender and gender-nonconforming people do not ...
More than 20 states since 2021 have implemented some form of age restriction on gender transition for minors, citing a dearth of long-term evidence for the efficacy of reducing adverse mental ...
The Process of Transition "The term transgender is often used as an all-purpose descriptor for a wide range of nonconventional gender identities that include individual's identified as transsexual, female-to male trans men, male-to-female trans women, gender queer, nongendered, two-spirited, cross dressers, drag queens and drag kings (Robert)".
The Stockholm Institute of Transition Economics (SITE) and the Forum for Research on Gender Economics in Eastern Europe (FROGEE) are pleased to invite submissions of papers for a one-day conference titled "How Does Gender Matter in the Economy?", to be held in Stockholm, Sweden on December 6th, 2024.